Our Children Can't Wait — Improving Services for

Educator Roles in Promoting Mental
Health and School Success for
PreK-12 Students
Carl E. Paternite, Ph.D.
Center for School-Based Mental Health Programs
Department of Psychology
Miami University (Ohio) http://www.units.muohio.edu/csbmhp
Presented at Mental Health Services and Schools Creating a Shared Vision
Ellicottville, NY
August 19 th , 2003
Educator Roles in Promoting
Mental Health and School
Success for PreK-12 Students
Instructional Objectives For Presentation:
Increase participant awareness of the importance of educators in school-based mental health programming.
Increase participant knowledge of effective approaches to enhance educator – mental health professional collaboration.
Increase knowledge of ways to infuse "mental health education" into the school milieu.
Educator Roles in Promoting
Mental Health and School
Success for PreK-12 Students
Themes Addressed in Presentation:
Program development.
Interdisciplinary collaboration and partnership.
Prevention.
Research, training and education.
Mental Health Needs of Youth and
Available Services
About 20% of children/adolescents (15 million), ages 9-17, have diagnosable mental health disorders (and many more are at risk or could benefit from help).
Less than one-third of youth with diagnosable disorders receive any service, and, of those who do, less than half receive adequate treatment (even fewer at risk receive help).
For the small percentage of youth who do receive service, most actually receive it within a school setting.
These realities raise questions about the mental health field’s over-reliance on clinic-based treatment, and have reinforced the importance of alternative models for mental health service
— especially expanded school-based programs.
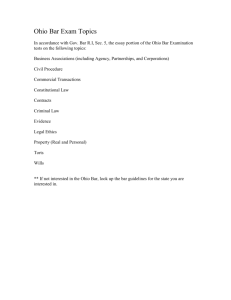
Leading Causes of Death in 15-19
Year Olds in the United States in 2000
— U N I T E D S T A T E S, 2000 —
CAUSE
Accidents
Homicide
Suicide
Cancer/Leukemia
Heart Disease
Congenital Anomalies
Lung Disease
Stroke
Diabetes
Blood Poisoning
HIV
# OF DEATHS
6573
1861
1574
759
372
213
151
60
40
36
36
1631
From Weist & Adelsheim, 2003
Report of President’s New Freedom
Commission on Mental Health
http://www.mentalhealthcommission.gov
“…the mental health delivery system is fragmented and in disarray…leading to unnecessary and costly disability, homelessness, school failure and incarceration.”
Unmet needs and barriers to care include (among others):
• Fragmentation and gaps in care for children.
• Lack of national priority for mental health and suicide prevention.
July, 2003
Report of President’s New Freedom
Commission on Mental Health: Six
Goals for a Transformed System
• Americans understand that mental health is essential to overall health.
• Mental health care is consumer and family driven.
• Disparities in mental health services are eliminated.
• Early mental health screening, assessment, and referral to services are common practice.
• Excellent mental health care is delivered and research is accelerated.
• Technology is used to access mental health care and information.
July, 2003
Four Recommendations Supporting Goal
4: Early Mental Health Screening,
Assessment, and Referral to Services are
Common Practice
1. Promote the mental health of young children.
2. Improve and expand school mental health programs .
3. Screen for co-occurring mental and substance use disorders and link with integrated treatment strategies.
4. Screen for mental disorders in primary health care, across the lifespan, and connect to treatment and supports.
July, 2003
Expanded School-Based
Mental Health Programs
National movement to place effective mental health programs in schools, serving youth in general and special ed.
To promote the academic, behavioral, social, emotional, and contextual/systems well-being of youth, and to reduce
“mental health” barriers to school success.
Programs incorporate primary prevention and mental health promotion, secondary prevention, and intensive intervention,joining staff and resources from education and other community systems.
Intent is to contribute to building capacity for a comprehensive, multifaceted, and integrated system of support and care.
University of Maryland
Center for School Mental Health
Assistance
Mark Weist
(http://csmha.umaryland.edu)
ESBMH
UCLA
Center for Mental Health Assistance
Howard Adelman & Linda Taylor
(http://smhp.psych.ucla.edu)
“Barriers to Learning”
(see handout)
Interconnected Systems for Meeting the
Needs of All Students
CONTINUUM OF SCHOOL AND COMMUNITY PROGRAMS AND SERVICES
(From Adelman & Taylor, http://smhp.psych.ucla.edu)
Continuum of Effective Behavior
Support
Students with
Chronic/Intense
Problem Behavior
(1 - 7%)
Students At-Risk for Problem
Behavior
(5-15%)
Tertiary Prevention
Secondary Prevention
Specialized Individual
Interventions
(Individual Student
System)
Specialized Group
Interventions
(At-Risk System)
Students without
Serious
Problem
Behaviors
(80 -90%)
Primary Prevention
Universal Interventions
(School-Wide System
Classroom System)
All Students in School
Potential of Schools as Key Points of
Engagement
Opportunities to engage youth where they are.
Unique opportunities for intensive, multifaceted approaches and are essential contexts for prevention and research activity.
