Genetics for Maternal Child Health Nursing
advertisement

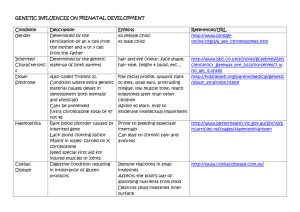
Genetics for Maternal Child Health Nursing Brandy M. Freschi (Smolnik), MS, CGC Certified Genetic Counselor Perinatal Associates of Northern Nevada www.renoperinatal.com Ph 775-829-0573 Fax 775-329-8528 Overview • • • • • Genetic Counselors & Genetic Counseling Prenatal Genetics Neonatal & Pediatric Genetics Pregnancy Loss Grief/Bereavement Genetic Counselors • • • • • Genetic counselors are health professionals with specialized Master’s degrees and experience in the areas of medical genetics and counseling. – Accredited by the American Board of Genetic Counseling; require specific competencies, case load/type, and coursework – Board certification required; Licensure available in only some states Genetic counselors work as members of a health care team, who provide information and support to families who have members with or are at risk for birth defects and/or genetic/inherited disorders by: – Identify families at risk – Investigate the problem present in the family – Interpret information about the disorder – Analyze inheritance patterns and risks of recurrence – Review available testing and treatment options with the family Genetic counselors also: – Provide supportive counseling to families – Serve as patient advocates – Refer individuals and families to community or state support services. – They serve as educators and resource people for other health care professionals and for the general public Settings: – Prenatal, Pediatric/Adult, Cancer, Laboratory, Research, Specialty Disease Clinics, etc. Non-directiveness – Unique from other disciplines/settings in health care – Important because genetics often involves reproductive decisions which are made involving many factors: • Magnitude of risk • Burden of impact of disorder • Individual perception of impact • Meaning of children • Individual cultural, religious or personal preferences Why is Genetics Important in Maternal Child Health Nursing? • Incidence of chromosome abnormalities 1/200 • 40-60% of admissions to children hospitals are for genetic or genetic related conditions • Thousands of genetic conditions exist with new ones discovered regularly • Majority of all deaths have a genetic component Prenatal Genetics Indications for a Genetic Counseling Referral FINDING • Increased risk for aneuploidy – AMA (35-singleton; 33twins) – Positive serum screen – Abnormal ultrasound marker/finding – Family history chromosome abnormality REASON TO CONSIDER CONSULTATION • Discuss risks to pregnancy and available testing options – – – – CVS Amniocentesis 1st or 2nd tri screening Level II ultrasound Aneuploidy • Definition: – The occurrence of one or more extra or missing chromosomes leading to an unbalanced chromosome complement, or, any chromosome number that is not an exact multiple of the haploid number • Most common type of chromosome abnormality • Examples: – Trisomy: one extra chromosome for a total of 47 – Monosomy: one missing chromosome for a total of 45 • Typically not inherited, most trisomies occur due to nondisjunction Case #1 • 37 y, G4P3 • Referred for advanced maternal age (AMA) and first trimester screening • Ultrasound at initial visit revealed fetus had increased nuchal translucency (3.6 mm) • Pt declined FTS and CVS; elected to proceed with amniocentesis after 16 weeks • Results were consistent with trisomy 21 (Down syndrome) Case #1 Trisomy 21: Down syndrome • • • • • • • • Most common aneuploidy, 1/800 births Mental retardation: – Typically mild to moderate but encompasses full range of ability-disability Characteristic facial features Hypotonia Feeding and breathing difficulties Congenital heart defects: – 50% of all affected individuals – Typically AV canal defects Trisomy 21 is not inherited, due to nondisjunction which is a risk for each and every pregnancy at any maternal age Average life span 50-60 http://bagnewsnotes.typepad.com/bagnews/images/Trig1.jpg Nuchal translucency Normal translucency Increased nuchal translucency Down syndrome (Trisomy 21) http://images1.clinicaltools.com/images/ gene/karyotypes/trisomy21.jpg Case #2 • 34 y o, G1P0 • Referred due to