Promoting Healthy Behavior - Population Reference Bureau
advertisement

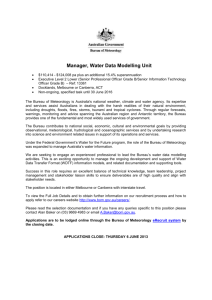
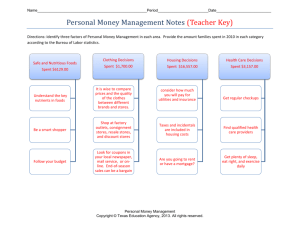
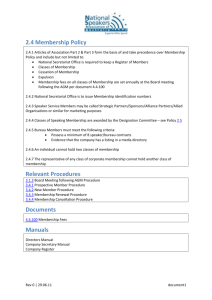
Promoting Healthy Behavior © 2005 POPULATION REFERENCE BUREAU Behavior and Global Health “Health is a state of complete physical, psychological, and social well-being and not simply the absence of disease or infirmity.” (World Health Organization, 1948) • Physical good health eludes billions of people • Death and disease from preventable causes remain high • Behavior is a key factor in determining health © 2005 POPULATION REFERENCE BUREAU Ten Leading Risk Factors for Preventable Disease • Maternal and child underweight • Unsafe sex • High blood pressure • Tobacco • Alcohol • Unsafe water, poor sanitation, and hygiene • High cholesterol • Indoor smoke from solid fuels • Iron deficiency • High body mass index or overweight Source: WHO, World Health Report 2002: Reducing Risk, Promoting Healthy Life (Geneva: WHO, 2002), accessed online at www.who.int, on Nov. 15, 2004. © 2005 POPULATION REFERENCE BUREAU Whose Behavior is Responsible For… • • • • Maternal and child underweight Smoking and alcohol abuse Unsafe sex Unsafe water and lack of adequate sanitation © 2005 POPULATION REFERENCE BUREAU Maternal and Child Underweight • • • • Individuals (may resist nutrition education) Communities (male preference norms) Policymakers (fail to address poverty) Health planners and health workers (do not include nutrition programs for the poor) © 2005 POPULATION REFERENCE BUREAU Smoking and Alcohol Abuse • Individuals (choice) • Communities (norms regarding smoking) • Health policymakers • Legislators & tax assessors • Tobacco company executives • Decision-makers in marketing companies © 2005 POPULATION REFERENCE BUREAU Unsafe Sex • Individuals (abstinence, fidelity, condoms) • Communities (norms regarding male dominance and multiple partners) • Poverty (transactional sex for poor women) • Health policymakers and health workers (effective AIDS prevention programs) © 2005 POPULATION REFERENCE BUREAU Unsafe Water and Lack of Adequate Sanitation • Individuals (where they fetch water, boiling water, washing hands) • Communities (fatalism regarding diarrheal diseases, community latrines) • Governments (ignore or underfund safe water and sanitation needs) © 2005 POPULATION REFERENCE BUREAU Risky behaviors translate to diseases © 2005 POPULATION REFERENCE BUREAU Global Causes of Death Injuries Communicable diseases, maternal and perinatal conditions, and nutritional deficiencies 9% Noncommunicable diseases 31% 60% Source: WHO, World Health Report 2000—Health Systems: Improving Performance (Geneva: WHO, 2000). © 2005 POPULATION REFERENCE BUREAU Behavior change reduces risky behaviors © 2005 POPULATION REFERENCE BUREAU Health Promotion Means Changing Behavior at Multiple Levels A B C D E Individual: knowledge, attitudes, beliefs, personality Interpersonal: family, friends, peers Community: social networks, standards, norms Institutional: rules, policies, informal structures Public Policy: local policies related to healthy practices Source: Adapted from National Cancer Institute, Theory at a Glance: A Guide for Health Promotion (2003), available online at http://cancer.gov. © 2005 POPULATION REFERENCE BUREAU A: Individual-Oriented Models • Individual most basic unit of health promotion • Individual-level models components of broader-level theories and approaches • Models Stages of Change Model Health Belief Model © 2005 POPULATION REFERENCE BUREAU Stages of Change Model • Changing one’s behavior is a process, not an event • Individuals at different levels of change • Gear interventions to level of change Source: James O. Prochaska et al., “In Search of How People Change: Application to Addictive Behaviors,” American Psychologist 47, no. 9 (1992): 1102-14. © 2005 POPULATION REFERENCE BUREAU Stages of Change Model (cont.) Precontemplation Maintenance Action © 2005 POPULATION REFERENCE BUREAU Contemplation Decision Health Belief Model • Perceived susceptibility and severity of ill health • Perceived benefits and barriers to action • Cues to action • Self-efficacy Source: Irwin M. Rosenstock et al., “Social Learning Theory and the Health Belief Model,” Health Education Quarterly 15, no. 2 (1988): 175-85. © 2005 POPULATION REFERENCE BUREAU B: Interpersonal Level: Social Learning Theory • Interaction of individual factors, social environment, and experience • Reciprocal dynamic • Observational learning • Capability of performing desired behavior • Perception of self-efficacy Source: Albert Bandura, Social Foundations of Thought and Action (Englewood Cliffs, NJ: Prentice Hall, 1986). © 2005 POPULATION REFERENCE BUREAU Interpersonal Level: Social Learning Theory (cont.) • Three strategies for increasing self-efficacy Setting small, incremental goals Behavioral