kwon ch 15 abnormal psychology

Psychological Disorders
http://www.youtube.com/watch?v=RK8zaVYrsPI
(2:08-)
HW of the week 3/24-3/28
Monday
Ch 15 p.612-620
Tuesday
Ch 15 p.620-626
Block day
Ch 15 p.627-633
Study for vocab quiz and free response
Friday
Ch 15 p.634-642 ½
Last day to take ch 14 test
Agenda, Monday 3/24
Project
Unit introduction
Perspectives on psych disorders
Abnormal Psychology
Research Project
Research and explain one psychological disorder* to class
(*see signup sheet and outline for a list)
Due: next Tuesday and block day
Maximum TWO people per topic
5-10 min presentation
Include info on: definition, symptoms, diagnosis, treatment, case study etc
You will have this block day and half of next Monday to work on/rehearse project
Sign up for your project by Block day morning.
Topics are first-come, first-serve.
Presentations order is as listed in signup sheet
Project outline & rubric
Read through them both
Question & Concerns?
“Most people have problems from time to time but are not mentally ill.”
Prevalence
Approximately 48% of adults experience symptoms at least once in their lives
Approximately 80% who experienced symptoms per year do NOT seek treatment
A Matter of Degree
Determining Abnormality
Three Criteria:
ATYPICAL/DEVIANT BEHAVIOR
unusual behavior that is also disturbing to the values or beliefs of others is likely to be considered deviant.
DISTRESSING
such as in depression or debilitating anxiety
DYSFUNCTIONAL/HARMFUL
Often it is a matter of degree.
Ex. Drinking alcohol until no longer able to function well at home or work
• Watch “strange addiction” (chalk)
Psychological Disorders
Psychological Disorder
in which a behavior is judged to be:
deviant-not enough in itself and varies with time and culture
distressful
dysfunctional
Perspectives on Psychological
Disorders
Individual: One’s own sense of personal wellbeing determines normality.
Society: Behavior is abnormal when it does not conform to the existing social order.
Mental-health professional: Personality and degree of personal discomfort and life functioning d e termine normality.
Psychological Disorders
.
1.
There are 450 million people suffering from psychological disorders (WHO, 2004).
2.
Depression and schizophrenia exist in all cultures of the world.
Classification of Behavior
Difficult to define
Causes and cures are rarely obvious or clear-cut
Must be ongoing
Use DSM-IV
Historical Perspective
Perceived Causes
movements of sun or moon
lunacy--full moon
evil spirits
Ancient Treatments
T rephination, exorcism, being caged like animals, being beaten, burned, castrated, mutilated, or transfused with animal’s blood.
Trephination (boring holes in the skull to remove evil forces)
Ignorance (thinking demon possession as cause of mental disorders) led to harsh and ineffective remedial treatments
Medical Perspective
Explains that madness is not due to demonic possession, but an ailment of the mind.
Dance in the madhouse.
Medical Model
Medical models gained momentum when physicians discovered that syphilis infection led to mental disorders
Criticism on Medical model
Neglects importance of social circumstance and psychological factors (e.g., anorexia in the West)
Biopsychosocial Perspective
Assumes that biological, socio-cultural, and psychological factors combine and interact to produce psychological disorders.
Classifying Psychological Disorders
The American Psychiatric Association (APA) rendered a Diagnostic and Statistical Manual of
Mental Disorders (DSM) to describe psychological disorders.
The most recent edition is DSM-5 (2013)
DSM-IV ( Diagnostic and Statistical
Manual of Mental Disorders ) 2000
Standard classification of mental disorders
Diagnostic Criteria- Essential and associated features that must be present for the patient to be given a diagnostic label
Disorder Categories
Youth: Infancy, Childhood, & Adolescence
Delirium, Dementia, and other Cognitive
Disorders
Substance-Related
Schizophrenia & other Psychotic Disorders
Mood
Anxiety
Dissociative
Sexual
Eating
Sleep
Impulse Control
Multiaxial Classification
Axis I
All except mental retardation and personality disorder
Axis II
Personality Disorder or Mental Retardation
Axis III
General Medical Condition (diabetes, hypertension or arthritis etc)
Axis IV
Psychosocial or Environmental factors
(school or housing issues)
Axis V
Global Assessment http://www.youtube.com/watch?v=Oif3xDj lV5I
Goals of DSM
1.
2.
Describe (approx 300) disorders.
Determine how prevalent the disorder is.
DSM is uses observable symptoms so different professionals will give similar diagnosis
(reliable).
Others criticize DSM for “putting any kind of behavior within the compass of psychiatry.”
*childhood bipolar disorder
Labeling Psychological Disorders
Critics of the DSM-IV argue that labels may stigmatize individuals.
David Rosenhan: Pseudo-
Patient Experiment
Investigated reliability of psychiatric diagnoses
8 healthy people were admitted to psychiatric hospitals when complained of hearing voices
http://www.youtube.com/watch?v=j6bmZ8cV
B4o http://www.youtube.com/watch?v=eO5r9ms8myI
Rosenhan: Results
Staff treated patients as if they were really ill
Staff noted “abnormal” symptoms
Kept patients for an average of 19 days
Discharged with diagnosis of “schizophrenia in remission”
Rosenhan: Nonexistent
Impostor Experiment
Told hospital staff to expect pseudo-patients
(“impostors”)
No pseudo-patients were actually sent, but staff identified 41 anyway
(these were, in fact, real patients)
Rosenhan study conclusion
"it is clear that we cannot distinguish the sane from the insane in psychiatric hospitals" illustrated the dangers of dehumanization and labeling in psychiatric institutions.