Schools: The Most
Universal Natural Setting
• Over 52 million youth attend 114,000 schools
• Over 6 million adults work in schools
• Combining students and staff, one-fifth of the U.S. population can be found in schools
From Weist, 2003
Center for School-Based Mental Health
Programs (at Miami University)
Overarching Goals
Build collaborative university-school district relationships to address the mental health needs of children and adolescents through multifaceted programming.
Promote mental health and school success for youth through:
Primary prevention and mental health education
Early direct intervention for identified at-risk children and adolescents, and treatment for those with severe/ chronic mental health problems
Action research, training, and consultation
Center for School-Based Mental Health
Programs (at Miami University)
Ohio Mental Health Network for School Success
• Six affiliate organizations working together in regional and state-wide activities (including “ S hared Agenda” initiative)
Butler County School-Based Mental Health Program
• School-based mental health promotion, prevention, intervention, and applied research activities.
Addressing Barriers to Learning Program
• Annual conferences to initiate and sustain local, school-based projects that reduce mental health barriers to learning and enhance the development of healthy school communities.
Center for School-Based Mental Health
Programs (at Miami University)
Behavioral Health Advisor
• Mental health newsletter for elementary and secondary school educators, focusing on issues related to child mental health and school success.
Evaluation of Alternative Education/ Discipline
Programs
• Ongoing formative evaluation of 11 alternative programs in
Butler County,OH.
Mental Health for School Success
• Special project with Ohio Department of Education to promote mental health — education integration.
Center for School-Based Mental Health
Programs (at Miami University)
Funding History (current in bold )
Butler County Mental Health Board
The Health Foundation of Greater Cincinnati
Ohio Department of Mental Health
The Center for Learning Excellence
Butler County Family and Children First
Council
Talawanda and New Miami School Districts
Ohio Department of Education
Miami University cost sharing
School-Based Mental Health Partnerships
Many individuals have been instrumental to our school-based mental health partnerships since 1998. To name just a few:
University-Based (3 universities, 5 academic divisions, 6 departments)
Faculty/Staff: Carl E. Paternite, Karen Schilling, Julie Rubin, Denise Fox-Barber, Amy Wilms, Betty Yung, David Andrews, Al Neff, Diana Leigh, Alex
Thomas, Randy Flora, Doris Bergen, Valerie A. Ubbes, Raymond Witte, Joan FopmaLoy …
Psychology interns and graduate assistants : Lynne Knobloch, Becky Hutchison, Sally Phillips, Leslie Baer, Linda Gal, Derek Oliver, Mike Imhoff,
Julie Cathey, Liz Morey, Chris Dyszelski, Chris Mauro, Nancy Pike, Jessica Donn, Sandra Kirchner, LaTasha Mack, Ann-Marie Bixler, Jari Santana-
Wynn, Jeanene Robinson, Gloria Oliver, Francesca Dalumpines, Jamie Williamson, Jill Thomas, Jennifer Malinosky, Jason Kibby, Julia Pemberton, Ann
Marie Lundberg, Marc McLaughlin, Robin GraffReed, Melissa Maras, Chris Reiger, Julie Swanson …
Community-Based
John Staup, Kay Rietz, Saundra Jenkins, Barbara Perez, Susan Smith, Valerie Robinson, Jolynn Hurwitz, Kate Keller, Terri Johnston, Charlie Johnston,
Kathy Oberlin, Ellen Anderson, Noelle Duval, Linda Maxwell, Greg Foster, Teresa Jullian-Goebel, Suzanne Robinson, Terre Garner, Bryan Brown, Greg
Rausch, Carolyn Jones, David Turner …
School-Based
Teacher consultants : Sherie Davis, Marilyn Elzey, Tom Orlow, Teresa Abrams, Sarah Buck, Jim Carter, Julie Churchman, Amy Gibson, Joy Boyle,
Chris Carroll, Mary Hessling, Joan Parks, Joanne Williamson, Jaimie Pribble, Pam Termeer, Pat Stephens, Patricia Scholl, Martha Slamer, David Wood,
Susan Meyer, Monna Even, Ginny Paternite, Connie Short, Terri Hoffmann, Karen Shearer …
Guidance counselors, school psychologists, school nurses, and administrators : Marianne Marconi, Sandy Greenberg, Tom O’Reilly, Roberta
Perlin, Betsy Esber, MaryBeth Bergeron, Greg Rausch, Ann Schmitt, Alice Bonar, Stephanie Johnson, Marcia Schlichter, Susan Cobb, Phil Cagwin, Bob
Bierly, Martha Angello, Bill Miller, Bob Phelps, Dan Milz, Dave Isaacs, Mark Mortine, Rhonda Bohannon, Clint Moore, Cathy Keener, Mary Jane Roberts,
Jean Eagle, Alice Eby, Kathy Jonas, David Greenburg, Candice McIntosh, Sharon Lytle, Terri Fitton, Steve Swankhaus, Melissa Kessler, Mary Jacobs ..
