Mission: Lifeline® EMS 2016 Recognition Webinar Transcript
advertisement

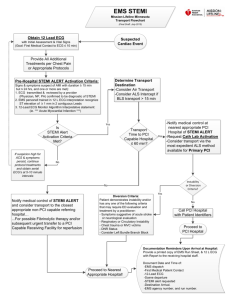
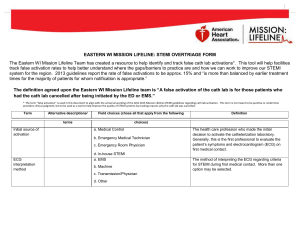
Mission: Lifeline® EMS 2016 Recognition Webinar Transcript December 2, 2015 Paul: Welcome and thank you all for standing by. At this time, all of our participants are in a listen only mode. For the Q&A session of today's call, if you would like to ask a question, please press * followed by the number 1. This call is also being recorded. If you have any objections, you may disconnect at this time. Now, I'm going to go over to your host, Mr. David Travis. Sir, you may now begin. David Travis: Well thank you very much Paul, and on behalf of the American Heart Association and Mission Lifeline, I want to thank you all for joining us on today's webinar on Mission: Lifeline EMS Recognition Program for 2016. My name is David Travis and I am the EMS manager for Mission Lifeline and we have some other panelists who are joining us today, Dr. Lee Garvey, who is a professor of emergency medicine from the Carolina Medical Center. Alex Kuhn, who is also with the American Heart Associate, is the Senior Director of Quality and Systems Improvement. Ben Leonard, also with the American Heart Association, the EMS Director in Mission Lifeline, Quality and Improvement Initiatives from Wyoming. And we have Joshua Roberts who is from Susquehanna Valley, EMS, in Pennsylvania. Just a few points about EMS recognition. The EMS Recognition Application period will open on January 1st and remain open through March 31st, 2016. The EMS Recognition for 2016 will remain focused on STEMI patients. There will likely be additional measure for stroke and resuscitation in the future, but for 2016, we have just been focusing on STEMI as we did in 2015. And in fact, the criteria for achievement for 2016 remains the same as for 2015. However, we have added new optional reporting measures for this year. So with today's webinar, Dr. Garvey will be discussing the importance of achieving First Medical Contact to device times of within 90 minutes or less. Alex Kuhn will be reviewing the EMS Recognition program overall and the criteria and the new reporting measures. Joshua Roberts will review the process his agency uses for gathering necessary data. And Ben Leonard will review the spreadsheet available for all agencies to use. And then we will have a period of open discussions and questions as time permits. So without further due, I'll introduce Dr. Lee Garvey. He is a professor of emergency medicine from Carolina's Medical Center, based out of Charlotte, North Carolina and a very long time Mission Lifeline volunteer. Thank you Dr. Garvey. Dr. Lee Garvey: Well thanks David. Welcome everyone to this webinar. I am delighted to be a participant and look forward to all of the good work you are doing and the recognition that is so well deserved. If we can help facilitate that today and answer any questions. That's my number one goal. If we could move to the background slide where the STEMI Point of Entry Protocol please. I think I could spend my entire allocated 15 minutes on this slide alone. I think it is one of the real punch lines and I would call attention to this anytime you're working on STEMI protocols. I think it really helps define where the important parts of the process are and how they are integrated together, how they overlap and our intent is to work in parallel, not sequentially or in serial processing. If you notice the ambulance is at the key center of of this diagram and we are going to focus a lot on the ERS role in providing Excellent care to STEMI patients, focusing on first medical contact and integrating with the hospital's reprefusion strategy. Next slide please. I think it's a very important slide here as well. To call your attention to the definitions that are used for the Mission Lifeline ERS Recognition strategy. Highlighted in red is the definition of first medical contact is the time of eye to eye contact between the STEMI patient and the first caregiver. So, if that caregiver is the first responder, under EMS, paramedic, physician at clinic and documented, that is what we use first. We'd like to know if its the first responder, whether or not, they are able to perform a 12 lead ECG, but that is the definition that we will be using for this program of ERS recognition. Next slide please. I think that just drawing your attention to the fact that these polls, community initiatives are now part of the guidelines published by the American Heart Association and the American College of Cardiology. It now acknowledges and it emphasizes how EMS is central to the community's performance on this critical measure. Even in the guidelines, it states that it can be. This performance can be facilitated by participating in programs such as Mission Lifeline and the Door to Balloon alliance and specifically wants to acknowledge the EMS recognition portion of this. Next slide. Also emphasizes that first medical contact, as we've defined it, until device time with the system goal of 90 minutes or less. To those patients who are taken directly from their first site of care to the PCL Center that is different for transferred patients. We will speak just very briefly about that at the end of this section if we have some time. 2016EMSRECEditMovie Page 2 of 20 But I think our country has adopted primarily PCL as a recommended measure of reperfusion when it can be performed in a timely manner, very very well. And a lot of hospitals are becoming very expert to the door to balloon portion of that and a lot of doors systems and community systems are really addressing how this can be established with destination protocols, integration, EMS services, and then hospital performance. Next slide please. I think that ... I mean, click through this a little bit, through the graphics of the fly-ins if you will. The doors to balloon, which has been such an emphasis over the last decades, almost is really solved. The door to balloon is no longer the measure that we need to watch. We are now much more focused on first medical contact to device time. How do we facilitate this? Or EMS delivered patients, just through the use of pre-hospital ECG. You can see over the years that we've been increasing our performance in these metrics as the systems have matured, more systems have been brought into the fold. Next side please. The slide EMS, the first medical contact to device here just outlines a few bullet points that I would like to emphasize. For the EMS component of this, it really begins with call capture, dispatch protocols response. Response times are what they are. It is a fact that it takes time to process the call, it takes some time to activate the responding, the first medical responders and or paramedics. We want to have that operated in a smooth manner as possible. That's work that you all do, and are familiar with, or not only STEMI, buT all sorts of other acute, highly acutely patients. But for the