Rosenhan: Implications
Psychiatrists disputed the results
Prompted changes in psychiatric diagnosis
The DSM-IV
Labeling Psychological Disorders
Labels may be helpful for healthcare professionals when communicating with one another and establishing therapy.
Agenda Tuesday 3/25
Perspectives
Learning
Biological/evolutionary
Social-cognitive
Signup for project topic
The Learning Perspective
Learning theorists believe anxiety disorder to be a product of:
Fear conditioning
Stimulus generalization
Reinforcement
Observational learning
The Learning Perspective
Stimulus Generalization tendency for the conditioned stimulus to evoke similar responses after the response has been conditioned.
e.g., if a child has been conditioned to fear a stuffed white rabbit, the child will exhibit fear of similar objects
The Learning Perspective
Reinforcement reinforcement helps maintain phobias and compulsions
Avoid/escape the feared situation => reduces anxiety => more of same behavior
The Learning Perspective
Young monkeys develop fear when they watch other monkeys who are afraid of snakes.
Parents transmit their fears to their children.
http://psychcentral.com/news/2007/03/16/howfear-is-learned/691.html
The Biological Perspective
Natural Selection (evolution) has led our ancestors to learn to fear snakes spiders, and other animals.
People didn’t develop lasting fear of overhead planes after WWII
Calbin Pott says depression served as adaptive function by slowing people down and prevent engaging in life-threatening behaviors
The Biological Perspective
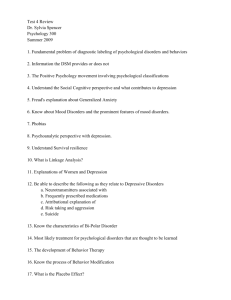
General anxiety, panic attacks, obsessions are biologically measurable
(= overarousal of brain areas involved in impulse control and habits)
Anterior Cingulate Cortex of an OCD patient.
Biological Perspective
Genetic Influences: Mood disorders run in families. The rate of depression is higher in identical (50%) than fraternal twins (20%).
Studies link possible genes and dispositions for depression.
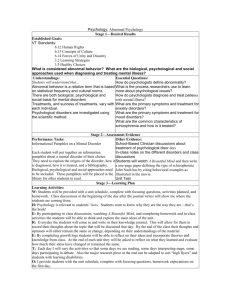
Neurotransmitters & Depression
A reduction of norepinephrine and serotonin has been found in depression.
Pre-synaptic
Neuron
Serotonin
Norepinephrine
Drugs that alleviate mania reduce norepinephrine.
Post-synaptic
Neuron
Social-Cognitive Perspective
• Emotional disturbance comes from selfblame (learned helplessness) and overgeneralized explanations (pessimism).
“I didn’t get the job because I’m stupid and inept” vs.
“I didn’t get the job because the interview didn’t go well”
Example
Explanatory style plays a major role in becoming depressed.
Cognitive Bases for Depression
A.T. Beck : depressed people hold pessimistic views of
themselves
the world the future
Depressed people distort in negative ways
exaggerate bad experiences minimize good experiences
Selection time!
Definition of some disorders
Depression Cycle
Hopelessness changes the way the individual thinks and acts, fueling personal rejection.
Seasonal affective disorder
a type of depression that occurs at the same time every year. If you're like most people with seasonal affective disorder, your symptoms start in the fall and may continue into the winter months, sapping your energy and making you feel moody.
Psychosomatic vs.
Somatoform
psychosomatic: patient's mental issues causes real physical illness. e.g., high blood pressure, limp
somatoform: group of mental disorders in which people have subjective feelings of illness that are seemingly untestable by medical means
Conversion Disorder
Somatoform disorders in which a dramatic specific disability has no physical cause but instead seems related to psychological problems .
Hypochondriasis
A somatoform disorder in which a person interprets insignificant symptoms as signs of serious illness in the absence of any organic evidence of such illness.
Kleptomania
irresistible urge to steal items that you generally don't really need and that usually have little value.
Munchausen (MOON-chow-zun) syndrome
someone with a deep need for attention pretends to be sick or gets sick or injured on purpose. People with
Munchausen syndrome may make up symptoms, push for risky operations, or try to rig laboratory test results to try to win sympathy and concern.
Histrionic personality disorder
characterized by a long-standing pattern of attention seeking behavior and extreme emotionality. Someone with histrionic personality disorder wants to be the center of attention in any group of people, and feel uncomfortable when they are not.
Project
Decide, sign up.
Agenda, Block day 3/26-27
• Computer lab research day
• Project due next block day
• 2, 4 th period: room 526
• 1 st period: room 209
• Vocab quiz, writing prompt on Friday
Homework of week 3/31-4/4
• Monday
• Tuesday
• Wednesday
• Thursday
• Friday