Action-Project Teams : Fourteen 2-4 person teams from ten schools in five school districts, each with a university faculty/graduate student liaison.
The Ohio Mental Health Network for
School Success
Mission
To help Ohio’s school districts, community-based agencies, and families work together to achieve improved educational and developmental outcomes for all children — especially those at emotional or behavioral risk and those with mental health problems, including pupils participating in alternative education programs.
The Ohio Mental Health Network for
School Success
Action Agenda
Create awareness about the gap between children’s mental health needs and “treatment” resources, and encourage improved and expanded services (including new anti-stigma campaign).
Encourage mental health agencies and school districts to adopt mission statements that address the importance of partnerships.
Conduct surveys of mental health agencies and school districts to better define the mental health needs of children and to gather information about promising practices.
The Ohio Mental Health Network for
School Success
Action Agenda (continued)
Provide technical assistance to mental health agencies and school districts, to support adoption of evidence-based and promising practices, including improvement and expansion of school-based mental health services.
Develop a guide for education and mental health professionals and families, for the development of productive partnerships.
Assist in identification of sources of financial support for school-based mental health initiatives.
Assist university-based professional preparation programs in psychology, social work, public health, and education, in developing inter-professional strategies and practices for addressing the mental health needs of school-age children.
Policy Maker Partnership (PMP) at the National
Association of State Directors of Special
Education (NASDSE) and the National
Association of State Mental Health Program
Directors (NASMHPD)
Concept Paper
Mental Health, Schools and Families Working Together for All Children and Youth:
Toward A Shared Agenda (2002)
Purpose of the Concept Paper
“Encourage state and local family and youth organizations, mental health organizations, education entities and schools across the nation to enter new relationships to achieve positive social, emotional and educational outcomes for every child.”
The concept paper is available online at:
www.nasdse.org/sharedagenda.pdf
www.ideapolicy.org/sharedagenda.pdf
www.nasmhpd.org
Policy Maker Partnership (PMP) at the National
Association of State Directors of Special
Education (NASDSE) and the National
Association of State Mental Health Program
Directors (NASMHPD)
Shared Agenda Seed Grant Awards to Six States:
Missouri,
Ohio
, Oregon,
South Carolina, Texas, and Vermont
Additional Funding for Ohio’s Shared
Agenda Initiative
Ohio Department of Mental Health
Ohio Department of Education
Ohio Department of Health and
Numerous Additional State-level and Regional
Organizations
Infrastructure for Ohio’s Shared
Agenda Initiative
The Shared Agenda seed grant is being implemented in Ohio within the collaborative infrastructure of the Mental
Health Network
Three Phases of Ohio’s Shared
Agenda Initiative
Phase 1
—Statewide forum for leaders of mental health, education, and family policymaking organizations and childserving systems (March 3, 2003)
Phase 2 —Six regional forums for policy implementers and consumer stakeholders (April-May, 2003)
Phase 3 —Legislative forum involving key leadership of relevant house and senate committees (October, 2003)
Phase 1 and Phase 2
Shared Agenda Forums
Logo
Here
Columbus, OH — Statewide Forum, March 3, 2002
Athens, OH—Southeast
April 15, 2003
Columbus, OH—Central
April 29, 2003
Wooster, OH—North Central
April 28, 2003
Bowling Green, OH—Northwest
April 29, 2003
Cleveland, OH—Northeast
May 5, 2003
Hamilton, OH—Southwest
May 5, 2003
Strategies and Features of
Various Shared Agenda Forums
Keynote presentations by national and state experts:
•
•
•
•
•
•
• Mark Weist, Center for School MH Assistance, U. of Maryland
Steve Adelsheim, New Mexico School MH Initiative
Howard Adelman & Linda Taylor, UCLA School MH Project
Kimberly Hoagwood, Columbia University
Howie Knoff, Project Achieve
Joseph Johnson, Ohio Department of Education
Eric Fingerhut, Ohio State Senator
Strategies and Features of
Various Shared Agenda Forums
Promising work in Ohio showcased
Youth and parent testimony
Cross-stakeholder panel discussions
Facilitated discussion structured to create a collective vision, build a sense of mutual responsibility for reaching the vision, instill hope that systemic change is possible, and problem-solve regarding implementation issues
Appreciative Inquiry model for promotion of systems-level change and transformation informed the process
Outcomes and Recommendations from Phases 1 and 2 of Ohio’s
Shared Agenda Initiative
Approximately 725 participants
Report being compiled that will inform the Fall, 2003 Shared Agenda Legislative
Forum
Through Legislative Forum raise public awareness and build advocacy for policy and fiscal support for better alignment for education and mental health in the next biennial budget process
Website created to track and publicize Ohio’s Shared Agenda initiative
( http://www.units.muohio.edu/csbmhp/sharedagenda.html)
Ten Emerging Recommendations from Phases 1 and 2 of Ohio’s
Shared Agenda Initiative
Logo
Here
1.
Promote EFFECTIVE mental health and educational practices in schools
2.
Increase family and community involvement in school mental health and educational programs
3.