STEMI programs, the key piece of information is the pre-hospital 12 lead ECG. So having the skilled providers, being able to bring the device to the patient, acquire a 12 lead ECG, interpret that ECG in some manner, which we can talk about as well, and make a decision about the destination that is most appropriate for that STEMI patient is really key. I would say that that element is new to EMS in the last 10 or 15 years and really critical to the overall performance of STEMI systems of care. In an effort to maximize efficiency and again use parallel processing, not serial, sequential processing, the earlier the pre-hospital providers can notify and activate the receding cath lab, the better. There is some transportation time to seeing departure until hospital arrival or if you are going directly to cath lab to cath lab arrival that we need to use. The earliest time point that communication can occur between the pre-hospital providers who have made that diagnosis based on the 12 lead ECG and the receiving facility. We want that to be able to use that time to the best advantage at the receiving facility, to accommodate the scheduling, if it's a day time event or to recruit staff and to perform the cath lab procedures if it's a after hours event. Well we do want to minimize the seen time, we don't have much influence over transportation time. So we want to maximize the systems use of that transportation time however. As introduced, I 2016EMSRECEditMovie Page 3 of 20 practiced emergency medicine and I am one of the strongest believers I think that these patients don't need to come to the emergency department most of the time. If we can get an accurate appraisal of the patients clinical condition, an accurate interpretation of the ECG, early activation of the cath lab team, it's very appropriate for patients to go directly to a cath lab and even bypass the emergency department. Next slide please. Many successful and mature STEMI systems of care have developed such protocols and are working, and Mission Lifeline is working on this actively to assist, on developing protocols where EMS patients may go directly to the cath lab and bypass the emergency department when it's appropriate. We can talk about that a little bit more in the question and answer if we have the time. Next slide does outline a little bit of the criteria for ECG acquisition. Most of these STEMI protocols in the EMS world have criteria that are somewhat similar to this. This was published actually regarding patients who present to triage and how to select patients for an immediate ECG upon arrival. I think the same applies to those patients where EMS personnel encounter them and have to decide is this a patient who needs an ECG right away. So there are some aged based criteria. 30 years old with chest pain that is not obviously traumatic or 45 years older with either chest pain or these other potential inguinal equivalents of synchope weakness, palpitations, rapid heart, difficulty breathing and so forth. I think that's a useful scheme to use and would advise adopting this in your systems if you don't already a scheme in place for that. Next slide please. Again, the pre-hospital 12 lead ECG is the key piece of information and the information contained in that is crucial to the timely care of the STEMI patients presenting through the pre-hospital system. We get into the discussion about how the information ... Or how the decisions are made and how the diagnosis is made. There are a lot of options that are used in various programs from paramedics performing the interpretation and read independently or some systems use the ECG machine interpretation statement generation and act on those. Many systems I think use a combination that either uses the algorithm plus paramedic confirmation or a paramedic screening of appropriate cases and transmission or either a physician reader at online medical control or at there receding facility. Some systems are trying to transmit the ECG to all the decision makers. Through email distribution systems or some other commercial distribution system so that all the decision makers have access to the ECG imaging at the first opportunity. My personal opinion is that it's necessary to institute a system that meets your local requirements and equipment and expertise but then also to do a quality management program and see how many of these are being accurately interpreted. Is there any advantage to getting a different set of eyes on that and so forth. 2016EMSRECEditMovie Page 4 of 20 Next slide sort of outlines some of the work done across the state in North Carolina where we wanted to see how well we were performing on STEMI system activation. So of all those cath lab activations, we deemed about 85% of them were done appropriately. About 15% we would've considered inappropriate because the emergency department ECG was interpreted as STEMI originally and then reinterpreted as not or the EMS ECG was called STEMI and then later readers and decision makers decided it was not STEMI. Or something that is also new I think to EMS and emergency departments is considering how suitable a cath lab candidate is, this particular patient is. Generally speaking about 5% of the cath lab activations were cancelled or deemed inappropriate for each of those three red clocks of ED or EMS ECG or cath lab candidacy issues. What I am adovcating, whenever I get to work with a system is ... The next slide please. Is that, if there is a definite ECG STEMI diagnosis and the paramedics have confidence in that and the patient is a definite cath lab candidate then the entire system is activated immediately. If there are questions about either the ECG diagnosis or the cath lab candidacy, then a core group of individuals, whether that's the interventionalists and, or emergency physician with the EMS providers, makes decisions individually and then a decision is made whether to activate the entire system or not after there is a consultation and individualized decision making. I think a lot of systems are going to that block to activate the entire STEMI system when there is good confidence in the ECG diagnosis and the cath lab candidacy has been worked out. Certain things are in that are typical cath lab candidacy dis-qualifiers such as advanced directives indicating hospice or comfort care or non-intervention if there are other comorbidities that disqualify patients such as active hemorrhage or multiple severe system comorbidities, some of those things then may be individualized and decisions made that way. Will you look at the next slide, which is a stacked bar graph. I wanted to just talk a little bit about how we are using this information in system use. Each of these bars represents an individual hospital and the blue bars at the bottom are the first medical contact until hospital arrival. The tan bars in the middle are from the hospital arrival until cath lab arrival and then the green bars at the top are the time intervals for cath lab arrival