Chapter 15: Special Senses
advertisement

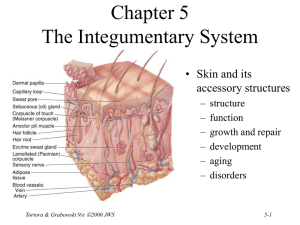
Chapter 15 Sensory, Motor & Integrative Systems • • • • Levels and components of sensation Pathways for sensations from body to brain Pathways for motor signals from brain to body Integration Process – wakefulness and sleep – learning and memory Tortora & Grabowski 9/e 2000 JWS 15-1 Is Sensation Different from Perception? • Sensation is any stimuli the body is aware of – What are we not aware of? • X-rays, ultra high frequency sound waves, UV light – We have no sensory receptors for those stimuli • Perception is the conscious awareness & interpretation of a sensation. – precisely localization & identification – memories of our perceptions are stored in cortex Tortora & Grabowski 9/e 2000 JWS 15-2 Sensory Modalities • Different types of sensations – touch, pain, temperature, vibration, hearing, vision • Each type of sensory neuron can respond to only one type of stimuli • Two classes of sensory modalities – general senses • somatic are sensations from body walls • visceral are sensations from internal organs – special senses • smell, taste, hearing, vision, and balance Tortora & Grabowski 9/e 2000 JWS 15-3 Process of Sensation • Sensory receptors demonstrate selectivity – respond to only one type of stimuli • Events occurring within a sensation – stimulation of the receptor – transduction (conversion) of stimulus into a graded potential • vary in amplitude and are not propagated – generation of impulses when graded potential reaches threshold – integration of sensory input by the CNS Tortora & Grabowski 9/e 2000 JWS 15-4 Sensory Receptors • Selectively respond to only one kind of stimuli • Have simple or complex structures – General Sensory Receptors (Somatic Receptors) • no structural specializations in free nerve endings that provide us with pain, tickle, itch, temperatures • some structural specializations in receptors for touch, pressure & vibration – Special Sensory Receptors (Special Sense Receptors) • very complex structures---vision, hearing, taste, & smell Tortora & Grabowski 9/e 2000 JWS 15-5 Classification of Sensory Receptors • • • • Structural classification Type of response to a stimulus Location of receptors & origin of stimuli Type of stimuli they detect Tortora & Grabowski 9/e 2000 JWS 15-6 Structural Classification of Receptors • Free nerve endings – bare dendrites – pain, temperature, tickle, itch & light touch • Encapsulated nerve endings – dendrites enclosed in connective tissue capsule – pressure, vibration & deep touch • Separate sensory cells – specialized cells that respond to stimuli – vision, taste, hearing, balance Tortora & Grabowski 9/e 2000 JWS 15-7 Structural Classification • Compare free nerve ending, encapsulated nerve ending and sensory receptor cell Tortora & Grabowski 9/e 2000 JWS 15-8 Classification by Response to Stimuli • Generator potential – free nerve endings, encapsulated nerve endings & olfactory receptors produce generator potentials – when large enough, it generates a nerve impulse in a first-order neuron • Receptor potential – vision, hearing, equilibrium and taste receptors produce receptor potentials – receptor cells release neurotransmitter molecules on firstorder neurons producing postsynaptic potentials – PSP may trigger a nerve impulse • Amplitude of potentials vary with stimulus intensity Tortora & Grabowski 9/e 2000 JWS 15-9 Classification by Location • Exteroceptors – near surface of body – receive external stimuli – hearing, vision, smell, taste, touch, pressure, pain, vibration & temperature • Interoceptors – monitors internal environment (BV or viscera) – not conscious except for pain or pressure • Proprioceptors – muscle, tendon, joint & internal ear – senses body position & movement Tortora & Grabowski 9/e 2000 JWS 15-10 Classification by Stimuli Detected • Mechanoreceptors – detect pressure