Clinical Assessment - LAUSD School Mental Health
advertisement

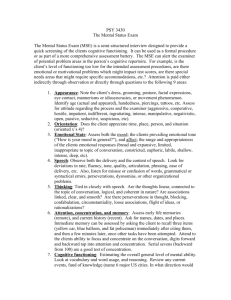
Clinical Assessment LAUSD School Mental Health October 29, 2014 Presenter: Eugene Alper, LCSW Assessment A complete and thorough assessment: Lays the foundation for an accurate diagnosis Demonstrates medical necessity and the need for services. Leads to appropriate selection of treatment plan objectives, services, and interventions Is ongoing throughout the course of treatment Must be completed within 30 days, but no later than the 2nd claimed service Important Assessment Components: Bio-Psycho-Social Assessment Interview(s) in which information is obtained from the client and the client’s parent/guardian (for minor clients). Outcome Measures Mental Status Substance Use Assessment Other Relevant Documents or Sources* * May require a signed release of information Risk Factors Other Relevant Documents or Sources IEPs Psych Reports Previous or Current Service Providers Teachers and Other School Staff Family DCFS Members Social Workers Other The Clinical Loop The Clinical Loop: Consists of the connection between the Assessment Symptoms and Functional Impairments Diagnosis Treatment Plan Selected Interventions and Services Progress Notes Clinical Loop, Cont’d. Includes the sequence of documentation that supports the demonstration of ongoing medical necessity Includes the process of continual reassessment and monitoring and documentation of progress Clinical Loop, Cont’d. Assessment Progress Notes Service Delivery Diagnosis Treatment Plan Mental Status The aim of the mental status examination (MSE) is to be an objective description, not interpretation, of the child’s appearance, symptoms, behavior and functioning as manifested at the time of the examination. A well-written MSE enables another clinician or the same clinician weeks, months or years later to have a clear picture of the patient’s mental state at the time of assessment. Mental Status The MSE is purely descriptive, includes no judgment of whether the appearance and behavior is normal or abnormal, clinically significant or non-significant. Although presented as a separate component that is distinct from the history-taking, in reality much of the MSE takes place implicitly as the clinician interacts and observes the child during the individual and family interviews. Cultural considerations: There are potential problems when the MSE is applied in a cross-cultural context, when the clinician and patient are from different cultural backgrounds. Culturally normative spiritual and religious beliefs need to be distinguished from delusions and hallucinations without understanding may seem similar though they have different roots. Cognitive assessment must also take the patient's language and educational background into account. Clinician's racial bias is another potential confounder. MSE with Children: There are particular challenges in carrying out an MSE with young children and others with limited language such as people with intellectual impairment. In this group, utilize tools such as play materials Puppets Art Materials or Diagrams with multiple choices of facial expressions depicting emotions The child’s stage of development should also be considered. Mental Status Components Component: Take Notice Of: May Be Used To Assess: Physical Appearance Quality of Self-care Abuse or Neglect Medical Concerns Drug and Alcohol Use or Abuse Mood (Depression, Mania) Psychosis Neurological disorders Side effects of medication Tourette's syndrome Psychotic symptoms Autism Mania Delirium. Depression Medical condition Medical conditions Specific language disorders Autism Psychosis Mania Anxiety Depression Age (actual and apparent) Age-appropriate clothes Grooming and cleanliness Differences in body structure, bruises, scars Height & Weight Physical features of alcohol or drug abuse Odor Tics, mannerisms Activity level Arousal level Coordination Unusual Motor Patterns Eye contact, quality, and movement Gait Repetitive purposeless movements Fluency Volume Rate Rhythm Articulation Language skill Stuttering Mutism Echolalia (repetition of another person’s words) Palilalia (repetition of one’s own words) Vocabulary Psychomotor Behavior Speech and Language Mental Status Components Component: Take Notice Of: May Be Used To Assess: Thought Content Overvalued ideas (a false belief that is held with conviction) Preoccupations Delusions Obsessions Psychosis Obsessive Compulsive Disorder Personality Disorders Depression Clinical risk Anxiety Phobias Quantity (i.e. poverty of thought) Tempo (i.e. flight of ideas) Retarded or Inhibited thoughts Coherency of thought Perseverations Thought Disorders Mania Depression Anxiety Psychosis Personality Disorders Organization of thought (i.e. thought blocking, fusion, loosening of associations, tangential thinking, derailment of thought, circumstantial) Developmentally appropriate vocabulary Fund of knowledge Appropriate drawings Alertness (awareness of & response to environment) Orientation (to person, place, & time) Attention & concentration Psychosis Anxiety Attention Deficit Intoxication Neuropsychological problems Side effects of psychiatric medications Chronic drug or alcohol use Brain damage including tumors Other brain disorders Memory (short & long term) Abstraction (the ability to categorize) Thought Process Overall cognitive functioning Mental Status Components Component: Take Notice Of: May Be Used To Assess: Mood Anxiety Depression Mania Ability to describe their mood state Affect Client's description of his/her mood Clinician’s observation of client mood: neutral, euthymic (reasonably positive mood), dysphoric (unhappiness), euphoric (elated mood), angry, anxious or apathetic (indifference or suppression of emotion). Emotion conveyed by the person's nonverbal behavior Appropriateness, intensity, range, reactivity and mobility Appropriateness to the current situation Congruency with their thought content Range and Reactivity of Affect Depression PTSD Psychosis Mania Personality Disorder Suicidal thoughts or behavior Self-harming behavior Thoughts or plans of harming others Risk-taking behavior Anxiety Depression Impulse control disorders Personality disorders Psychosis Mania Drug or alcohol abuse Eye contact Ability to cooperate and engage with assessment Behavior towards parents and siblings Cooperation, guardedness, hostility The quality of information obtained during the assessment. Examination of risk Attitude/Rapport Mental Status