ISALUS EMR Cheat Sheet
advertisement

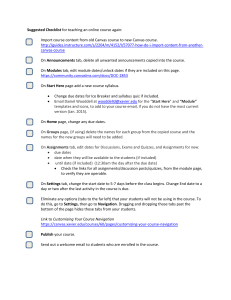
ISALUS EMR Cheat Sheet The highlighted sections are what you will see on your desk top in the EMR section Allergies Patient History Vitals ← Medications Problem List Immunizations Encounter History These tabs allow you to bring up a history of previous visits. Ex: if you open the Patient History tab and hit display history it will pull up all the previous patient histories that have been completed. Chart Tabs: Summary Vitals Allergies History ROS Exams Order Entry Problem List Prescriptions Immunizations HPI Treatment Plan The Chart Tabs allow you to enter information for the specific day that you are seeing the patient Chart Tabs: This is where information for the patient’s visit is recorded. Info needs to be recorded in order (vitals through treatment plan). The summary tab accumulates the info you are entering and allows you a brief snap shot of what is happening throughout the visit. As you enter info the tabs above and to the left will begin to fill with the info you are entering. Below is the info that MUST be completed under each of the chart tabs. You will see that there is a lot more information that can be recorded in each chart tab. This section of ISALUS could not be changed to meet our specific needs so the information that is not pertinent to us can be left BLANK. If you record the information it will end up on the SOAP Note which we do not want! Anything with a red * must be completed. Remember to use the Superbill to record data that needs to be inputted in multiple places. Vitals LMP Height, weight and BMI (BMI autocalculates) Blood pressure (include extremity and sit/stand) SAVE! Every time you complete a chart tab you have to push SAVE or your data will be erased! Allergies Add allergies by searching and choosing from the drop down list (no known allergies is in the drop down list). Cannot search using abbreviations! Once you add the allergen you must add at least one symptom. SAVE! History As you enter information into each of the tabs in this section it will auto populate the Summary tab at the top. Demographics: EVERYTHING must be completed in this section. Looks a lot like CVR info. Significant Illnesses: Self explanatory- check Hospitalizations: “No” and move on or Surgical History: check “yes” and record Disability History: the necessary info Dental Care: Social History: Complete only the following: Abuse, Tobacco use, Caffeine use, Recreational drug use, and ETOH use. Leave everything else BLANK. Family Medical History: Complete everything up to cause of death (COD). COD can be left BLANK. Menstrual/Obstetrical History: Complete ALL Sexual History: fields Contraceptive History: Immunization History: SAVE! ROS: Complete EVERYTHING SAVE! Exams: Templates: Scroll down to find the appropriate form for the visit. Complete ALL fields on them template. SAVE! Order Entry: Follow Up Visit: Enter (order) all necessary follow up visits. Referral: Enter (order) all necessary referrals you MUST choose whoever is at the front desk as the PROCESSOR (person who needs to perform the order)! In House Orders: Enter (order) all in house labs (UA, UPT, hemoglobin, etc) AND Gardasil and Rocephin injections (if being given during THIS visit). You have to assign a specific PROCESSOR. Labs: Enter (order) all labs that are processed outside of the clinic (pap, GC/CT, etc.). You have to assign a specific PROCESSOR. Breast Imaging: Enter (order) the procedure and assign a PROCESSOR. Other Orders: Enter (order) anything not listed above and assign a PROCESSOR (ex: Needs to have an ROI signed so we can get Pap results). SAVE! Problem List: Record patient problems by CPT Code by performing a search in the scroll down list. Left click over the problem to edit it (add notes, remove the problem, etc.) Alerts will appear next to the problem when applicable. SAVE! Prescriptions: Perform a drug search to find the medication (top left of the page). The following info has to be completed on the script WHEN WE ARE THE ORDERING CLINICIAN: o Drug (name and strength) o Dispensing qty and method (pack, tablet, ring, etc.) o Route and frequency o VOID Date (need to record void date as 13 months from original script date). o Patient Reported field should say “NO” (change by left clicking). The following needs to be completed to record medications that the patient is currently on from OTHER CLINICIANS: o Drug (name and strength if known) o Dispensing route and frequency (if known) o Patient Reported field should say “YES” (change by left clicking). SAVE! Immunizations: Use for Gardasil injections only HPI: More CVR date. Complete ALL SAVE! Treatment Plans: More CVR data Abnormal Lab Follow Up: Document all abnormal lab follow up. General Counseling and Education: Document counseling and education provided. Treatment Provided: Document what patient was treated for (only includes certain diagnosis). SAVE! Notes: * To record Lab results (in house or outside labs) you go into the EXAM Chart Tab and pull down the appropriate template: “Internal Lab Results”- to record in house results “External Lab Results”- to record PAP and GC/CT and any other labs sent out for processing. SAVE! After each enrty!