until device deployment. Our emphasis today is on this entire stacked bar and our intent is to use the first medical contact until device, broken down this way, so we can maximize each of those efforts and minimize the time spent. Some of the most successful programs, even high volume programs, who are able to coordinate with their EMS providers and their cath labs, are able to minimize that tan bar in the middle where patients spend very little time in the emergency department, mainly because they have been using the time of transport, seen time, and transport time in the EMS world to prep their cath lab. You'll see most of those green bars at the top, the cath lab times are pretty close on generally speaking. There's a 2016EMSRECEditMovie Page 5 of 20 bit more variation in the tans bars so our intent is to use the EMS time to reduce the time necessary to spend in the emergency department. Next slide. I just wanted to mention STEMI transfers because I know a lot of EMS agencies are evolved in that process and we focus on door in, door out times. There are lots of issues there's that are outside the EMS responsibility but some of them have to do with transfer vehicle availability and crew response times. And also integrating the care from hospital one through the EMS transport agency to hospital two and limiting barriers such as IV, infused medicines, waiting for xrays and documentation. I think that are EMS colleagues can help a bit there but most of it is in having a system designed so that the EMS response to that first hospital is optimized. Next slide shows again, just a stacked bar graph for individual hospitals in a system where the blue bars on the bottom are door in, door out of hospital one time, transport time is the tan bar, and the green bars at the top are the time spent from arrival at the PCI center until reperfusion or device deployment. So for transport patients with EMS issues that door in, door out and transport time are our targets. With that I will switch to the last slide. My portion of the discussion, which I'll say is really just the background and hopefully most of it is very familiar to you. Just to kind of key it up for the rest of the presentations which are focused on specifics related to the Mission Lifeline EMS Recognition program. Again, its been my pleasure to participate in this and I look forward to the other presentations and further discussion. Thank you. Alex Kuhn: Thank you Dr. Garvey. This is Alex Kuhn with the American Heart Association. I know many of the folks on the line have probably from from me, seen emails from me, actually may have participated the past few years in recognition. I am certainly happy that you guys continue to explore opportunity and improvement. I'm going to run through the recognition measures and some other information related to the recognition program. But I know Dave and James from the HA will hop on here later and explain that there will be other opportunities for outreach related to the measures and completing successful applications and I know that you have local Mission Lifeline or quality directors in your region that will be eager to help you submit a successful application of your interest. Just quickly, it's always good to go a little back in history and this is the third year that the American Heart Association is doing the Mission Lifeline Recognition program. Last year in 2015, we had 450 agencies that we recognized. 123 bronze agencies, 239 silver agencies and 85 Gold agencies. To achieve recognition at those levels, which will be the same for this year. To achieve a bronze recognition you would have to have a 75% or higher on each of 2016EMSRECEditMovie Page 6 of 20 the compliance measures that we will share with you here in just a second, and at least two STEMI'S at least in one quarter, with the total a four STEMI in the calendar year for 2015. For agencies that got the silver, or are looking to get a silver this year, you would have to have again 75% compliance score on your recognition measures and I think eight STEMI’S in 2015. And for agencies that are looking to go for gold, or got gold last year, they had 24 month or two calendar years of meeting the minimum of 75% of each of the required measures and have at least eight STEMI’S and were silver the year prior. A couple different things, last year we also opened up really trying to expand, look at all the different individuals that potentially may be involved in the STEMI'S care and pre-hospital care and the STEMI'S patients. Really try to understand systems and the way that they work and accommodate the recognition to the multiple different systems designed. So again we are doing that again this year. We have three different categories that agencies can apply for. Again, we have an individual recognition and that's for a single applicant. These agencies must do the 12 lead ECG and transport the patient to STEMI receiving or a STEMI referral facility and meet the volume criteria and performance criteria. Then we also have a joint application, which is a dual application, where you may have one or both agencies do a 12 lead ECG and then transport the patient to a STEMI receiving center within 90 minutes. And both agencies must meet the performance criteria. Then a team application. A team application is one that ... You have one agency that may be a first responding agency or a BLS agency that doesn't have 12 lead ECG capability but may get dispatched initially to a patient, were the ALS agency is following up afterwards and doing the 12 lead ECG and then taking those patients to a STEMI receiving and a STEMI referral facility. So the three measures, and again the three measures are the ones that we had for the last 2 years. The first measure is the percentage of patients with nontraumatic chest pain over the age of 35 treated by EMS who get a pre-hospital 12 lead ECG. The second measure as percentage of steady patients with the first medical contact device within 90 minutes, and those are non-transfer patients. The third is the percentage of STEMI patients taken to a referral hospital who are administered fibrinolytic therapy with a door to needle time within 30 minutes. And again I know Dr. Garvey went over this, that you know we want to make sure that everybody understands what first medical contact is. We are looking at from the time that a patient with a STEMI has first contact with any medical care provider, a physician EMS personnel, they have to be a paramedic or EMT Basic first responder, anybody that is providing care to that patient initially is where we're starting the clock for first medical contact. So a lot of questions usually come up around which measures should I submit, and it really just kind of depends on where you are regionally and what kind of hospitals you are taking your patients to. If you are taking your hospital patients 2016EMSRECEditMovie Page 7 of 20 only to a hospital that is a STEMI receiving center and is going to do primary