PQI-Plan-March-2015
advertisement

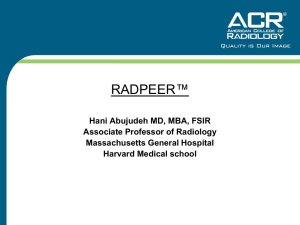
FATHER MALONEY’S BOYS AND GIRLS HAVEN PERFORMANCE AND QUALITY IMPROVEMENT PLAN I. Introduction A. PQI Philosophy The mission of Boys and Girls Haven is to shelter, heal and teach struggling young people to become productive and healthy members of our community. We continuously strive to fulfill our mission and provide the highest quality of care to our clients, their families and our community. We accomplish this, in part, through the implementation of a Performance and Quality Improvement (PQI) plan. This plan: Promotes excellence and mission-driven action throughout the agency Involves clients, staff members, stakeholders and other relevant parties in the PQI process Utilizes data to assess the performance of individual programs, departments and the agency as a whole Encourages continuous improvement across all services and programs offered by Boys and Girls Haven Supports the strategic priorities, goals and objectives of the agency. B. PQI Structure Teams and Committees Teams and committees play an integral role in the implementation of our PQI plan. Descriptions of these teams and committees are provided below: All Staff: “All staff” meetings are held at least six times per year. These meetings include all employees and are facilitated by the CEO. Directors provide reports relevant to their departments. During these meetings, PQI information is provided to the employees. The employees also have the opportunity to share information and provide feedback to agency leaders. Program Teams: Program teams are comprised of staff members of agency programs. Program teams are led by Program Supervisors and Program Managers. These teams oversee efforts to improve service delivery within their respective programs. Each program team helps identify opportunities to enhance the overall quality of services for our consumers. Program teams communicate PQI information to their supervisors or managers, who then share that information with others in the agency. Program teams meet at least twice per month. Risk Management Team: The Risk Management Team is comprised of the CEO, Directors, Associate Directors, Program Managers, Program Supervisors, the 1 Training/Recreation Supervisor, the Referral/Intake Coordinator and the Maintenance Supervisor. The Director of Programs & Operations is responsible for leading the Risk Management Team. This team is responsible for quarterly reviews of issues related to risk management. This team, or portions thereof, meet with greater frequency as needed to review safety concerns and risks as they arise. Case Record Review Team: A peer review team comprised of managers, supervisors, therapists, case managers, the Training Supervisor and Associate Director of Programs reviews client records on a quarterly basis. The Associate Director of Programs leads the case record review team. Client records are randomly chosen each quarter for review by the team. The number of records that are reviewed is based on a percentage of the total number of clients served per year, in accordance with COA standards. See Appendix A for a description of the agency’s case record review process. Leadership Team: This team is comprised of the CEO, Director of Programs and Operations, Director of Development, Director of Finance, Director of Human Resources, Associate Director of Programs, Program Managers, Referral/Intake Coordinator and the Training Supervisor. This team reviews information that is important to the daily operation of the agency, and makes plans to disseminate information and implement necessary changes. This team also reviews PQI information and assists with the implementation of performance improvement plans. Leadership Team meetings take place monthly. PQI Committee: The PQI Committee bears primary responsibility for implementing the agency’s PQI plan. It is chaired by the CEO or the Director of Programs and Operations. The PQI Committee includes Directors, Associate Directors, Program Supervisors, Program Managers, the Referral/Intake Coordinator and Training Supervisor. The Chair of the Board of Trustees may also choose to sit on this committee. This committee meets quarterly to review a wide range of data related to the performance of individual programs and the organization as a whole. Committee members identify potential opportunities for improvement, and initiate Performance Improvement Plans (PIPs) accordingly. The committee also reviews existing PIPs to determine if the desired outcomes have been achieved. Board Committees: Board Committees are comprised of members of the Board of Trustees, the CEO, one or more Directors and Associate Directors and select staff members. Each committee is led by one Board member who has volunteered to lead that committee and has an interest in that particular aspect of the agency. The Board committees include: Executive Committee, Governance Committee, Program Committee, Finance Committee, HR Committee, and PR/Development Committee. Committees meet at least four times per year. PQI reports are presented at committee meetings. Board members share feedback related to PQI that can be communicated to other teams and committees. Each Board committee also reports on relevant PQI activities to the full Board of Trustees. 