contracting: specifying goals and rewards Self-monitoring: feedback can reinforce determination to change (keep a diary) • Positive reinforcement: encouragement helps Source: Albert Bandura, Social Foundations of Thought and Action (Englewood Cliffs, NJ: Prentice Hall, 1986). © 2005 POPULATION REFERENCE BUREAU C: Community-Level Models • Analyze how social systems function • Mobilize communities, organizations, and policymakers • Use sound conceptual frameworks Community Mobilization Organizational Change Diffusion of Innovations Theory © 2005 POPULATION REFERENCE BUREAU Community Mobilization • Encompasses wider social and political contexts • Community members assess health risks, take action • Encourages empowerment, building on cultural strengths and involving disenfranchised groups Source: National Cancer Institute, Theory at a Glance: A Guide for Health Promotion: 18; Paolo Freire, Pedagogy of the Oppressed (New York: Continuum, 1970.); Saul Alinsky, Rules for Radicals: A Pragmatic Primer for Realistic Radicals (New York: Vintage Books, 1971; revised edition, 1989). © 2005 POPULATION REFERENCE BUREAU Organizational Change Organizational Stage Theory Organizational Development Theory Define problem Identify solutions Organizational structures Initiate action Allocate resources Implement Institutionalize © 2005 POPULATION REFERENCE BUREAU Worker behavior and motivation Diffusion of Innovations Theory • How new ideas, products, and behaviors become norms • All levels: individual, interpersonal, community, and organizational • Success determined by: nature of innovation, communication channels, adoption time, social system Source: Everett M. Rogers, Diffusion of Innovations, 4th ed. (New York: The Free Press, 1995). © 2005 POPULATION REFERENCE BUREAU Diffusion of Innovations (cont.) Nature of innovation • Relative advantage over what is being replaced • Compatible with values of intended users • Easy to use • Opportunity to try innovation • Tangible benefits © 2005 POPULATION REFERENCE BUREAU Diffusion of Innovations (cont.) Communication channels • Mass media (enhanced by listening groups, call-in opportunities, and face-to-face approaches) • Peers • Respected leaders © 2005 POPULATION REFERENCE BUREAU Diffusion of Innovations (cont.) Adoption time • Awareness Intention Adoption • Gradual • Movement through groups Pioneers Early adopters Masses © 2005 POPULATION REFERENCE BUREAU Change Diffusion of Innovations (cont.) Social system: • Identify influential networks to diffuse innovation: health systems, schools, religious and political groups, social clubs, unions, and informal associations • Identify opinion leaders, peers, and targeted media channels to diffuse innovations © 2005 POPULATION REFERENCE BUREAU Health Promotion © 2005 POPULATION REFERENCE BUREAU Health Promotion Tools • • • • • • Mass media Social marketing Community mobilization Health education Client-provider interactions Policy communication Source: Robert Hornik and Emile McAnany, “Mass Media and Fertility Change,” in Diffusion Processes and Fertility Transition: Selected Perspectives, ed. John Casterline (Washington, DC: National Academies Press, 2001): 208-39. © 2005 POPULATION REFERENCE BUREAU Behavior Change Successes • • • • Reducing malnutrition (micronutrient initiatives) Preventing malaria (insecticide-treated bednets) Helping children survive (breastfeeding) Improving maternal health (safe motherhood movement, emergency obstetric care) • Making family planning a norm (worldwide efforts) • Combating HIV/AIDS (Uganda program) © 2005 POPULATION REFERENCE BUREAU Combating HIV/AIDS in Uganda • Political support, multisectoral response • Decentralized behavior change campaigns • Focus on women and youth, stigma and discrimination • Mobilization of religious leaders • Confidential voluntary counseling and testing • Social marketing of condoms • Control and prevention of STIs Source: Edward C. Green, Rethinking AIDS Prevention: Learning from Successes in Developing Countries (Westport, CT: Praeger Publishers, 2003). © 2005 POPULATION REFERENCE BUREAU Health Promotion: Lessons Learned • • • • • • Research underlying causes Address contextual factors Identify and reach key actors at every level Involve stakeholders throughout process Use sound behavioral theories Monitor and evaluate © 2005 POPULATION REFERENCE BUREAU Conclusion • Improving global health requires behavior change at every level—individuals, families, communities, organizations, and policymaking bodies • Evidence-based behavioral theories and successful behavior-change case histories point the way • Next step: political will and sufficient resources © 2005 POPULATION REFERENCE BUREAU For More Information Elaine M. Murphy, “Promoting Healthy Behavior,” Health Bulletin 2 (Washington, DC: Population Reference Bureau, 2005). Available online at www.prb.org © 2005 POPULATION REFERENCE BUREAU