Actively solicit and appreciate student input in program planning and operation
4.
Reduce stigma for children who need mental health services
Ten Emerging Recommendations from Phases 1 and 2 of Ohio’s
Shared Agenda Initiative (cont’d)
Logo
Here
5.
Maintain focus on all children, not just students in special education
6.
Promote a better understanding of children’s mental health needs in schools
7.
Expand cross-discipline training (preservice and inservice) for mental health/family-serving providers, educators and parents
Ten Emerging Recommendations from Phases 1 and 2 of Ohio’s
Shared Agenda Initiative (cont’d)
Logo
Here
8.
Work more effectively to reduce “turf issues” that interfere with children’s mental health service delivery and with mental health-education collaboration
9.
Coordinate more effectively between state-level and regional/local efforts in the area of school mental health and in promotion of mental health and school success
10. Develop organizational structures (e.g., 501C3) that will promote strong coalitions and facilitate funding
Creating and Maintaining
Ongoing, Empowering
Dialogue with Educators
Multi-level, formal and informal dialogue with policy makers, formulators, enforcers, and implementers.
Programs for school board members and administrators.
Newsletter for teachers.
Website resources.
Extensive “contact time” with educators in their school buildings.
“Joining” the school community.
Key opinion leaders.
Assessing and Responding To
Educator-Identified Needs and
Concerns
Careful, detailed, local needs assessments from the perspective of educators, and a commitment to be responsive to identified needs.
Results used in advocacy efforts and as guideposts for ongoing work.
Perceived Problems
And
Teamwork Exercises
Teacher Consultants
Teacher consultants develop and implement special projects related to school-based mental health enhancement.
Teacher consultants serve as liaisons to the schools in efforts to promote school-based mental health programming.
Teacher consultants serve as informal advisers/mentors to school staff on matters related to social-emotional adjustment and learning needs of children and school/climate issues.
Incentives For Teacher Consultants
Leadership opportunity
Training opportunity
Academic credit
Stipends (“supplemental contracts”)
Empowerment
Demystification
Addressing Barriers to Learning: Annual
Conference and Action Projects
Program
Goal
Conduct annual conferences, to help initiate planned local public school-based projects that reduce mental health-related barriers to learning and enhance the development of healthy school communities.
Objectives of Addressing
Barriers to Learning Program
Demonstrate, produce and assess school-based mental health practices (classroom-based, classroom-linked) that address barriers to desired academic outcomes and personal and social skill development.
Put into continuing practice that which participants learn in conference activities and projects.
Increase the effectiveness of school district collaboration and system support for school-based mental health practices.
Disseminate findings.
Resources for Addressing
Barriers to Learning Program
Researchers and practitioners whose work on the conference theme evidences quality and the potential for successful application locally.
Web-site support.
Resource packets.
Small grants to support action projects.
Ongoing consultation with action teams with graduate students/faculty.
Conference Themes for
Addressing Barriers to
Learning Program
2000 — Nonviolent Schools: Building Programs That Work
Consultants: Betty Yung and Jeremy Shapiro
2001 — School, Family, and Community Partnerships
Consultants: Marc Atkins and Scott Rankin
2002 — School, Family, and Community Partnerships
Consultants: Program faculty
Addressing Barriers to Learning:
Current Elementary School
Action Projects
Schoolwide project focused on increasing students’ positive social skills, using monthly themes and activities (open house nights, assemblies, community speakers). Parent involvement in planning and implementation is emphasized.
Schoolwide project focused on “trait of the month” themes (e.g., responsibility, caring) and activities (community service projects, fund raising for needy families, school-based counseling groups, after school activities, peer mediation program).
School-wide attendance enhancement program, through improved monitoring, enhanced parental involvement with an after school/evening tutoring program linked to family dinner/activity events, and an attendance reward program.
Schoolwide outreach program to families (“The Road Show”) taking school informational meetings into neighborhoods and communities, to overcome obstacle of the geographically large catchment area and to increase family sense of engagement with the school.
School-wide project focused on positive social skills, with emphasis on recess programming.
Addressing Barriers to
Learning: Current Elementary
School Action Projects (cont’d)
A violence reduction program, focused on development of resource materials and use of psychoeducational training in coping skills and strategies for at risk students.
School-wide family engagement project emphasizing literacy, through school-based reading night dinner programs with storytellers and opportunities for families to read together.
School-wide parent involvement and support program focused on attention to needs of families, efforts to increase positive attitudes toward learning, and enhancement of social skills of students, using community picnics and “Parents on Board” parenting classes.
School-wide program focused on understanding and appreciating difference, tolerance, and conflict resolution skills, using curricula from the Center for Peace Education.
Addressing Barriers to
Learning: Current High School
Action Projects
Mentoring program focused on academic and personal success of students, including a strong community service component.
Alternative high school service learning program incorporating intensive involvement with a senior citizens center and tutoring in an elementary school.