2 Board of Trustees: The CEO reports on at least a quarterly basis to the Board of Trustees on the progress of the Performance and Quality Improvement Plan. During each meeting Board Committees report PQI information to the full Board to ensure that continuous quality improvement is a prime component of the Board’s activities. The Program Committee is primarily responsible for reviewing and reporting on program outcomes; however, all Board committees are involved in activities related to PQI. Any feedback from the board related to performance and quality improvement is documented and relayed by the CEO to the other teams and committees. Personnel Involved in PQI Activities The following chart lists individuals who are involved in carrying out the agencies PQI plan. Their roles and training necessary to carry out PQI activities are also identified: Title Board members PQI Roles Members of the Board of Trustees participate in meetings of the full Board as well as Board committee meetings. They review PQI information, offer feedback, and assist in identifying areas where performance/quality improvement is needed. Training Members of the Board receive a general orientation as well as orientation specific to the committees in which they will participate. During these orientations, their role in reviewing and disseminating PQI information is discussed. CEO The CEO is responsible for facilitating allstaff meetings and meetings of the Board of Trustees. The CEO also participates in Board committee meetings, Leadership Team meetings, Risk Management Team meetings and PQI Committee meetings. The CEO participates in trainings related to the PQI process through the Kentucky Children’s Alliance, the Center for Nonprofit Excellence and other non-profit organizations. In addition, the CEO engages in in webinars and self-paced trainings offered by COA. Directors Directors are responsible for leading the PQI Committee, Risk Management Team and Leadership Team. Directors also facilitate Board committee meetings and participate in all-staff meetings. Directors participate in trainings related to PQI through COA, as well as internal trainings offered by the agency’s Director of Programs & Operations. Directors also receive training that is relevant to their particular program areas. This includes training on the electronic medical records system, Microsoft Excel, data collection, data analysis, basic statistics and implementation of performance improvement plans. PQI trainings are provided by the agency upon 3 hire and on an annual basis. Associate Directors Associate Directors lead the Case Record Review Team. Associate Directors are also responsible for attending PQI Committee meetings, Risk Management Team meetings and Board committee meetings. Associate Directors also participate in allstaff and Leadership Team meetings. Associate Directors participate in trainings related to PQI through COA, as well as internal trainings facilitated by the Director of Programs & Operations. Associate Directors receive training that is relevant to their particular program areas. Training topics include the electronic medical records system, Microsoft Excel, data collection, data analysis, basic statistics and implementation of performance improvement plans. PQI trainings are provided by the agency upon hire and on an annual basis. Program Managers Program Managers are responsible for participating in all-staff meetings, Leadership Team meetings, Risk Management Team meetings, case record reviews, and PQI Committee meetings. Program Managers also work with the Program Supervisors to lead program team meetings. PQI trainings are provided by the agency upon hire and on an annual basis. Program Managers receive PQI training facilitated by the Director of Programs & Operations, and may also participate in webinars and selfpaced trainings offered by COA. They receive training relevant to their particular program areas. This includes training on the electronic medical records system, Microsoft Excel, data collection, data analysis and implementation of performance improvement plans. Program Supervisors Program Supervisors are responsible for participating in all-staff meetings, Leadership Team meetings, Risk Management Team meetings, case record reviews, and PQI Committee meetings. Program Supervisors also work with the Program Managers to lead program team meetings. PQI trainings are provided by the agency upon hire and on an annual basis. Managers receive PQI training facilitated by the Director of Programs & Operations, and may also participate in webinars and selfpaced trainings offered by COA. They receive training relevant to their particular program areas. This includes