PCI then we are asking agencies to report on measures one and two. Again that is the percentage of patients that have pre-hospital ECG and then the first medical contact to primary PCI. If you are an agency that may be a little bit more rural and not have easy access to a hospital that has a primary PCI and you need to go to a hospital that may either transfer the patient or get fibrinolytic therapy we are asking those agencies to report on measures 1 and measures 3, which is the door to needle within 30 minutes. And then if you happen to be in the area where you have kind of a mix opportunity of taking patients to a semi receiving or a semi referral facility than you would report on all three measures. So just going into this a little bit deeper, I'm going to show what the numerators and the denominators are for each. And give you kind of a screenshot of what the application will look like online. For measure 1, again this is 12 lead ECG accusation, your denominator is the number of patients that you have over 35 with non-traumatic chest pain and again I get a lot of questions from folks about the other signs and symptoms of heart attacks and at this point we're just looking at those non-traumatic chest pains. The numerator would be the patient, the number of patients that get a 12 lead ECG. This is what the form looks like, if folks haven't seen the online form. We're going to ask you to count up quarter by quarter by quarter, how many patients you had that have had chest pain and then answer that in the denominator side section and then and then numerator section it will ask you how many of those patients received a 12 lead ECG. Measure 2, again this is first medical contact to device within 90 minutes your denominator, a little bit different than from a age perspective than a ECG acquisition, were looking at patients 18 and over that had a STEMI noted on the pre-hospital ECG and were transported to a STEMI receiving center and had primary PCI. So you'll have to figure out a lot of different information on that denominator to see who's included in that and then once you figure that out, then in your numerator how many of your patients had a primary PCI in less than 90 minutes. Again, very similar to measure one, we're going to ask you how many patients had, quarter by quarter by quarter, met that inclusion criteria. And how many patients, based on the denominator, met the first medical contact primary PCI within 90 minutes. There are some exclusion on outlier criteria that may come into play here. If you have a patient that is not giving consent, has cardiac arrest, can't get access, can't cross the lesion, those patients can be excluded and you'll want to collect those numbers from your hospitals because we will ask you to put that information in the form. The good thing here is that it will count towards your overall number of STEMI's that won't impact your denominator towards the overall percentage of meeting the first medical contact primary PCI within 90 minutes. 2016EMSRECEditMovie Page 8 of 20 Then, the third measure, is similar, is fibrinolytic administration in less than 30 minutes. Again, 18 years or over, transported to a referral center and had fibrinolytic administered are the denominator and the numerator are the number of patients that met that within 30 minutes. Again there are some criteria here for the exclusions and these include patients who can't get consent for the patient who are in cardiac arrest or needs intubation. This year we're adding some optional measures into this. Why we call them optional, that we highly encourage them. We are beginning to ask that EMS agencies to report the percentage of 12 lead ECG's for chest pain patients that are done within ten minutes of FMC. Another optional measure that we are asking agencies to report on is the time, in minutes, that the 75th percentile of hospital notifications are performed after the positive 12 lead capture. And then we're also asking for over triage and under triage or over activation or under activation the cath lab. So those were the measures. Fortunately there are good ways that hospitals are capturing this information that's helping agencies in their applications. Many hospitals in the US participate in the action [inaudible 00:31:05] the guidelines on why this data is being captured through that registry. So if you have good relationships with your hospital and your cath lab, you may be able to get this data right from them or some of the data from them to help you complete your application. A lot of hospitals now are providing some type of feedback form to EMS agencies with a lot of this critical data and so you should be able to get some of this information back from your hospitals that help you to complete your application. Shamelessly from Lehigh Valley here, they have actually done a lot more information, provided a lot more information from EMS agencies. They're providing FMC and pre-hospital ECG and they have a goal of actually having this done in less than five minutes. You can kind of see how this agency is meeting that criteria. Then as we talked about false activation, you can see that they are also providing out this information to their EMS agencies within their region to really help them understand the false activation rate is for their agencies. So just quickly as I'm wrapping up here. Go back to Deming here, without data, you're just another person with an opinion. The reason I say that is there are more and more folks looking at EMS data beyond the HA and this recognition program and I believe it's important for us to really do good data collection, to advance good quality care. 2016EMSRECEditMovie Page 9 of 20 We've been doing ECG's for a long time. We've been doing the first ECG's out in the field were done in 1967. The first time we began to see ECG's in the AHA's guidelines were in 1999. We saw that it is reasonable for paramedics to do 12 lead ECG's in 2004. Dr. Garvey and the [inaudible 00:33:00] group that wrote a paper for the federal government that said hey, we really should be having more ECG's in the field and by 2008, 90% of our cities have 12 lead capabilities. Then the most recent guidelines really begins to open it up more so not just for ALS providers but to all EMS providers to do 12 lead ECG's. Why I say that is again we've been doing advocate [inaudible 00:33:27] 12 lead ECG's since 1967. Really in about 2004, 2005, 2006 is when it became a standard of care for EMS providers to do 12 lead ECG's. But we still find that there are gaps in patients that are having chest pains, getting the 12 lead ECG. This is some data that I pulled. California's done a great job for measures reporting out and about 80% of their chest pain patients are getting 12 lead ECG's. Here in Ohio, and it's only about 60% of patients that are getting 12 lead ECG's. And then Dr. Garvey, I know that you were co-author on this paper down in North Carolina where you began to show some variability in patients