Addressing Barriers to
Learning: Training in the
Project Evaluation Process
1. Determine goals and objectives.
2. Determine data needed to measure desired outcomes.
3. Select measurement methods.
4. Outline data collection plan.
5. Collect data.
6. Compile, analyze, interpret, and report results.
7. Refine project based on findings.
Note: Dr. Doris Bergen (Miami University Center for Human Development, Learning, and
Teaching) has provided ongoing technical assistance on the evaluation process.
Addressing Barriers to
Learning:Levels of Evaluation
Evaluation expected on two or more of the four levels:
Level 1 -- Records on planned activities.
Level 2 -- Self-report data from participant groups on knowledge, attitudes, behaviors.
Level 3 -- Outcome data on student effects (attendance, office referrals, grades…).
Level 4 -- Systematic observational data on behavior change related to objectives of project.
Note: Dr. Doris Bergen (Miami University Center for Human Development, Learning, and
Teaching) has provided ongoing technical assistance on the evaluation process.
Addressing Barriers to
Learning: Linking Project
Objectives to Evaluation
“The Road Show”
Objectives:
Increase family involvement with school
Increase student attendance
Decrease discipline referrals
Evaluation Plan:
Number of positive/negative calls to school
“Road show” attendance rates and parent survey
Attendance at parent conferences
Student attendance rates
Student discipline referrals
Educators as Key Members of the Mental Health Team
Schools should not be held responsible for meeting every need of every student.
However, schools must meet the challenge when the need directly affects learning and school success.
(Carnegie Council Task Force on Education of Young
Adolescents, 1989)
There is clear and compelling evidence that there are strong positive associations between mental health and school success.
Educators as Key
Members of the Mental
Health Team
“Children whose emotional, behavioral, or social difficulties are not addressed have a diminished capacity to learn and benefit from the school environment. In addition, children who develop disruptive behavior patterns can have a negative influence on the social and academic environment for other children.” (Rones & Hoagwood, 2000, p.236)
Contemporary school reform —and the associated highstakes testing (including federal legislation signed in 2002) — has not incorporated the Carnegie Council imperative. That is, recent reform has not adequately incorporated a focus on addressing barriers to development, learning, and teaching.
Educators as Key
Members of the Mental
Health Team
An Exercise:
How much time do you spend addressing the emotional,behavioral, and/or social difficulties of your students (minutes per hour)?
Context Examples
Senior high school with
880 students reported over 5,100 office discipline referrals in one academic year.
What does this mean?
• 5100 referrals @ 10 minutes each =
– 51,000 minutes or
– 850 hours or
– 141 6 hour days!
Context Examples
Middle school principal reports he must teach classes when teachers are absent, because substitute teachers refuse to work in a school that is unsafe and lacks discipline.
Context Examples
Middle school counselor spends nearly 15% of day “counseling” staff who feel helpless & defenseless in their classrooms because of lack of discipline & support.
Context Examples
Elementary school principal found that over 45% of their behavioral incident reports were coming from the playground.
Context Examples
Three rival gangs are competing for “four corners.” Teachers actively avoid the area.
Because of daily conflicts, vice principal has moved her desk to four corners to regain control.
Context Examples
Bus transportation company is threatening to w/draw their contract if students don’t improve their behavior. Recently, security guards were hired to ride buses.
Context Examples
Elementary school principal reports that over 100% of her office discipline referrals came from 8.7% of her total school enrollment, & 2.9% had 3 or more.
Who’s problem is it?
• In one school year, Jason received 87 office discipline referrals.
• In one school year, a teacher processed
273 behavior incident reports.
Something to Think About
• “Any student who is giving it bad to an educator is getting it at least as bad or worse from some important source in his life.”
(Mendler, 1997)
Problem Behaviors
Insubordination, noncompliance, defiance, late to class, nonattendance, truancy, fighting, aggression, inappropriate language, social withdrawal, excessive crying, stealing, vandalism, property destruction, tobacco, drugs, alcohol, unresponsive, not following directions, inappropriate use of school materials, weapons, harassment, unprepared to learn, parking lot violation, irresponsible, trespassing, disrespectful, disrupting teaching, uncooperative, violent behavior, disruptive, verbal abuse, physical abuse, dress code, other, etc., etc., etc.
• Exist in every school
• Vary in intensity
• Are associated w/ variety of contributing variables
• Are concern in every community
Prioritizing Promotion of Healthy
Development and Problem Prevention
Schoolbased models should capitalize on schools’ unique opportunities to provide mental health-promoting activities.
For example, recommended strategies for drop-out and violence prevention, including those for which the central role of educators is evident, can be promoted actively within an expanded school-based mental health program.
Prioritizing Promotion of Healthy
Development and Problem Prevention
For drop-out prevention, these include:
Early intervention.
Mentoring and tutoring.
Service learning.
Conflict resolution and violence prevention curricula and training for students/staff.
Alternative schooling.
Some of What We Know About Youth Violence
From the Surgeon General (2001), U.S. Secret Service (2000),
CDC (2002), Mulvey & Cauffman (2001)
Violence is a serious public health problem.
Violence is most often expressive/interpersonal, rather than primarily instrumental or psychopathological.