training on the electronic medical records system, Microsoft Excel, data 4 collection and performance improvement plans. PQI trainings are provided by the agency upon hire and on an annual basis. Support personnel receive PQI training facilitated by the Director of Programs & Operations, and may also participate in webinars and selfpaced trainings offered by COA. They receive training relevant to their particular program areas. This includes training on the Electronic medical records system, Microsoft Excel, data collection and data analysis. Support Personnel Support Personnel are responsible for participating in all-staff meetings, Leadership Team meetings, Risk Management Team meetings, case record reviews, and PQI Committee meetings. They also assist with gathering survey data and other information relevant to PQI. Staff members Staff members participate in all-staff meetings as well as program team meetings. Select staff members participate in case record reviews and Risk Management Team meetings. PQI trainings are provided by the agency upon hire and on an annual basis. Ongoing information regarding the PQI process is provided during program team meetings and all-staff meetings. Foster parents Foster parents participate in program meetings, trainings and events as members of the therapeutic foster care team. They provide direct feedback to staff members and complete stakeholder surveys. PQI information is shared with foster parents during the initial certification process. It is also reviewed on an annual basis. Staff members explain how feedback from foster parents contributes to the PQI process. Volunteers Volunteers participate in program meetings and agency events when appropriate. Volunteers may also participate in team and committee meetings. Volunteers are apprised of PQI activities and are asked to complete stakeholder surveys. The agency communicates PQI information through various means, including newsletters, annual reports, social media and the agency’s website. Volunteers are informed of the PQI plan during the orientation process. Volunteers are also encouraged to complete stakeholder surveys. Stakeholders The agency seeks feedback and input from stakeholders during every step of the PQI process. There is a continuous flow of information from stakeholders to the agency, and from the agency to stakeholders. Stakeholder feedback plays a crucial role in identifying opportunities for performance and quality improvement. The agency communicates PQI information through various means, including newsletters, annual reports, social media and the agency’s website. Solicitations for survey responses include information about how those responses will be used (e.g. 5 to support the PQI activities). Flow of PQI Information There is continuous circulation of information throughout all levels of the organization. See the chart entitled “Boys and Girls Haven: Flow of PQI Information” for a visual representation of how information flows between the teams, committees and stakeholders involved in the PQI process. C. Stakeholders Key stakeholders Boys and Girls Haven engages the following stakeholders in its PQI process: Referral sources (e.g. DCBS, DJJ) Judges/Court personnel Schools Clients Staff members Foster parents Volunteers Board members Donors Consultants Contractors Vendors Community partners Political figures Governmental organizations Private foundations Neighbors Involving stakeholders in PQI Boys and Girls Haven involves our stakeholders and consumers in our Performance and Quality Improvement Process through surveys to clients, Board members, parents/guardians, referral sources, staff, community partners and volunteers. Surveys are distributed at least annually to most stakeholders. Staff members participate in an annual employee survey. Client surveys are distributed quarterly. Stakeholder surveys are sent out with self-addressed stamped envelopes to encourage a higher rate of return. When possible, surveys are distributed and collected via electronic means (e.g. e-mail, Survey software). 6 Collected data is analyzed and used in conjunction with other external surveys used by licensing and regulating agencies (e.g. COA), to improve our overall quality and delivery of services to our consumers and community. Survey results are presented during PQI committee meetings and are used to develop performance improvement plans. Survey results, when appropriate, are shared with staff at every level of the organization. Boys and Girls Haven personnel receive regular feedback from stakeholders as they carry out their job duties. This feedback is used to identify opportunities to improve quality. Informal feedback can be shared with any staff member and then communicated to the various teams and committees that are involved in the PQI process. II. Measures and Outcomes A. Long-term Strategic Goals and Objectives Strategic Planning The strategic plan is revised every four years and is reviewed yearly by the Leadership Team and Board of