that are getting ECG's that have chest pain. I'll let you jump in later on, maybe in the discussion as to what you were finding there. If you look at this from Ohio, if you're looking at 65% to California, 80%, that's a long way from 100. I always ask the question, for any 100%, is 99 good enough? I sold this from some of the six sigma stuff but looked at 99% being good enough, if that's the case then there would be 22,000 checks that were deducted from the wrong back account in the next 60 minutes. There would be 20,000 incorrect drug prescriptions that will be written wrong in the next 12 months and 12 babies that will be given to the wrong parents. While 99% is something that we should be aiming for, 100% should be really what we're aiming for. Based on our data, currently, we have a long way to go to get there. What does that really mean? I think at the end of the day, trying to improve outcomes of care. This is to me, a real opportunity to look inside the quality of your organization to identify opportunities to improve quality. Ben. Ben Leonard: Yeah. Thanks Alex. That's a great summation of what quality and improvement does and just listening to you present on some of those concepts really kind of tied it all together and it goes back into the concept that you really can't improve what you do not measure. Which in essence is the quality and improvement initiative. My name is Ben Leonard. I worked for the missions lifeline quality and improvement initiatives for the state of Wyoming. I also spend a little bit of time with the EMS agencies within the southwest region of the American Heart 2016EMSRECEditMovie Page 10 of 20 Association. I was asked to present on one of the data collections tools that was developed within some community work here on the AHA side of things. Alex, I think you need to switch control over to me. I don't have it quite yet. Knowing that there's a number of different PCR tools out in the EMS world, some are electronic, some are still utilizing the paper towels too. It's really hard to create a one size fits all program or process to in terms of collect this information. [inaudible 00:36:48] compliance is a great tool and there's some opportunity for that with the commentated definitions. But really what we want to be able to do is to assist agents agencies with the capabilities to collect this stuff if they don't have those other capabilities. What are group put together here, as my screen pops up. It's really a spreadsheet that's helped, designed to help track this information. A quick layout of the sheet is if you see this homepage here, it kind of puts down a processes to what we're trying to do. A little bit of the descriptors in terms of what the results what's true or include. But just really kind of an overview. The sheet itself is broken into three different tabs and those three tabs represent the three measures that Alex presented upon. If we go to this first tab, percent of ECG. In all three of these Tabs are outlines and put together in somewhat of the same fashion. These first three columns really kind of help you track information regards to patients, obviously the date of incident, the reporting quarter, it's got to drop down information that you can fill in. I also want to pressure that this tool is available on the website and by no means is it locked. What we want to be able to do is provide you with another option to collect this data. It doesn't have to be used in this fashion, you can take it, use it however you see fit to make it work for your service. Column C is patient identifiers and really that's just the way that you can track your patients when they go through your systems. So you can type in STEMI one or however you want to do it. The concept is to be able to filter these columns and so is Alex presented that the way the application tools split up into quarters, you can start to buy filtering your first quarter patients and be able to have that information readily available. Column D, E, and F, really define what the patient population in that denominator value is. Patient with A chief complaint of non traumatic chest pain you select yes, patient was transported yes, the patient was 35 years or older yes. You're going to get a result in this, column G that is true and this patient is counted in the denominator. I don't know about everybody else on the call, but in my years of working in EMS, I was lucky if I could put together a formulation in an Excel spreadsheet to add. Knowing the capabilities of this program is really great. So conceptually if you filtered on the reporting quarter, you can just basically highlight this line or this column and you come down in this count of 7, if you count all of these trues, that gives you that denominator. You can enter that into your application and go on to your next part. 2016EMSRECEditMovie Page 11 of 20 If we scroll over here to the side and I'll try to move the scroll bar slowly. I know having this go through on a webinar can potentially make you dizzy. We go to the next column here, H, was 12 lead acquired by this agency or department? You would select yes. What we want to do in this column I is track the date and time the FMC and a lot of the PCR's, you can get this information from. If you enter the date and time in the format of month, month, day, day and reported the year, and in military time, with the colon right there. That format is very very important. And the reason for that is if there's a formulation in there to do the time difference and we'll show you how that goes. FMC, you enter that into column I. In column J, date and time of your 12 lead acquisition. You can kind of see where these times are starting to track some of those optional reporting measures that Alex described in terms of FMC to 12 lead and what that percentage of time is. Once again, the numerator, based off of this column H. The patient did receive a 12 lead, that's going to change this to yes. Once again, we basically click and hold, highlight our columns here and you can see our count here is 7. As we would go as if these are the only patients in quarter one, we would be 7 out of 7. We'd be scoring 100% on that. Our next column over, was the heart team activated based from this positive STEMI or based from this positive ECG. If you select yes, the reperfusion strategy, and this really goes for those agencies that either potentially transport to both referral or PCI. You can start which ones you went to. As Dr. Garvey pointed out, it's possible PCI is finding the preferred method as long as it can be done in a timely fashion. If you have that opportunity, hopefully within your local system, you have those routing protocols in place, that's a good thing. Scrolling over again. What we want to do if that patient was activated, if the heart team was activated from this EKG, let's track the time for that. This might be one of those pieces of information that you get. Alex presented a very good example of feedback