About 30 to 40 percent of male and 15 to 30 percent of female youth report having committed a serious violent offense by age 17.
About 10 to15 percent of high school seniors report that they have committed an assault with injury in the past year
— a rate that has been rising since 1980.
By self-report, about 30 percent of high school seniors have committed a violent act in the past year — hit instructor or supervisor; serious fight at school or work; in group fight; assault with injury; used weapon (knife/gun/club) to get something from a person.
Violent acts are committed much more frequently by male than by female youth. (see
Miedzian, 1991)
Some of What We Know About Youth Violence
(continued)
43% of male and 24% of female high school students report that they had been in a physical fight during the past school year. (CDC, 2002)
No differences are evident by race for self-report of violent behavior.
At school, highest victimization rates are among male students.
Violent behavior seldom results from a single cause.
School continues to be one of the safest places for our nation’s children.
Serious acts of violence (e.g., shootings) at school are very rare.
Targeted violence at school is not a new phenomenon.
Most school shooters had a history of gun use and had access to them.
In over 2/3 of school shooting cases, having been bullied played a role in the attack.
“For every complex problem there is a simple solution that is wrong.”
H.L. Mencken
A QUESTION:
WHAT ARE THE CAUSES
OF VIOLENCE, OTHER
PROBLEM BEHAVIOR,
AND DISCIPLINE
PROBLEMS?
Causes of Violence, Other
Problem Behavior, and Discipline
Problems
• Out-of-School
– Society
– Media
– More children living in poverty
– Deterioration of family
– Difficult temperaments
– Less able to listen effectively and process verbal material, compared to children 20 – 30 years ago
Violent Behavior
(Resnick et al., 1997)
• Behaviors modeled by sports and television heroes desensitize students to violence and antisocial behaviors
• Strongest protective factors from antisocial behavior…
– Strong emotional attachments to parents and teachers
Aggressive and Rejected
Children
• Thinking errors
– Attribute hostile intentions to accidental or ambiguous behavior
– Misinterpret important social cues
– Tease others but respond incompetently when provoked
Educators
• Thinking errors
– If punishment is severe enough, children will cease negative behavior
– Punishment is in the best interest of the child
– Well controlled classrooms must be quiet classrooms
– Control is like a behavioral ointment:
• no control at home = slather it on in school
– Prescribed discipline programs provide security for staff
Model: Influences on Violent versus
Non-Violent Behavior
(From Shapiro, 1999, Applewood Centers, Inc., Cleveland, OH)
Some of What We Know About
Youth Violence Prevention
From the Surgeon General (2001), U.S. Secret Service (2000),
CDC (2002), Mulvey & Cauffman (2001)
Promoting healthy relationships and environments is more effective for reducing school violence than instituting punitive penalties.
The best predictor of adolescent well-being is a feeling of connection to school.
Students who feel close to others, fairly treated, and vested in school are less likely to engage in risky behaviors.
A critical component of any effective school violence program is a school environment in which ongoing activities and problems of students are discussed, rather than tallied. Such an environment promotes ongoing risk management, which depends on the support and involvement of those closest to the indicators of trouble — peers and teachers.
Violence Prevention:
What Doesn’t Work
From the Surgeon General (2001) and others
Scare tactics. (e.g., Scared Straight)
Deterrence programs — shock incarceration, boot camps.
Efforts focusing exclusively on providing education/information about drugs/violence and resistance. (DARE)
Efforts focusing solely on self-esteem enhancement.
Vocational counseling.
Residential treatment.
Traditional casework and clinic-based counseling.
Promoting Nonviolence: An
Example of a Heuristic
School-Based Framework
Deutsch (1993) — Educating for a peaceful world
Four Key Components Including:
Cooperative Learning.
Conflict Resolution Training.
Use of Constructive Controversy in Teaching Subject
Matters.
Mediation in the Schools.
Prioritizing Promotion of Healthy
Development and Violence Prevention:
Best and Promising Practices
Including:
Structured social skill development programs.
Mentoring. (see Big Brothers/Sisters; Garbarino, 1999)
Employment.
Programs that foster school engagement, participation, and bonding.
Promotion of developmental assets. (see Search Institute)
A variety of approaches that engage parents and families. (e.g., parent training, MST, functional FT)
Early childhood home visitation programs.
Multi-faceted programs that combine several of the above.
For good examples see “Blueprint Programs.”
Developmental Assets and Violence
(1997 data, www.search-institute.org)
Approximately 100,000 6 th -12 th graders.
Definition of violence —three or more acts of fighting, hitting, injuring a person, carrying a weapon, or threatening physical harm in the past 12 months.
61% of youth with fewer than 11 of 40 developmental assets were violent.
6% of youth with 31 or more of 40 developmental assets were violent.