Trustees. The strategic plan is updated regularly to take into account current trends, needs and opportunities. The strategic plan includes the following: Clarification of mission, values and mandates. Goals and objectives that flow from our mission and mandated responsibilities. An assessment of our strengths and weaknesses. An assessment of our human resource needs. Identification and formulation of strategies for meeting our identified goals. An assessment of our community, to include: Services offered by other providers. Gaps in our array of services Accessibility issues. A demographic profile of our community and consumers which includes: Annual household income. Gender Age Racial/ethnic composition Religious affiliation Language of choice The most recent update to the Boys and Girls Haven strategic plan was completed in August 2012. The agency’s current strategic goals and objectives are listed below: Goal 1: We will develop a comprehensive plan to address shortfalls in program funding 1.1 We will implement a strategy to identify and cultivate sustainable program prospects that address a core funding gap. 7 1.2 1.3 We will implement a strategy to identify and cultivate an additional $780,000 and expand private funding (i.e., a Wills and Trusts program). We will create overall plan and specific marketing plans for various special events. 1.4 We will implement a capital campaign. Goal 2: We will build community awareness and the visibility of Boys and Girls Haven’s services across the social service spectrum and community. 2.1 We will work to increase and expand local and statewide visibility. 2.2 We will engage community members by creating an Advisory Board. 2.3 We will create and engage a Speaker’s Bureau to promote BGH. 2.4 We will expand the Communications and Development Office staff to help promote BGH. Goal 3: We will develop a plan of action to meet our census goals. 3.1 We will develop new partnerships and strengthen existing partnerships with referral sources. We will secure alternate funding sources 3.2 3.3 3.4 We will adapt current programs and develop new programs to meet the needs of our referral sources We will assess the feasibility of expanding current facilities and/or building new facilities in order to meet programmatic needs Goal 4: We will develop and implement a comprehensive plan for recruitment and staff development. 4.1 We will develop and implement a workforce development plan to maximize output 4.2 We will develop a Compensation & Recognition philosophy & structure. 4.3 We will develop a succession plan for key employees. 4.4 We will develop HR metrics (to include baseline). 4.5 We will develop a plan to coordinate & recruit volunteers. We will develop a recruitment plan that uses diversified recruitment methods to attract & retain successful employees 4.6 Goal 5: We will monitor our operating plan and budget to achieve positive programmatic results, as well as financial accountability and programmatic sustainability. 5.1 We will implement a process for timely oversight of program financial performance. 5.2 We will implement a Continuous Quality Improvement Strategy. 5.3 We will implement a Critical Success/Risk Factor Report. Our PQI plan is aligned with our strategic plan. By engaging in activities that promote continuous performance and quality improvement, we accomplish the goals and objectives established in the strategic plan. The PQI process also informs future revisions of that plan. 8 Legal, regulatory and other mandates regarding measurements of outputs and outcomes Boys and Girls Haven’s intent is to demonstrate best practices in all areas of service delivery and organizational performance for the benefit of our consumers and stakeholders. We comply, to the best of our ability, with all applicable regulatory and licensing entities to whom we are responsible. These entities include the Kentucky Division of Regulated Childcare/ Office of Inspector General, Cabinet for Health and Family Services, Department of Juvenile Justice, Kentucky Department for Medicaid Services, Children’s Review Program, Kentucky Fire Marshall, Louisville (KY) Health Department, the Kentucky Transportation Cabinet and the Council on Accreditation. We are also must uphold the standards and expectations of all entities that fund the agency through public and private contributions. Our internal monitoring mechanisms and our overall Performance and Quality Improvement Plan ensure that we remain in compliance with legal, regulatory and other mandates. Outcomes and outputs related to these mandates are tracked and analyzed throughout the year. Results are presented during PQI Committee meetings, and performance improvement plans are initiated as necessary to promote compliance and positive outcomes/outputs. B. Management/Operational Performance Measures Boys and Girls Haven measures outputs and/or outcomes related to the organization’s capacity to manage and operate quality programs and services. The following outputs/outcomes