abnormal ultrasound findings: choroid plexus cysts, clenched hands, and possible heart defect • Findings above were confirmed also IUGR was noted • Patient was counseled on increase risk for chromosome aneuploidy • Amniocentesis performed and karyotype revealed trisomy 18 (Edwards syndrome) Case #2 Trisomy 18: Edwards Syndrome • • • 1/3000 births IUGR Brain abnormalities – – • • • • CPCs Heart defects Renal abnormalities Dysmorphic features: – – – – • • • • • Hypotonia Seizures Short palpebral fissures Micrognathia Low set ears Clenched fists Cleft lip/palate Rocker-bottom feet Hearing loss Feeding and breathing difficulties High mortality rate: 90% are miscarried or stillborn; 90% die within first year of life (most within the first few days) http://www.ninetynineballoons.com/ Trisomy 18 Case #3 • • • • • 27 y o, G4P2 Referred for first trimester screening Ultrasound revealed a cystic hygroma Pt declined screening and opted for CVS Results were 45,X or Turner syndrome http://www.turnersyndrome.org Case #3 45, X: Turner syndrome • 1/2,500 births • Heart defects – Coarctation of the aorta • Short, webbed neck • Low set ears • Swollen hands and feet • Not associated with MR but may specific learning issues (math, etc) • Short stature • Early loss of ovarian function • Very high miscarriage rate but if liveborn has a very good outlook/prognosis Case #3 Ultrasound Pictures Turner syndrome (45,X) https://images1.clinicaltools.com/images/ gene/karyotypes/turnersyndromexnoy.jpg Prenatal Testing for Aneuploidy • In 2007, the American College of Obstetrics and Gynecology recommend that ALL women regardless of age should be counseled the risk of having a pregnancy with aneuploidy and given the option of both prenatal screening and prenatal diagnosis testing options Modes of Prenatal Screening • • Principles of Prenatal Screening: – Uses various noninvasive tools (maternal serum, ultrasound) to provide a risk assessment for the most common trisomies – It is not able to diagnose these conditions but determines if the patient is at either an increased or normal risk • False positives and false negatives, cannot detect other conditions Types – First trimester screen • 11-14 weeks gestation • Combines maternal age, ultrasound nuchal translucency measurements, evaluation of the nasal bone, and maternal serum levels of PAPP-A and free beta hCG • Provides an adjusted risk for trisomy 21, 18, and 13 (x:xxx chance) • Up to 91-95% detection for trisomy 21; 95% for trisomy 18 & 13 • Does not screen for ONTDs; f/u with serum AFP only and/or u/s in 2nd tri – Second trimester screen (multiple marker; AFP quad, AFP tetra) • 15-20 weeks gestation • Combines maternal age with serum levels of AFP, hCG, unconjugated estriol, and inhibin A • Provides an adjusted risk for trisomy 21, 18, and open neural tube defects (x:xxx chance) • 75-80% detection for trisomy 21; 60% for trisomy 18, and 80-85% for ONTDs – Integrated or Sequential Screening • Combines first & second trimester screening for ~90% detection of DS, 80% for T18 Modes of Prenatal Screening – Non-Invasive Prenatal Diagnosis • Became available in the last year, still under study • Maternal serum screening starting at 10 weeks which evaluating cell-free fetal DNA that circulates in maternal blood and determines the concentration of specifically tagged chromosomes • On average, can detect: – – – – >99% (96-100%) detection of T21 (Down syndrome) 97%-99% (85-100%) of T18 cases 78.6%-91.7% (50-99.9%) of T13 cases Most labs with a <1% false positive rate • Some labs are now including analysis for Turner syndrome & the presence of the Y chromosome • False positives and negatives are still possible, still requires follow up prenatal dx with CVS or amnio – Ultrasound at 18-20 weeks • Examines for markers/signs of chromosome aneuploidy; ONTDs, and other isolated birth defects • Can be somewhat center-dependent • ~50-60% detection for trisomy 21; >90% for trisomy 18, 13 and ONTDS • Anatomy scan by OB; detailed/level II by perinate Modes of Prenatal Diagnosis • Chorionic villus sampling (CVS) – – – – – – • 10-12 weeks gestation Chromosome/genetic/DNA analysis performed on a sample of the chorionic villi 