Continuum of Effective Behavior
Support
Students with
Chronic/Intense
Problem Behavior
(1 - 7%)
Students At-Risk for Problem
Behavior
(5-15%)
Tertiary Prevention
Secondary Prevention
Specialized Individual
Interventions
(Individual Student
System)
Specialized Group
Interventions
(At-Risk System)
Students without
Serious
Problem
Behaviors
(80 -90%)
Primary Prevention
Universal Interventions
(School-Wide System
Classroom System)
All Students in School
Positive Behavior Support
(see www.pbis.org)
• PBS is a broad range of systemic & individualized strategies for achieving important social & learning outcomes while preventing problem behavior with all students.
Terminology
• Positive Behavior….
– Includes all skills that increase success in home, school and community settings.
• Supports….
– Methods to teach, strengthen, and expand positive behaviors.
– System change.
Discipline Defined
• “The steps or actions, teachers, administrators, parents, and students follow to enhance student academic and social behavior success.”
• “Effective discipline is described as teaching students selfcontrol.”
Reactive Vs. Proactive
• Traditional approaches. (including aversive interventions)
– Address problem behaviors reactively
– Crisis driven
• PBS emphasizes proactive interventions.
Goals
1.
Improved quality of life for all relevant stakeholders. (the individual, family members, teachers, friends, employers, etc.)
2.
Problem behaviors become irrelevant, inefficient, and ineffective and are replaced by efficient and effective alternatives.
PBS Interventions
• Context driven.
• Addressing the functionality of the behavior problem.
• Acceptable to the individual, family and community.
PBS is a Problem-Solving
Process
• Decisions are based upon functional behavioral assessment. (FBA)
• FBA directs intervention design.
– FBA establishes instructional targets for alternative skills
– FBA designates supports and context revisions required for maintenance of positive changes
Systems Change
****DEFINING FEATURE OF PBS****
• Efforts focused on fixing problem contexts, not problem behavior.
• Successful outcomes can not depend solely on identifying ONE key critical intervention to “fix” the problem.
Components of School-
Wide Systems
• Common philosophy.
• Positively stated rules. (3 or 4)
• Behavior expectations defined by context.
• Teaching behavior expectations in context.
• Reinforcement of expectations.
• Discouragement of violations.
• Monitor and evaluate effects.
Two Distinct Discipline Models
• Obedience Model
• Responsibility Model
From Johnston (2003)
Obedience
• MAIN GOAL:
– Student follows orders
• PRINCIPLE:
– Do what the teacher wants
• INTERVENTION: PUNISHMENT
– External locus of control
– Done to the student
• STUDENT LEARNS:
– Don’t get caught
– It’s not my responsibility
From Johnston (2003)
Responsibility
•MAIN GOAL:
To teach students to make good choices
•PRINCIPLE:
Learn from the outcomes of decisions
•INTERVENTION: CONSEQUENCES
Internal locus of control
Natural or logical
Done by the student
•STUDENT LEARNS:
I have more than one alternative
I have power to choose
I cause my own outcomes
From Johnston (2003)
Science of behavior has taught us that students….
• Are NOT born with “bad behaviors”
• Do NOT learn when presented contingent aversive consequences
• Do learn better ways of behaving by being taught directly & receiving positive feedback
From Johnston (2003)
Teacher Behaviors That
Contribute to Discipline
Problems
• Sitting at the desk most of the time, not moving or mingling with the students
• Using a low, unenthusiastic or uniteresting voice tone
• Becoming easily sidetracked by one student’s irrelevant question
From Johnston (2003)
Teacher Behaviors That
Contribute to Discipline
Problems
• Ignoring students’ interests and tying instruction solely to the textbook
• Repeating student’s answers too frequently
• Leaving concepts before they have been clarified and/or expecting independent work before understanding has been checked
• Not being prepared and leaving “down time” for students to fill
From Johnston (2003)
Teacher Behaviors That
Contribute to Discipline
Problems
• Poorly worded questions that cloud discussion or understanding
• Having questions/answers be directed solely between teacher and student
• Neglecting to tie content or learning to prior knowledge of students
• Using too much time to teach the lesson and not focusing on what is being learned
From Johnston (2003)
Teacher Behaviors That Contribute to
Reduction of Discipline Problems
• Remove conditions that trigger & maintain undesirable practices
• Increase conditions that trigger & maintain desirable practices
• Remove aversives that inhibit desirable practices
• Establish environments & routines that support continuum of PBS
From Johnston (2003)
Promoting Nonviolence
:
An
Example of a Promising Secondary
Violence Prevention Program
Positive Adolescent Choices Training (PACT)
Developed by
Betty R. Yung & W. Rodney Hammond
Components
I. Violence-Risk Education
II. Anger Management
III. Social Skills
Continuum of Effective Behavior
Support
Students with
Chronic/Intense
Problem Behavior
(1 - 7%)
Students At-Risk for Problem
Behavior
(5-15%)
Tertiary Prevention
Secondary Prevention
Specialized Individual
Interventions
(Individual Student
System)
Specialized Group
Interventions
(At-Risk System)
Students without
Serious
Problem
Behaviors
(80 -90%)
Primary Prevention
Universal Interventions
(School-Wide System
Classroom System)
All Students in School
PACT Components I and II
Violence Risk Education:
Increase awareness of circumstances, risk factors, and consequences of violence.