related to management and operational performance are measured: 1. Staff retention a. Turnover rates for all employees b. Turnover rates for Youth Counselors c. Comparison of turnover rates to other, similar agencies 2. Staff injuries a. Number of injuries that did not lead to workers compensation claims b. Number of injuries that did lead to workers compensation claims 3. Employee survey responses a. Employees’ satisfaction with benefits and compensation b. Employees’ satisfaction with workplace c. Employees’ satisfaction with management/leadership d. Employees’ satisfaction with co-workers e. Employees’ suggestions 4. Performance of independent contractors 5. Financial performance a. Gross revenues by department and for the entire agency b. Net revenues by department and for the entire agency c. Actual expenses by department and for the entire agency 9 d. Comparison of budgeted revenues and actual revenues, by department and for the entire agency e. Comparison of budgeted revenues and actual revenues, by department and for the entire agency f. Total development revenue by source g. Comparison of budgeted development revenue and actual development revenue h. Ratio of expense to revenue for fundraising activities i. Indirect expenses by department and for the entire agency j. Utilization of endowment funds to cover operational expenses k. Performance of invested endowment funds C. Quality of Programs and Service Delivery Measures Boys and Girls Haven measures outputs and/or outcomes that are indicative of the overall quality of its services and programs. The following outputs/outcomes related to quality and performance are measured 1. Risk management data a. Number of physical managements b. Rate of physical managements per 100 days of service c. Number of critical incidents (including medication errors) d. Rate of critical incidents per 100 days of service e. Number of client grievances f. Number of CPS investigations involving staff 2. Client record review data a. Completion of essential documentation b. Quality of essential documentation c. Timeliness of essential documentation 3. Program outcomes data a. Number of clients served b. Number of clients discharged c. Duration of services d. Planned and unplanned discharges e. Outcomes for active clients f. Outcomes for discharged clients 4. Program/department census data a. Program/department demographics 5. Client survey responses a. Clients’ perceptions of quality b. Clients’ perceptions of safety c. Clients’ perceptions of effectiveness d. Clients’ suggestions 6. Stakeholder survey responses 10 a. Stakeholders’ perceptions of quality b. Stakeholders’ perceptions of effectiveness c. Stakeholders’ perceptions of visibility d. Stakeholders’ perceptions of community impact e. Stakeholders’ suggestions 7. Results of facility and physical plant inspections a. Ongoing facility and physical plant needs b. Emerging facility and physical plant needs c. Results of emergency drills 8. Findings from re-licensure audits a. Plans of correction resulting from audits 9. Findings from re-accreditation audits a. Plans of correction resulting from audits 10. Results of annual financial audits D. Client and Program Outcomes Measures Boys and Girls Haven measures outputs and/or outcomes that help the organization evaluate the impact of its services. The following client and program outputs/outcomes are measured: 1. Discharge reason 2. Discharge location 3. Clients discharged to appropriate, less restrictive settings 4. Number of adoptions 5. Progress towards treatment goals 6. Change in Child Behavior Checklist (CBCL) scores at discharge 7. Progress towards educational goals 8. Frequency of school disruptions 9. Frequency of legal entanglements 10. Participation in vocational activities 11. Number of clients completing life skills education 12. Number of clients securing employment Other outputs or outcomes may be tracked and analyzed as needed. Boys and Girls Haven collects data as required by funders. III. PQI Operational Procedures A. Data Collection and Aggregation Management/operational performance Data related to management/operational performance is collected from a variety of sources. That data is then aggregated into reports, which are utilized to further the PQI process. The 11 following reports contain essential PQI data: 1. 2. 3. 4. Quarterly HR Committee Reports Annual Contractor Performance Reports Annual Employee Survey Reports Monthly Finance Committee Reports See Section 2B of the PQI Plan for a list of the output/outcome measures included in these reports. Quality of programs and service delivery Data related to quality of programs and service delivery is aggregated into the following reports: 1. 2. 3. 4. 5. 6. 