99.9% accuracy/detection of chromosome problems (genetic/DNA testing accuracy/detection is condition-specific) Risk of miscarriage 1/200 No analysis of AFP for ONTDs Performed transabdominally or transcervically Amniocentesis – – – – – 15-20 weeks gestation Chromosome/genetic/DNA analysis performed on a sample on the fetal cells found in amniotic fluid 99.9% accuracy/detection of chromosome problems (genetic/DNA testing accuracy/detection is condition-specific) Risk of miscarriage is as low as 1/1200 or 0.08% Provides 98-99% detection for ONTDs using analysis of amniotic fluid AFP Tests ordered from CVS/Amnio • Karyotype – Gold standard – Karyotype is used to identify and evaluate the size, shape, and number of chromosomes in the fetus – “Photograph” of the chromosomes – Detects 99.9% of all major structural defects (trisomies, translocations, deletions) Tests ordered from CVS/Amnio • FISH (Fluorescent in situ hybridization) – Probes are made to “attach” to a specific region/section of a chromosome – Many utilizations: • Probes for common aneuploidy (allows for rapid detection) • Probes for specific microdeletions/microduplicatons not able to be seen on karyotype Tests ordered from CVS/Amnio • Chromosomal Microarray – Evaluates specific areas (typically 100s of regions) along the human genome for gains or losses of chromosome segments at a much higher resolution than traditional karyotyping – Typically done in cases of abnormal ultrasound findings and/or known family history of microarray abnormalities Indications for a Genetic Counseling Referral FINDING • Family history genetic disease/birth defect/mental retardation AND/OR • Consanguinity REASON TO CONSIDER CONSULTATION • Review pedigree, assess degree of relatedness, discuss recurrence risks, methods of risk reductions, and discuss available testing options The Family History in Genetics • Fundamental component of genetic consultation • Visual record of the family – Clarifying relationships between individual – Allows for sorting of phenotypic features relevant to condition in question – Assists in determining the mode of inheritance if evident • Important in establishing rapport-can learn a lot of nongenetic information from pedigree – Chief support people, social relationships, family “myths” Putting it all together Single Gene Inheritance Autosomal Dominant • Examples: – Huntington Disease – Achondroplasia – Neurofibromatosis type 1 – Marfan syndrome • Some cases in the family will be “de novo” with no previous family hx – Certain diseases are known to have high de novo rates and there is an increased risk with h paternal age Single Gene Inheritance Autosomal Recessive • • • • • Cystic Fibrosis Sickle Cell Disease Thalassemia PKU Galactosemia Increased risk with consanguinity Single Gene Inheritance X-Linked • • • • Hemophilia A & B Duchenne MD Colorblindness Fragile X syndrome Multifactorial Conditions • Examples: – Heart defects • Maternal diabetes, ace inhibitors, lithium – Cleft lip/Cleft palate • Cigarette smoking, folic acid deficiency, maternal medications – Open neural tube defects • Folic acid deficiency, MTHFR, maternal diabetes, anti-seizure medications Indications for a Genetic Counseling Referral FINDING • Preconception/prenatal genetic carrier testing • Environmental Hazards – Maternal viral infection, teratogenic exposures • Maternal conditions putting the fetus at risk – Diabetes, PKU • Infertility/Recurrent pregnancy loss – Translocations; hereditary thrombophilias; patient has genetic/chromosomal condition REASON TO CONSIDER CONSULTATION • Discuss inheritance & testing • Discuss risks to pregnancy & testing • Discuss risks to pregnancy & testing • Discuss various etiologies & offer workup as necessary Carrier Screening • • Screening the population, or particular parts of the population for their risk to have a child with a recessive disorder Traditionally, carrier screening was performed/offered specific to the person’s ethnicity – Since they are recessive conditions, a normal family history does not reduce the chances from general population risks • • • • • 1/25 Europeans are carriers of CF 1/40 Europeans are carriers of SMA 1/12 Africans are carriers of Sickle