Components Component: Judgment Take Notice Of: May Be Used To Assess: Acknowledgement of problems Capacity to judge hypothetical situations Attitude towards receiving help Compliance with treatment Capacity to make sound, reasoned and responsible decisions Impulsiveness Planning ability Impaired judgment is not specific to any diagnosis but may be a prominent feature of disorders affecting the frontal lobe of the brain. If a person's judgment is impaired due to mental illness, there might be implications for the person's safety or the safety of others Recognition that one has a mental illness Compliance with treatment Ability to re-label unusual mental events (such as delusions and hallucinations) as pathological Adaptive capacity Assets Motivation for treatment Psychosis Dementia Client’s readiness for treatment Strengths to build upon in treatment Insight Strengths Suggested Questions for the MSE with Children What do you enjoy most? Why? What is your favorite movie/t.v. program? Tell me about it. What would you like for your birthday? If you had three wishes, what would you wish for? Why? What’s the nicest/worst thing that’s ever happened to you? What would you like to be when you grow up? Why do you think your mother/father/parents/grandma brought you to see me? Suggested Questions for the MSE with Children Do you have any friends? Who is your best friend? His/her name? What do you do together? How long have you been friends? Do you ever feel lonely? When? What do you do? What rules do you have in your house? What happens when you break a rule? Do you usually get blamed for things? What are your brothers and sisters like? Do you get along with them? Suggested Questions for the MSE with Children What things do you like best about school? What are the worst/hardest things? Are you the smartest, dumbest in your class or somewhere in-between? How do you get along with your teacher? Do you get into fights at school? Often? What makes you mad? What makes you sad? How is your mood most of the time (Happy, Sad, Mad, Scared)? Have you ever felt so bad you wished you could disappear? Die? Have you ever tried to hurt yourself? Role Play the MSE Get together with your elbow partner and take turns interviewing each other, and gathering information for the MSE, using the following “student” as the client. You have 10 minutes to do this exercise. I’ll have you switch at the midpoint. Have Fun! Maggie’s Story “True Story” from a LA County Agency 7 years old, female, African American Presents with Depressive Sxs (irritability, daily crying outbursts, suicidal ideation, lack of interest in play), Anxiety Sxs (separation fears, cannot sleep alone, worries about family members and future), and Disruptive Behavior (“attitude”, non-compliance with adult commands, aggressive behavior towards sibs) History of trauma and recent assault by male classmate who touched her in private parts Children’s Global Assessment Scale 100-91 Superior functioning in all areas (at home, at school and with peers); involved in a wide range of activities and has many interests (eg., has hobbies or participates in extracurricular activities or belongs to an organised group such as Scouts, etc); likeable, confident; ‘everyday’ worries never get out of hand; doing well in school; no symptoms. 90-81 Good functioning in all areas; secure in family, school, and with peers; there may be transient difficulties and ‘everyday’ worries that occasionally get out of hand (eg., mild anxiety associated with an important exam, occasional ‘blowups’ with siblings, parents or peers). 80-71 No more than slight impairments in functioning at home, at school, or with peers; some disturbance of behaviour or emotional distress may be present in response to life stresses (eg., parental separations, deaths, birth of a sib), but these are brief and interference with functioning is transient; such children are only minimally disturbing to others and are not considered deviant by those who know them. 70-61 Some difficulty in a single area but generally functioning well (eg., sporadic or isolated antisocial acts, such as occasionally playing hooky or petty theft; consistent minor difficulties with school work; mood changes of brief duration; fears and anxieties which do not lead to gross avoidance behaviour; selfdoubts); has some meaningful interpersonal relationships; most people who do not know the child well would not consider him/her deviant but those who do know him/her well might express concern. 60-51 Variable functioning with sporadic difficulties or symptoms in several but not all social areas; disturbance would be apparent to those who encounter the child in a dysfunctional setting or time but not to those who see the child in other settings. 50-41 Moderate degree of interference in functioning in most social areas or severe impairment of functioning in one area, such as might result from, for example, suicidal preoccupations and ruminations, school refusal and other forms of anxiety, obsessive rituals, major conversion symptoms, frequent anxiety attacks, poor to inappropriate social skills, frequent episodes of aggressive or other antisocial behaviour with some preservation of meaningful social relationships. 40-31 Major impairment of functioning in several areas and unable to function in one of these areas (ie., disturbed at home, at school, with peers, or in society at large, eg., persistent aggression without clear instigation; markedly withdrawn and isolated behaviour due to either mood or thought disturbance, suicidal attempts with clear lethal intent; such children are likely to require special schooling and/or hospitalisation or withdrawal from school (but this is not a sufficient criterion for inclusion in this category). 30-21 Unable to function in almost all areas eg., stays at home, in ward, or in bed all day without taking part in social activities or severe impairment in reality testing or serious impairment in communication (eg., sometimes incoherent or inappropriate). 20-11 Needs considerable supervision to prevent hurting others or self (eg., frequently violent, repeated suicide attempts) or to maintain personal hygiene or gross impairment in all forms of communication, eg., severe abnormalities in verbal and gestural communication, marked social aloofness, stupor, etc. 10-1 Needs constant supervision (24-hour care) due to severely aggressive or self-destructive behaviour or gross impairment in reality testing, communication, cognition, affect or personal hygiene.