report that are available, hopefully with those actively involved systems so you'd be able to see what times the activation actually happened. Grab that information, put it in this column. Column Q actually starts to do some of these calculations here so with a time entry that we placed first medical contact EKG and minutes is basically the difference between the calling of the first medical contact time and then the 12 lead acquisition. That's the automatic calculation for that. Column R has the EKG to EMS request for heart team activation. And that's also in minutes. So once again that's the difference in time. For those who measures. Now if we scroll over to column S and column T, it really kind of does break down into those optional reporting measures. If you look at this little note here in order to get the 75th percentile. I put a note in there that you have to amend the second R value, the last field enter the data. So if you see this R value here, the first is R2 the second is R8. We have obviously 8 cells with data entry, so if we go through and there's 15 cells in the data entry, go down to R16, you want to change that number here. The same goes for column T, you want to be able 2016EMSRECEditMovie Page 12 of 20 to change the second Q value to the last Q cell that has data entered. That will give you the average time. It will also give you the 75th percentile for the EKG at cath lab, time activation. Lots of information this first page. So there is multiple ways for people to track their 12 lead acquisition rates. If you have something in place, by all means go for it. If you need ... We really encourage you all to track those additional measures that's going to help us in the future. That's kind of that first tab. The second two tabs kind really kind of go hand in hand with the concept of that first tab. The third tab I'll highlight really quickly, because it's kind of the same thing. Everything is laid out, numerator, denominator, you track your hospital and the time that you had first arrived to the facility because this is the door to needle time. You can actually get that obviously when you enter that into your PCR. All you have to do is get the time that the medication was administered. It does an automatic calculation and it goes through that same process, being an outlier, tracking if it needs one of the exclusions and then tracking that as an exclusion criteria. We have this available on the website. Please reach out to us if you have any further questions on this. I will actually take it back to Dave, I believe for any other questions. David Travis: Well thank you very much Ben and as Ben mentioned, we do have a number of tools on the Mission Lifeline website available to help you with Mission Lifeline EMS Recognition. We have a frequently asked questions field guide, this Excel tool that he just brief you on and also some other materials that will be helpful regarding the criteria and then you reporting measures and that's what it's saying. At this point ... James is Joshua available, as well? Ben Leonard: Yes. Dr. Should be online. Joshua Roberts: Good afternoon.. my name is Josh Roberts from [inaudible 00:49:33] Pennsylvania. [inaudible 00:49:35] EMS. If we can get to the overview page please. So compiling data for tracking of core clinical cases such as STEMI, cardiac arrest, CBA, and trauma, there are keys factors in an organizations ability to identify trends and evaluate areas for improvement. With electronic documentations software, becoming the norm across the nation, many agencies are utilizing the back end software components to capture this data. Which comes as a huge times savings, sparing the user from opening up each case and manually documenting the data components desired. Next slide please. 2016EMSRECEditMovie Page 13 of 20 The first step you have to take is identify what type of data you're looking for. Planning this out before tinkering with the software reporting system can make future data pulls quicker. So we need to establish the basics. The first one used is the date of event. If your software doesn't covert the data into the actual day you can use an Excel formula to make this happen. With our software, it pulls a lot of the data for us, but we have to actually key this into another Excel worksheet to make all of our formulas work. What we found without software, were using ESO currently, the information is there, but we can't modify it to the detail level that our organization expects. The thing with event, we use that day of the week to identify trends. It doesn't really have any effect on patient care but it certain can be defeminated to EMS providers on duty that a certain day is generally a higher frequency day of STEMI. Then we look at our patient demographics, a last name will use suffice, along with a patients age. We use the patients last name as an easy reference to obtain the outcome information from our local PCI centers. The age is an important factor in trend analysis. Municipality, sometimes obtaining this information can help you identify which areas of your response are a higher risk or have high rates of STEMI. For example, in Pennsylvania, we are a common wealth where we have different forms of [inaudible 00:51:38]. We have Burroughs, we have cities, townships, counties, other areas such as states with only have county based systems. You can break this down however you want it, whether it's by zip code or various municipality or incorporated towns and what now. We use this to do our community outreach programs. We can aim them more aggressively to certain areas that have higher rates of STEMI's at certain periods of time. In conjunction with other data, this is also able to assist in identifying response times and other factors that can lead to a better out come by better placement of EMS units. Next slide please. Here we're identifying event times. These are critical components of tracking every aspect of the call from start to finish. These include the time of dispatch, time of response, time of patient contact. The time of transport and receiving facility and between these various categories, you can identify the minutes to each component as necessary. I'll show you an example of our layout on the next slide. That's the basic layout of our time measurement. We perform calculations of how long it takes from the time of the 911 dispatch to patient contact. How long crews are spending on the scene. The time it takes for dispatch to arrive at the hospital when the time of patient contact when arriving to the hospital. We set up some very basic parameters to what we expect with the EMS providers. You can use Excel for a lot of different things with formulas and also conditional formatting. This is really important for the quality assurance aspect of it. So if you have certain parameters set up. For example on this screen, you'll see the 2016EMSRECEditMovie Page 14 of 20 total number of minutes from 911 to the patient, we have that set up. We