or stretch – touch, pressure, vibration, hearing, proprioception, equilibrium & blood pressure • • • • Thermoreceptors detect temperature Nociceptors detect damage to tissues Photoreceptors detect light Chemoreceptors detect molecules – taste, smell & changes in body fluid chemistry Tortora & Grabowski 9/e 2000 JWS 15-11 Adaptation of Sensory Receptors • Change in sensitivity to long-lasting stimuli – decrease in responsiveness of a receptor • bad smells disappear • very hot water starts to feel only warm – potential amplitudes decrease during a maintained, constant stimulus • Receptors vary in their ability to adapt – Rapidly adapting receptors (smell, pressure, touch) • adapt quickly; specialized for signaling stimulus changes – Slowly adapting receptors (pain, body position) • continuation of nerve impulses as long as stimulus persists Tortora & Grabowski 9/e 2000 JWS 15-12 Somatic Tactile Sensations • Touch – crude touch is ability to perceive something has touched the skin – discriminative touch provides location and texture of source • Pressure is sustained sensation over a large area • Vibration is rapidly repetitive sensory signals • Itching is chemical stimulation of free nerve endings • Tickle is stimulation of free nerve endings only by someone else Tortora & Grabowski 9/e 2000 JWS 15-13 Meissner’s Corpuscle • Dendrites enclosed in CT in dermal papillae of hairless skin • Discriminative touch & vibration-- rapidly adapting • Tortora Generate impulses mainly at onset of a touch & Grabowski 9/e 2000 JWS 15-14 Hair Root Plexus •Free nerve endings found around follicles, detects movement of hair Tortora & Grabowski 9/e 2000 JWS 15-15 Merkel’s Disc • Flattened dendrites touching cells of stratum basale • Used in discriminative touch (25% of receptors in hands) Tortora & Grabowski 9/e 2000 JWS 15-16 Ruffini Corpuscle • Found deep in dermis of skin • Detect heavy touch, continuous touch, & pressure Tortora & Grabowski 9/e 2000 JWS 15-17 Pacinian Corpuscle • Onion-like connective tissue capsule enclosing a dendrite • Found in subcutaneous tissues & certain viscera • Sensations of pressure or high-frequency vibration Tortora & Grabowski 9/e 2000 JWS 15-18 Thermal Sensations • Free nerve endings with 1mm diameter receptive fields on the skin surface • Cold receptors in the stratum basale respond to temperatures between 50-105 degrees F • Warm receptors in the dermis respond to temperatures between 90-118 degrees F • Both adapt rapidly at first, but continue to generate impulses at a low frequency • Pain is produced below 50 and over 118 degrees F. Tortora & Grabowski 9/e 2000 JWS 15-19 Pain Sensations • Nociceptors = pain receptors • Free nerve endings found in every tissue of body except the brain • Stimulated by excessive distension, muscle spasm, & inadequate blood flow • Tissue injury releases chemicals such as K+, kinins or prostaglandins that stimulate nociceptors • Little adaptation occurs Tortora & Grabowski 9/e 2000 JWS 15-20 Types of Pain • Fast pain (acute) – – – – occurs rapidly after stimuli (.1 second) sharp pain like needle puncture or cut not felt in deeper tissues larger A nerve fibers • Slow pain (chronic) – – – – begins more slowly & increases in intensity aching or throbbing pain of toothache in both superficial and deeper tissues smaller C nerve fibers Tortora & Grabowski 9/e 2000 JWS 15-21 Localization of Pain • Superficial Somatic Pain arises from skin areas • Deep Somatic Pain arises from muscle, joints, tendons & fascia • Visceral Pain arises from receptors in visceral organs – localized damage (cutting) intestines causes no pain – diffuse visceral stimulation can be severe • distension of a bile duct from a gallstone • distension of the ureter from a kidney stone • Phantom limb sensations -- cells in cortex still Tortora & Grabowski 9/e 2000 JWS 15-22 Referred Pain • Visceral pain that is felt just deep