7. Quarterly Risk Management Reports Quarterly Client Record Review Reports Quarterly Program Outcomes Reports Quarterly Client Survey Reports Annual Stakeholder Survey Reports Monthly Facility Inspection Reports Annual Office of Inspector General (OIG) Statements of Deficiency and Related Plans of Correction 8. COA Accreditation Reports and Related Plans of Correction (Every Four Years) 9. Annual Financial Audit Reports Refer to Section 2C of the PQI plan for a list of the output/outcomes measures that are included in these reports. Client and program outcomes Data related to client and program outcomes is aggregated into the following reports: 1. Quarterly Program Outcome Reports 2. Reports for Grants and Foundations (Submitted When Required) See section 2D of the PQI plan for a list of the output/outcome measures that are included in these reports. B. Data Review and Analysis Data related to performance and quality improvement may be reviewed at any time, and at any level of the organization. Review of PQI data is ongoing, and may occur informally in order to provide information to staff members and/or initiate performance improvement activities quickly when the need arises. These PQI activities are promptly documented and communicated to other members of the organization. 12 Quarterly PQI Committee meetings serve as the primary venues for reviewing and analyzing PQI data at Boys and Girls Haven. During these meetings, members of the PQI Committee gather to review all relevant data. All teams and committees participate in PQI Committee meetings, so that all areas of the agency are represented. A representative of each team or committee reviews his/her respective report and invites feedback and discussion from the group. As the committee reviews data from a program or service area, there is honest discussion of its strengths and weaknesses. Ultimately, the committee works together to identify opportunities for improvement in each program and services area. Based on the feedback of the committee, the staff member responsible for that program or service areas then initiates one or more performance improvement plans. C. Using Data for Implementing Improvement Performance Improvement Plans When opportunities for performance and quality improvement are identified, staff members must initiate one or more Performance Improvement Plans (PIPs). The first step in developing a PIP involves working with your team to answer four questions: 1. 2. 3. 4. What are we trying to accomplish? What is the goal? How will we know that change is an improvement? What are the measureable outcomes we want to see? By answering these questions, the team begins to plan for change. The team then attempts to answer a fifth question: 5. What change will result in an improvement? To answer this question, the staff members follow five steps to achieve the desired outcome. The five steps are: a. b. c. d. e. Define the process currently in place Identify opportunities for improvement that exist Look for root causes of problems that have occurred Decide what you will change in the process Engage in Plan-Do-Study-Act cycles Finally, the team determines what intervention(s) will be implemented based on their analysis. Plan-Do-Study-Act (PDSA) Cycles A PDSA cycle allows the team to “test” change on a small scale to determine if that change will accomplish the desired goal or improvement. One PIP may require multiple PDSA cycles. 13 The components of each step in a PDSA cycle are listed below: 1. Plan a. b. c. d. e. f. g. What change are you hoping for? What do you predict will happen and why? What data will you collect and how? Who will be involved in this PDSA cycle? How long will the change take to implement? What resources will they need? Identify specific steps needed to test this change. 2. Do a. Carry out the test on a small scale. b. Document observations, including any problems and unexpected findings. c. Collect data you identified as needed during the “plan” stage. 3. Study a. b. c. d. Study and analyze the data. Determine if the change resulted in the expected outcome. What lessons were learned? Summarize what was learned. Look for: unintended consequences, surprises, successes, failures. 4. Act a. Based on what was learned from the test: b. Adapt: modify the changes and repeat PDSA cycle. c. Adopt: consider expanding the changes in your organization to additional residents, staff, and units. d. Abandon: change your approach and repeat PDSA cycle. Forms Boys and Girls Haven staff members must document PQI activities on the PIP* and PDSA* forms. These forms are attached to this document for reference. *These documents reference materials developed by the Centers for Medicare and Medicaid Services; http://www.cms.gov/Medicare/Provider-Enrollment-andCertification/QAPI/downloads/PDSACycledebedits.pdf D. Communicating Results PIPs and PDSA cycles should include staff members at all levels of the agency. A PIP may be initiated during a meeting of the PQI Committee; however, it can include key staff members who are not members of that committee. These staff members can assist in developing and 14 implementing the desired change. A PIP should trigger an exchange of information and feedback between multiple teams and committees. Once a team has engaged