Anger Management:
Understand and normalize feelings of anger, recognize anger triggers, and manage anger constructively.
PACT Components III:
Social Skills
Givin’ It:
Expressing criticism, disappointment, anger, or displeasure calmly and ventilating strong emotions constructively.
Takin’ It:
Listening, understanding, and reacting appropriately to others’ criticism and anger.
Workin’ It Out:
Listening, identifying problems and potential solutions, proposing alternatives when disagreements persist, and learning to compromise.
Closing Observations
Clearly, intellectual, social, and emotional education go hand-in-hand, and all are linked to creating safe schools, building healthy character, and achieving academic success:
The proper aim of education is to promote significant learning.
Significant learning entails development. Development means successively asking broader and deeper questions of the relationship between oneself and the world. This is as true for first graders as it is for graduate students, for fledgling artists as graying accountants.
A good education ought to help people become more perceptive to and more discriminating about the world: seeing, feeling, and understanding more, yet sorting the pertinent from the peripheral with ever finer touch, increasingly able to integrate what they see and to make meaning of it in ways that enhance their ability to go on growing.
To imagine otherwise, to act as though learning were simply a matter of stacking facts on top of one another, makes as much sense as thinking one can learn a language by memorizing a dictionary. Ideas only come to life when they root in the mind of a learner. (Daloz, 1999, p. 243)
Closing Observations
The need for increased attention to mental health promotion on behalf of youth, is quite clear:
We have a burgeoning field of developmental psychopathology but have a more diffuse body of research on the pathways whereby children and adolescents become motivated, directed, socially competent, compassionate, and psychologically vigorous adults. Corresponding to that, we have numerous research-based programs for youth aimed at curbing drug use, violence, suicide, teen pregnancy, and other problem behaviors, but lack a rigorous applied psychology of how to promote youth development.
The place for such a field is apparent to anyone who has had contact with a cross section of American adolescents. (Larson,
2000, p. 170)
Closing Observations
Certainly, educators are key partners in efforts to intervene with children in need and to promote development.
In fact, through their day-to-day interactions with students, educators are the linchpins of school-based efforts to encourage healthy psychological development of youth.
This PowerPoint Presentation, with a reference list for cited work, will be posted on the CSBMHP website http://www.units.muohio.edu/csbmhp
Common Messages Across Initiatives
It is important to build on the common goals of expanded school-based mental health programs and existing community and school initiatives. For example, in Ohio:
• “Shared Agenda Initiative”
• “Partnerships for Success”
• “Alternative Education Challenge Grant Program”
All share a common core focus on barriers to development, learning, and teaching.
Identification of the common message across initiatives is extremely important for reducing the chances that what is being introduced by any one initiative will be marginalized by proponents of narrowly-focused school reform.
Strategies and Features of
Various Shared Agenda Forums
Keynote presentations by national and state experts:
•
•
•
•
•
•
• Mark Weist, Center for School MH Assistance, U. of Maryland
Steve Adelsheim, New Mexico School MH Initiative
Howard Adelman & Linda Taylor, UCLA School MH Project
Kimberly Hoagwood, Columbia University
Howie Knoff, Project Achieve
Joseph Johnson, Ohio Department of Education
Eric Fingerhut, Ohio State Senator
Strategies and Features of
Various Shared Agenda Forums
Promising work in Ohio showcased
Youth and parent testimony
Cross-stakeholder panel discussions
Facilitated discussion structured to create a collective vision, build a sense of mutual responsibility for reaching the vision, instill hope that systemic change is possible, and problem-solve regarding implementation issues
Appreciative Inquiry model for promotion of systems-level change and transformation informed the process
Proven, Successful Treatments
Exist for Most Disorders
Treatment success rates:
• 80% for major depression
• 65% for bipolar disorder
• 60% for schizophrenia
• 45% for heart disease
From Weist & Adelsheim, 2003
Characteristics of Children Living in
Poverty
(Ruby Payne, 1998 )
• Laughs when disciplined; or is disrespectful to the teacher
• Argues loudly with the teacher
• Responds angrily
• Uses inappropriate or vulgar comments
• Fights to survive or uses verbal abuse with other students
Characteristics of Children
Living in Poverty
(Ruby Payne, 1998)
• Hands are always on someone else
• Can’t follow directions
• Is extremely disorganized
• Talks incessantly
• Cheats or steal
Characteristics of Children
Living in Poverty
(Ruby Payne, 1998)
• If one out of every four children under the age of 18 in the USA was living in poverty in 1996, 25% or more of our students may exhibit these behaviors in the classroom.
Students can’t learn when fearful of...
• Physical assault
• Assault to self-esteem
• Damages to personal property
…and teachers can’t teach!
Carly and Aidan in their vehicles
QuickTime™ and a TIFF (Uncompressed) decompressor are needed to see this picture.
QuickTime™ and a TI FF (Uncompressed) decompressor are needed to see this pict ure.
Carly, Elmo and Aidan
QuickTime™ and a TIFF (Uncompressed) decompressor are needed to see this picture.