cell and other hemoglobinopathies 1/9 Ashkenazi Jews are carriers of one of 9 “Jewish” conditions Now, with better and less expensive technology coupled with the fact that people are more often from multiple ethnic backgrounds, “Universal Genetic Carrier Screening” is utilized – Screens for over 100 autosomal recessive genetic conditions – 1/3-1/5 individuals are carriers of these conditions – Same cost as in individual disease carrier test Aim of Counseling Regarding Prenatal Diagnosis • Supply at risk families with information so they can make informed choices regarding pregnancy – Provide a definitive answer for condition in question which allows for: • An accurate diagnosis to provide a prognosis, management, and recurrence risks which allows for family to either continue or end a pregnancy • Providing reassurance to at risk families when result is normal • Allowing couples to prepare psychologically for the birth of an affected child • Helping the health care professional plan delivery, management and care of an affected child • Providing risk information to couples to assist in making decisions regarding their reproductive future: PGD, egg/sperm donors, adoption, natural pregnancy with diagnosis, no children • Important points to question/inform patient – Can condition be adequately screened for/diagnosed – Will this information help them in any of the above ways such that it outweighs the risk of the procedure? – No test can guarantee a “healthy baby” Neonatal/Pediatric Genetics Indications for Genetic Referral in Neonatal/Pediatric Setting • • • • • • • • • • Developmental delay or mental retardation Dysmorphic features Under or overgrowth Failure to thrive Seizure disorder of unknown cause Hypotonia Abnormal or ambiguous newborn screening results Birth defect - either single or multiple Ambiguous genitalia Family history of genetic or chromosomal condition Physical Examination • Done by Medical Geneticist (MD) – Looking for dysmorphic features- subtle or distinct – Anthropomorphic measurements – Photos of other family members • Some findings are familial---does not mean it is not a syndrome! – Some findings are common---seen in 1-5% of the population (normal variant) Dysmorphology Exam • • • • • • • • • • • Head Shape/Hair pattern Ocular measurements Nose Ears Philtrum/Mouth/Palate Maxillary region Mandible Chest/Back Limbs/Hands/Feet GU Skin Common findings: seen in isolation 1-5% of population Not so common anymore… • 6-8 Café-au-lait macules, learning disability= Neurofibromatosis • VSD, failure to thrive, distinct nose= VCFS Importance • Identifies etiology • Provides prognosis and appropriate medical management recommendations • Provides accurate risk assessment for recurrence – Isolated cleft palate or cleft lip • Recurrence risk based on empiric data (3-5%) – If syndromic, recurrence risk may be up to 50%. • 22q11.2 deletion (DiGeorge syndrome), Van der Woude, Stickler syndrome Other tools…. • • • • Karyotype FISH for specific suspected syndrome Gene specific testing for suspected syndrome Chromosomal microarray – Is now considered by many societies as a first-tier clinical diagnostic test for individuals with unexplained developmental delay/intellectual disability (DD/ID), autism spectrum disorders (ASD), or multiple congenital anomalies (MCA) Newborn Screening – More Than “The PKU Test”! • • • • CYSTIC FIBROSIS ENDOCRINE CONDITIONS: Congenital adrenal hyperplasia (CAH)*± • Congenital hypothyroidism* HEMOGLOBIN CONDITIONS:Sickle cell disease and other hemoglobinopathies* METABOLIC CONDITIONS: – AMINO ACID CONDITIONS : Homocystinuria* • Hyperphenylalanemia, including • phenylketonuria (Pk ) Tyrosinemia* – FATT y ACID OxIDATION CONDITIONS : Carnitine uptake defect • Carnitine palmitoyl transferase I deficiency (CPT I)* • Carnitine palmitoyl transferase II deficiency (CPT II) • Multiple acyl-CoA dehydrogenase deficiency • (MADD) Short chain acyl-CoA dehydrogenase deficiency • (SCAD) Medium chain acyl-CoA dehydrogenase deficiency • (MCAD)± Long chain 3 hydroxyacyl-CoA dehydrogenase • deficiency (LCHAD)*± Very long chain acyl-CoA dehydrogenase • deficiency (VLCAD)*± – ORgANIC ACID CONDITIONS : Beta-ketothiolase deficiency • (BkD)± Glutaric acidemia, Type I (GA I)* • Isobutyryl CoA dehydrogenase deficiency • (IBD)± Isovaleric acidemia • (IVA)* ± Malonic aciduria • Maple syrup urine disease • (MSuD)± Methylmalonic acidemias (MMA/8 types)± • Propionic acidemia • (PA)*± 3-Hydroxy3-methylglutaryl CoA lyase • deficiency (HMG)* 2-Methyl3-hydroxybutyryl CoA dehydrogenase • deficiency (MBHD)* 2-Methylbutyryl CoA dehydrogenase • deficiency (2MBC)* 3-Methylcrotonyl CoA carboxylase deficiency (3MCC) • 3-Methylglutaconyl CoA hydratase deficiency (3MGH) • Multiple carboxylase deficiency – UREA CyCLE CONDITIONS : Arginase deficiency • Argininosuccinate lyase deficiency (ASA)± • Citrullinemia± – OTHER CONDITIONS : Biotinidase deficiency • Galactosemia± Newborn Hearing Screening 1/1000 young children have a major hearing loss 50% of congenital hearing loss is genetic • Early diagnosis is key to proper management Pregnancy & Neonatal Loss Chromosome Abnormalities in Pregnancy Loss • Approximately 25% of all clinically recognized pregnancies result in a loss • <20 weeks = miscarriage – Up to 50% are due to chromosome aneuploidy • Most are due to nondisjunction with little increased risk of recurrence • However, karyotyping can be indicated in repeat pregnancy loss since 2-5% of couples have a chromosomal abnormality causing the increased RR • >20 weeks = stillbirth – 5% are due to chromosome abnormalities – However, some of these do increase the RR and when no other cause is known it is recommended to consider karyotype and/or microarray Importance of a Genetic Workup • Can allow for a diagnosis which will answer some of the most important questions a parent will have – Why? – Will this happen again? – Was it my fault? • Therefore workups and often autopsies are essential Grief and Bereavement • Pregnancy loss is the same to the majority of parents, if not worse, than any other type of death • It is extremely important to encourage, respect, and promote proper grieving of a loss no matter how early – It’s often a loss of dreams/hopes/expectations – Avoid comments that take away from the current situation: you can have another one, at least it was early, etc • Important to: – See, hold, spend time with the baby/body – Take photos, they can always be kept in patient chart if not ready to take them home – Name the baby, memorialize the baby in some meaningful way to the family – Encourage the family to recognize their spiritual or religious beliefs – Discuss cremation/burial options • Offering gentle and beautiful photography services in a compassionate and sensitive manner • Work done by professional photographers who volunteer their services and are trained in this specific area – Photographers will work with families in order to fit their needs and desires • Soft, gentle heirloom photographs of these beautiful babies are an important part of the healing process • They allow families to honor and cherish their babies, and share the spirits of their lives • www.nowilaymedowntosleep.org Perinatal Hospice “When the prenatal diagnosis of a lethal fetal anomaly has been established, some patients choose to continue their pregnancies. We propose a model of care that incorporates the strengths of prenatal diagnosis, perinatal grief management, and hospice care to address the needs of these families.” —Hoeldtke NJ, Calhoun BC. "Perinatal Hospice." Am J Obstet Gynecol. 2001 Sept;185(3)525-9 • Medical, emotional, and spiritual support through pregnancy, labor, birth, life and death • Variety of services to help parents define a birth vision they are comfortable with • Families may choose any of the services that fit their needs “Regardless of the length of a baby's life or duration of illness, it is their lifetime. Both the infant and family deserve skilled and compassionate attention to their plight; a safety net throughout the experience; a palliative care approach, which emphasizes living fully those days, hours, and even moments.” —Sumner LH. Taking palliative care into pregnancy and perinatal loss. National Perinatal Association Bulletin. 2004;5(2). A news clip on Now I Lay Me Down To Sleep. http://www.msnbc.msn.com/id/21134540/vp/23481435#23481435 Thank You Questions?