do not want that to be any more than 15 minutes. Next slide please. Then we get into our STEMI factors and identifying those. What are we actually looking for as it relates to STEMI care? Here are some of the factors our organization uses to identify areas for improvement and to benefit the patients overall. The first one is the EMS STEMI type. This is useful so our QA managers can verify that the providers are calling the right types of STEMI In the field. Then we look at our leads and views. Was there a 12, 15, or 18 lead acquired? At a minimum 12 leads must be performed but then you can also add what times other 12 leads were obtained if the provider is going serial EKG's. Then we talk about which hospital was the patient taken to. When was the first 12 lead obtained and we can measure this to assure that ... Very common that aspirin is overlooked in the heat of things so we really focus on that, make sure that the aspirin is done within 5 minutes of patient contact. Next slide. This is an example of what type of STEMI the EMS has documented and based on that type we have conditional formatting to see if a 15 lead or 18 lead was necessary and if so why was it performed. You can see about 4 lines down, there was a patient with an infero posterior presentation. In that situation our provider would have been expected to do a 15 or and an 18 lead EKG which it was not. When we did the quality assurance on that, that was found to be the patient was actually one four minutes from the local hospital so it was more beneficial to get that patient through the doors of the ER. Next slide. This is our data table for various STEMI elements that we capture. Again, with the conditional formatting you can assure that each parameter is met when ever patient allowed this. You'll see highlighted in grey, where it says total minutes, that's a formula you can use. I found that Googling a lot of my answers for Excel formulas has been a great help, especially if you're not familiar. At the end of this if you have any questions on how we set that up, you can certainly ask me. This is one of the things that you want to set up well ahead of time and not be in the middle of tracking your STEMI's and figuring this out. Next slide. Now we get into the quality assurance, quality improvement aspect. Again, planning is always the key to a successful STEMI management system. We need to identify our goals from the beginning and build that system based on these goals. Which helps you concentrate the development and implementation effort without losing focus. Once you have your data build, incorporating quality 2016EMSRECEditMovie Page 15 of 20 assurance and improvement measures into the STEMI system is rather easy. Like we showed on the previous slide, with conditional formatting, you can quickly identify which parameters that were not met. Some of these examples include the time of 12 lead obtaining and transmissions, the time of aspirin on seen times, any additional lead views for various presentations and then the field accuracy of interpret ion by the EMS provider. Next slide. We're having some technology issues where I can't show you the QA worksheet. I'm not sure if it's up, I'm not even seeing the views right now. But we have a sample QA worksheet that our field training officers use with every single call that put through the QA and QI process. This ensures that all patients have data documented in the same ... Reports that come in, they go over the details of the PCR to ensure compliance to organizational standards and state protocols. Another piece of information that they have at their disposal is the actual transmitted EKG. You'll see that this is an example of a 12 lead that comes through, when its transmitted to the local PCI center that also comes to our educational managers email account. We save those and they can also be attached into the PCR software. When there's a code R that went we notify the organization and give kudos to the crew involved and then there recognized at the yearly banquet. If there's issues within the call the FTO will flag this for a medical review. That medical review goes to a medical advisory board that's made up of a captain, a lieutenant, the ALS and BLS FTO's, a medical director, and a chief of operations. So this is where the final determination is made as to remediating by either the providers platoon captain or a more formal discussion in person with our medical director. So each case gets 100% review and then that provider has a lot more feedback coming directly to them. Next slide. Obtaining data from the hospitals is rather easy once you have the process set up and its also part of developing that relationship with your local hospital or PCI center. We have two hospitals in our local area that do PCI's for us and they each have their own ways of sending out the information. So this is one of the data sheets that we receive. This information is mostly visual nature which are providers can easily see how the various processes measured up to the standards stat. For this one just happened a few days ago. There was a prehospital EKG and pre-hospital code R called. They got to the hospital at a certain time. This person actually was only at a total minutes of 70 from door to o, completed [inaudible 01:01:05] mid RCA. Next slide. 2016EMSRECEditMovie Page 16 of 20 Here's another data sheet from another PCI center. This one we really like a lot. Our providers seem to like this because it shows the before and after intervention pictures of the vessel. It also gives a lot more information as to the 911 dispatch information when [inaudible 01:01:28] access was made, what time the wire crossed the lesion when they got the balloon inflated or there was a [inaudible 01:01:33] performed and then the final outcome. Next slide. To wrap this up, studying the STEMI process is not really that difficult. Again, it all goes back to your appropriate planning and goal identification and that kind of leads the way as it relates to how were going to proceed. Working with your PCR software vendor to create custom reports is the key to pulling data and making sure your software works for you. There's so many different data systems out there nation wide. Its one of these things that you're going to have to work with IT people from your software company and see if you can get some of these customized reports built for you. Again you may have to manually enter that into your Excel worksheet or however you're going to map your data through Excel or Access or some other method. Unfortunately we have not found a tried and true method of simply just pulling this software data into our current management worksheet. It's very limited now that we've worked with our vendor to get this down to our level. The [inaudible 01:02:38] the call is of key importance to measuring your organizational goals against what is actually happening in the field and the constant monitoring of the process, ensure that each potential or