Constipation - University of Manitoba
advertisement

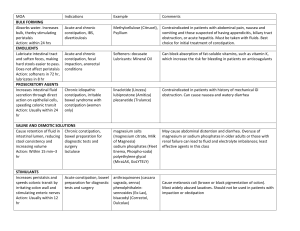
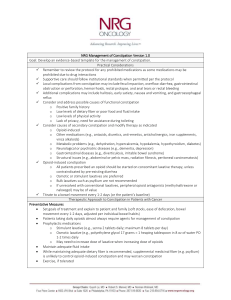
Management of Constipation in Family Medicine Meera Kaur, PhD, RD, CDE Assistant Professor, Family Medicine University of Manitoba, Canada http://home.cc.umanitoba.ca/~kaur/ Case 76 year old female with PMHx of HTN & DM-2, presents to the clinic. She’s complaining of having stools only twice a week, and feeling “full.” She’s eating more vegetables, started drinking more water, and she recently included Metamucil to her diet. Her last colonoscopy one year ago was clean. She comes to your office to be evaluated for her constipation. What would you offer her for the constipation? - A. Lactulose - B. Senna - C. Docusate - D. Weekly tap water enemas 15 What is constipation? • Is a symptom, not a disease • Is a condition in which a person has fewer than three bowel movements a week or has bowel movements with stools that are hard, dry, and small, making them painful or difficult to pass • Has varied meanings for different individuals, patients and care givers It is best when the stools are soft and passed at an hour customary to the patients when in health Hippocrates 2 Patients definition & concept about constipation • Patients’ Definition – Straining 52%, hard stools 44%, infrequent stool 32% • Misconception – 62% believe that daily defecation is necessary to good digestive health Ala, 2006 3 Rome III Criteria • Rome III criteria: 2 of the below defines constipation – Straining – Lumpy Hard Stools – Incomplete Evacuation – Use of Digital Rectal Maneuvers – Sensation of Anorectal Blockage – < 3 Bowel Movements per week 4 Diagnosis • Good history is enough for most cases – Duration, frequency, Consistency, blood in the stool, weight loss, Diet, Exercise, Toilet habits, Laxative use (what), other drugs • Basic laboratory test – CBC, Electrolytes, BS, BUN, Cr, TSH • Structural – Barium enema – Sigmoidoscopy – Colonoscopy 5 Causes • Primary cause – Primary Colorectal dysfunction – Slow Transit – Dyssnerygic Defecation – Irritable Bowel Syndrome • Secondary cause – Endocrine/Metabolic – Neurologic – Myogenic Disorders – Medications – Obstruction • Chronic Idiopathic Constipation (CIC) 6 Management… • Initial Management of chronic functional constipation – Lifestyle changes • Exercise • Establishing regular bowel regimen pattern • Early rising from bed – Diet • High fibre (20-35 g/day including both soluble and insoluble components) • ↑ Fluid intake • ↓ soft drinks, caffeinated drink 7 Management…Medication… • Bulk forming agent – Metamucil – Citrucel – Konsyl – Serutan • Osmotic agent – Milk of Magnesia – – – – Fleet Phospho-Soda Sorbitol Cephulac Miralax 8 Management…Medication… • Stool Softener – Colace – Docusate – Surfak • Lubricants – Fleet – Zymenol 9 Management…Medication… • Stimulant – Correctol – Dulcolax – Purge – Senokot • Chloride Channel Blockers – Lubiprostone (Amitiza) 10 Management • Surgery • Biofeedback • Alternative and Complementary Medicine – Yoga – Warm water + Honey – Herbal preparation – Homeopathic and Ayurvedic treatment 11 Complication • Hemorrhoid • Anal Fissures • Rectal Prolapse • Fecal Impaction 12 13 References • Books • Journal articles published during 1990-2012 • International, National and Provincial governments’ • • • relevant websites Regulatory organizations’ websites and reports Other relevant organizations’ publications/reports Guidelines, and References are available on request 14 Thank you 15 Summary Constipation in the older adult may be due to chronic constipation, secondary etiologic factors A thorough history must be obtained to rule out secondary causes. Therapy includes: Diet/lifestyle Stimulant Laxatives Osmotic Laxatives Bulk Forming agents Other therapy 15 Questions? 16