to the skin overlying the stimulated organ or in a surface area far from the organ. • Skin area & organ are served by the same segment of the spinal cord. – Heart attack is felt in skin along left arm since both are supplied by spinal cord segment T1-T5 Tortora & Grabowski 9/e 2000 JWS 15-23 Pain Relief • Aspirin and ibuprofen block formation of prostaglandins that stimulate nociceptors • Novocaine blocks conduction of nerve impulses along pain fibers • Morphine lessen the perception of pain in the brain. Tortora & Grabowski 9/e 2000 JWS 15-24 Proprioceptive or Kinesthetic Sense • Awareness of body position & movement – walk or type without looking – estimate weight of objects • Proprioceptors adapt only slightly • Sensory information is sent to cerebellum & cerebral cortex – from muscle, tendon, joint capsules & hair cells in the vestibular apparatus Tortora & Grabowski 9/e 2000 JWS 15-25 Muscle Spindles • Specialized intrafusal muscle fibers enclosed in a CT capsule and innervated by gamma motor neurons • Stretching of the muscle stretches the muscle spindles sending sensory information back to the CNS • Spindle sensory fiber monitor changes in muscle length • Brain regulates muscle tone by controlling gamma fibers Tortora & Grabowski 9/e 2000 JWS 15-26 Golgi Tendon Organs • Found at junction of tendon & muscle • Consists of an encapsulated bundle of collagen fibers laced with sensory fibers • When the tendon is overly stretched, sensory signals head for the CNS & resulting in the muscle’s relaxation Tortora & Grabowski 9/e 2000 JWS 15-27 Joint Receptors • Ruffini corpuscles – found in joint capsule – respond to pressure • Pacinian corpuscles – found in connective tissue around the joint – respond to acceleration & deceleration of joints Tortora & Grabowski 9/e 2000 JWS 15-28 Somatic Sensory Pathways • First-order neuron conduct impulses to brainstem or spinal cord – either spinal or cranial nerves • Second-order neurons conducts impulses from spinal cord or brainstem to thalamus--cross over to opposite side before reaching thalamus • Third-order neuron conducts impulses from thalamus to primary somatosensory cortex (postcentral gyrus of parietal lobe) Tortora & Grabowski 9/e 2000 JWS 15-29 Posterior Column-Medial Lemniscus Pathway of CNS • Proprioception, vibration, discriminative touch, weight discrimination & stereognosis • Signals travel up spinal cord in posterior column • Fibers cross-over in medulla to become the medial lemniscus pathway ending in thalamus • Thalamic fibers reach cortex Tortora & Grabowski 9/e 2000 JWS 15-30 Spinothalamic Pathways • Lateral spinothalamic tract carries pain & temperature • Anterior tract carries tickle, itch, crude touch & pressure • First cell body in DRG with synapses in cord • 2nd cell body in gray matter of cord, sends fibers to other side of cord & up through white matter to synapse in thalamus • 3rd cell body in thalamus projects to cerebral cortex Tortora & Grabowski 9/e 2000 JWS 15-31 Somatosensory Map of Postcentral Gyrus • Relative sizes of cortical areas – proportional to number of sensory receptors – proportional to the sensitivity of each part of the body • Can be modified with learning – learn to read Braille & will have larger area representing fingertips Tortora & Grabowski 9/e 2000 JWS 15-32 Sensory Pathways to the Cerebellum • Major routes for proprioceptive signals to reach the cerebellum – anterior spinocerebellar tract – posterior spinocerebellar tract • Subconscious information used by cerebellum for adjusting posture, balance & skilled movements • Signal travels up to same side inferior cerebellar peduncle Tortora & Grabowski 9/e 2000 JWS 15-33 Tertiary Syphilis • Sexually transmitted disease caused by bacterium Treponema pallidum. • Third clinical stage known as tertiary syphilis • Progressive degeneration of posterior portions of spinal cord & neurological loss – loss of somatic sensations – proprioceptive impulses fail to reach cerebellum • People watch their feet while walking, but still uncoordinated and jerky Tortora & Grabowski 9/e 2000 JWS 15-34 Somatic Motor Pathways • Control of body movement – motor portions of cerebral cortex • initiate & control precise movements – basal ganglia help establish muscle tone & integrate semivoluntary automatic movements – cerebellum helps make movements smooth & helps maintain posture & balance • Somatic motor pathways – direct pathway from cerebral cortex to spinal cord & out to muscles – indirect pathway includes synapses in basal ganglia, thalamus, reticular formation & cerebellum Tortora & Grabowski 9/e 2000 JWS 15-35 Primary Motor Cortex • Precentral gyrus initiates voluntary movement • Cells are called upper motor neurons • Muscles represented unequally (according to the number of motor units) • More cortical area is needed if number of motor units in a muscle is high Tortora & Grabowski 9/e 2000 JWS – vocal cords, tongue, lips, fingers & thumb 15-36 Direct Pathway (Pyramidal Pathway) • 1 million upper motor neurons in cerebral cortex – 60% in precentral gyrus & 40% in postcentral gyrus • Axons form internal capsule in cerebrum and pyramids in the medulla oblongata • 90% of fibers decussate(cross over) in the medulla – right side of brain controls left side muscles • Terminate on interneurons which synapse on lower motor neurons in either: – nuclei of cranial nerves or anterior horns of spinal cord • Integrate excitatory & inhibitory input to become final common pathway Tortora & Grabowski 9/e 2000 JWS 15-37 Details of Motor Pathways • Lateral corticospinal tracts – cortex, cerebral peduncles, 90% decussation of axons in medulla, tract formed in lateral column. – skilled movements hands & feet • Anterior corticospinal tracts – the 10% of axons that do not cross – controls neck & trunk muscles • Corticobulbar tracts Tortora & Grabowski 9/e 2000 JWS – cortex to nuclei of CNs ---III, IV, V, VI, VII, IX, X, XI & XII – movements of eyes, tongue, chewing, expressions & speech 15-38 Location of Direct Pathways • Lateral corticospinal tract • Anterior corticospinal tract • Corticobulbar tract Tortora & Grabowski 9/e 2000 JWS 15-39 Paralysis • Flaccid paralysis = damage lower motor neurons – – – – no voluntary movement on same side as damage no reflex actions muscle limp & flaccid decreased muscle tone • Spastic paralysis = damage upper motor neurons – paralysis on opposite side from injury – increased muscle tone – exaggerated reflexes Tortora & Grabowski 9/e 2000 JWS 15-40 Indirect Pathways • All other descending motor pathways • Complex polysynaptic circuits – include basal ganglia, thalamus, cerebellum, reticular formation • Descend in spinal cord as 5 major tracts • All 5 tracts end upon interneurons or lower motor neurons Tortora & Grabowski 9/e 2000 JWS 15-41 Final Common Pathway • Lower motor neurons receive signals from both direct & indirect upper motor neurons • Sum total of all inhibitory & excitatory signals determines the final response of the lower motor neuron & the skeletal muscles Tortora & Grabowski 9/e 2000 JWS 15-42 Basal Ganglia • Helps to program automatic movement sequences – walking and arm swinging or laughing at a joke • Set muscle tone by inhibiting other motor circuits • Damage is characterized by tremors or twitches Tortora & Grabowski 9/e 2000 JWS 15-43 Basal Ganglia Connections • Circuit of connections – cortex to basal ganglia to thalamus to cortex – planning movements • Output from basal ganglia to reticular formation – reduces muscle tone – damage produces rigidity of Parkinson’s disease Tortora & Grabowski 9/e 2000 JWS 15-44 Cerebellar Function Aspects of Function • learning • coordinated & skilled movements • posture & equilibrium 1. Monitors intentions for movements -- input from cerebral cortex 2. Monitors actual