recognized STEMI gets the same optimal care. So that concludes my section. I want to thank you for your time and thanks AJ for working so hard to improve and standardize STEMI care within the United States. David Travis: Well thank you very much Joshua and we have gone just a little bit on time here. We did make a request to have some additional time. Moderator are there some questions in queue? Paul: Let me just go ahead and inform your participants to ask a question. Please press star followed by the number one and to record your name clearly and slowly when prompted. Your name and introduce the question and to cancel just press star and two. I repeat one and star to ask a question. Thank you. David Travis: We did have one question come up about the application window. Again, the website will be available to accept applications starting January 1st and it will remain open through March 31st and again that is for calender year 2015 data to be entered for 2016 EMS recognition. We have an additional question on a webinar. Will there be any future webinars on EMS recognition. Yes, we are planning to have a webinar on January 27th, 2016EMSRECEditMovie Page 17 of 20 which will be a walk through of the applications for those who need some assistance with that. Do we have other questions moderator? Paul: Yes sir. We do have a couple of questions here so for the first one, this comes from the line of Steph Roberts and it the line is now open, you may proceed. Steph Roberts: I'm just looking for someone to clarify measure number two with the drop down of the 18 year old for the EKG. David Travis: Alex, would you like to handle that question. Alex Kuhn: Sure, I'll jump in here for a second and start it off and the other panelists can jump in here and also, especially Dr. Garvey. The two measures that are in there, frankly all three measures are based on the ECG, AHA guidelines. The 35 and over for chest pain, getting an ECG that is straight out of the guidelines and the 18 or over for FMC for primary PCI, again is straight out of the guidelines. I know there's some ... I know I run into a bunch of agencies where there's finding younger and younger patients having STEMI's it makes a lot of sense for probably doing ECG on younger patients but based on the way the guidelines are written, those are the ages that are in there. That's why there's a difference in the ages between the two. 18 and over for FMC to primary PCI, 35 and over for the ECG's. David Travis: Thank you Alex. Alex Kuhn: Yep. David Travis: Do we have another question? Paul: Yes sir. We do have the line for Mr. Anthony Cash on the line sir. The line is open, you may now proceed. Anthony Cash: Thank you very much. Regarding FMC, how do we account for when the patient is picked up at a facility such as a [inaudible 01:06:38]? David Travis: A skilled nursing facility is not counted. The time of the FMC is the time of the physician, the first responder, as such. The arrival time at a skilled nursing facility would be the time of FMC by EMS. The patient obviously would have been at the skilled nursing facility and it would be difficult to pinpoint exactly when the complaint occurred. So were talking about at a physican's office or at a clinic that first caregiver time when its available or the first responders time if its EMS. Anthony Cash: Okay thank you. 2016EMSRECEditMovie Page 18 of 20 David Travis: Sure thank you. Do we have another question? Paul: Yes sir. For the next question comes from the line of Jackie Holstrog. The line is open you may now proceed. Jackie Holstron: Hi, thanks for the information and taking my question. We have been submitting every year and our folks have been doing a great job winning the award. However, I have a couple small departments, rural departments that meet all the criteria except for the volume. For example, for the bronze, they must have at least two STEMI's per reporting quarter. They have a total of four throughout the year but not two in a quarter. I think what were doing is maybe limiting or cutting people out from winning awards that are doing a great job but from no fault of their own, don't have the volume. David Travis: And that is absolutely understood and that is a recurring issue on our feedback surveys when we ask respondents after the survey window, for any comments about the Mission Lifeline EMS Recognition program. That is probably the single most common complaint that we get, that we do have the volume requirements. Those volume requirements were set by our volunteer committee and they are in effect for 2016, you're absolutely correct, you have to have a minimum of at least four STEMI patients in a year and two have to be in a quarter and right now there is no plan to reduce that volume requirement or eliminate it, however that's something that the steering committee and cardiac sub-committee of Mission Lifeline will be evaluating in the future. We appreciate and are sympathetic to that issue. Paul: For the next question, this comes from Ms. Michelle Mayor, mam the lines are open you may not proceed. Michelle Mayor: Yes, my question was actually the same of the last individual's. We are first responders are true first responders not capable of doing a 12 lead EKG and I thought my understand of first medical contact last year was the provider that could actually perform a 12 lead EKG and our first responders actually don't always capture that eye to eye time so I wasn't sure how to go about reporting it if they don't always capture that information. David Travis: Right. The way its laid out, and there was some contradictory information about that measure last year, about that first medical contact, but the way it is laid out it's available, that's the time you should use. So if you don't have that time then you could use your agencies arrival time. Michelle Mayor: Okay. David Travis: It's preferred to have the FMC be that responders time but its understood that may not always be available. Michelle Mayor: Okay. Thank you. 2016EMSRECEditMovie Page 19 of 20 David Travis: Thank you. Moderator any addition questions. Paul: Sir right now there are no questions on the queue. David Travis: Okay. Well if we don't have any questions, those of you who are remaining on the line, if you questions that you think about or that you didn't get an opportunity to ask you can certainly email me directly at david.travis@heart.org that's david.travis@heart.org and I will follow up with you. Additionally there is information on the website if you go to heart.org/missionlifeline, you will see EMS recognition and there a lot of tools available to you there as well. Again on behalf of the American Heart Associate and Mission Lifeline, I wuld like to thank all of my panelists for being on today, for all there wonderful presentations and also thank all of you who participated in this and we look forward to your participation in Mission Lifeline EMS recognition for 2016. Thank you very much. 2016EMSRECEditMovie Page 20 of 20