movements with feedback from proprioceptors 3. Compares intentions with actual movements 4. Sends out corrective signals to motor cortex Tortora & Grabowski 9/e 2000 JWS 15-45 Wakefulness and Sleep • Circadian rhythm – 24 hour cycle of sleep and awakening – established by hypothalamus • Awake means to be able to react consciously to stimuli • EEG recordings show large amount of activity in cerebral cortex when awake Tortora & Grabowski 9/e 2000 JWS 15-46 Reticular Activating System • RAS has connections to cortex & spinal cord. • Many types of inputs activate the RAS---pain, light, noise, muscle activity, touch • Produces state of wakefulness called consciousness • Coma is sleeplike state – deep coma has no reflexes – death if cardiovascular reflexes are lost Tortora & Grabowski 9/e 2000 JWS 15-47 Sleep • State of altered or partial consciousness from which a person can be aroused • Triggers for sleep are unclear – adenosine levels increase with brain activity – adenosine levels inhibit activity in RAS – caffeine prevents adenosine from inhibiting RAS • Two types of normal sleep – NREM = non-rapid eye movement sleep – REM = rapid eye movement sleep Tortora & Grabowski 9/e 2000 JWS 15-48 Non-Rapid Eye Movement Sleep • Stage 1 – person is drifting off with eyes closed (first few minutes) • Stage 2 – fragments of dreams – eyes may roll from side to side • Stage 3 – very relaxed, moderately deep – 20 minutes, body temperature & BP have dropped • Stage 4 = deep sleep – bed-wetting & sleep walking occur in this phase Tortora & Grabowski 9/e 2000 JWS 15-49 REM Sleep • Most dreams occur during REM sleep • In first 90 minutes of sleep: – go from stage 1 to 4 of NREM, – go up to stage 2 of NREM – to REM sleep • Cycles repeat until total REM sleep totals 90 to 120 minutes • Neuronal activity & oxygen use highest in REM sleep • Total sleeping & dreaming time decreases with age Tortora & Grabowski 9/e 2000 JWS 15-50 Learning & Memory • Learning is acquiring new knowledge • Memory is retaining that knowledge – short-term memory • recall phone number while dialing • depends upon electrical events (reverberating circuits) – long-term memory • frequent retrieval of specific information helps with memory consolidation (learning) • structural or biochemical changes occurs – increase in dendrites, enlarge endbulbs, increase in presynaptic terminals or formation of additional membrane receptors • Recently acquired memory lost first with coma or shock treatments Tortora & Grabowski 9/e 2000 JWS 15-51 Spinal Cord Injury • Damaged by tumor, herniated disc, clot or trauma • Complete transection is cord severed resulting loss of both sensation & movement below the injury • Paralysis – – – – monoplegia is paralysis of one limb only diplegia is paralysis of both upper or both lower hemiplegia is paralysis of one side quadriplegia is paralysis of all four limbs • Spinal shock is loss of reflex function (areflexia) – slow heart rate, low blood pressure, bladder problem – reflexes gradually return Tortora & Grabowski 9/e 2000 JWS 15-52 Cerebral Palsy • Loss of motor control and coordination • Damage to motor areas of the brain – infection of pregnant woman with rubella virus – radiation during fetal life – temporary lack of O2 during birth • Not a progressive disease, but irreversible Tortora & Grabowski 9/e 2000 JWS 15-53 Parkinson Disease • Progressive disorder striking victims at age 60 • Environmental toxins may be the cause • Neurons from the substantia nigra do not release enough dopamine onto basal ganglia – tremor, rigidity, bradykinesia (slow movement) or hypokinesia (decreasing range of movement) – may affect walking, speech, even facial expression • Treatments – drugs to increase dopamine levels, or to prevent its breakdown, surgery to transplant fetal tissue or removal of part of globus pallidus to slow tremors Tortora & Grabowski 9/e 2000 JWS 15-54