in a sufficient number of PDSA cycles, it can finalize the PIP. This occurs when interventions have been tested and there is sufficient evidence that those interventions will lead to the desired change. That change is then implemented on a larger scale, and becomes part of a new or revised policy/procedure. The results of the PIP and the new policy/procedure are communicated both internally (to clients, employees and Board members) and externally (to stakeholders). PQI information should always flow in a continuous loop between stakeholders, Board members and employees. Please see the chart entitled “Boys and Girls Haven: Flow of PQI Information” for a visual representation of this process. E. Assessment of the effectiveness of the PQI Process A Performance and Quality Improvement report will be developed annually by the PQI Committee. This report will summarize the outputs and outcomes that have been measured during the previous year, and will incorporate feedback from consumers, employees and other stakeholders. The report will be presented to the CEO, who will then present it to the Board of Trustees. The Board of Trustees will utilize the PQI report to inform the strategic planning process of setting short-term and long-term goals. Annually, or as needed, the PQI Committee will revise to the PQI Plan to incorporate feedback from the CEO and the Board of Trustees. F. Summary Through a process of continuous Performance and Quality Improvement, Boys and Girls Haven will maintain its standing as a premiere social service agency in Kentucky. We intend to meet the needs of our clients and fulfill our mission while being excellent stewards of our resources. Our Performance and Quality Improvement process will enable us to achieve these goals purposefully, efficiently and effectively. 15 Appendix A Case Record Review Process 1. Client record reviews are conducted quarterly. A peer review team comprised of managers, supervisors, therapists, case managers, the Training/Recreation Supervisor and Associate Director of Programs review client records. a. Client records are randomly chosen each quarter for peer review by the Training/Recreation Supervisor. A web-based randomization program is used to select the records. The number of client records reviewed in a given year is based on a percentage of the total number of clients served during the previous year, per COA standards. b. Program Managers/Supervisors receive lists of client records from the Training/Recreation Supervisor that will be reviewed. c. Program Managers/Supervisors ensure that all selected records are submitted for review. d. Staff will not review records for clients whom they currently serve, nor will they review records associated with their programs. e. The Client Record Review forms will be used to document the peer review process. Peer reviewers will use the forms that correspond to the programs that they are reviewing. i. Client Record Review forms must be completed in their entirety. Forms that are incomplete or not signed will be returned to the peer reviewer for completion. ii. Once a peer reviewer has finished the process of reviewing a record, he/she will return the completed form and the record to the Training/ Recreation Supervisor for data collection. f. Once a quarterly case record review is finished, Program Managers/Supervisors will ensure that all records are collected and returned to the proper storage areas. g. The Training/Recreation Supervisor will provide each Program Manager/Supervisor with copies of the Client Record Review forms for his/her program. i. Once a Program Manager or Program Supervisor receives the Client Record Review forms, he/she will inform staff members of the need to update and/or correct client records. Staff members will be responsible for making all necessary corrections, changes and/or updates within seven days. ii. The Program Manager or Program Supervisor will create a plan for updating and/or correcting each noncompliant record that describes actions taken to ensure that the record is in compliance with applicable standards and regulations. This plan can also explain why certain standards/regulations may not apply for that record. For example, a residential client who was discharged in less than 21 days would not be required to have a comprehensive treatment plan in his record. 16 iii. Within 14 days after Peer Review, the Program Manager or Program Supervisor will send copies of all updated/corrected plans to the Training/Recreation Supervisor. h. The Training/Recreation Supervisor will maintain updates and plans of correction for each program. The Training/Recreation Supervisor or his/her designee will also conduct random record reviews to verify that the updates and plans of correction have been implemented. 2. The Training/Recreation Supervisor will compile aggregate data after each Peer Review that indicates the level of compliance with applicable documentation standards for each program. All updates and corrections will also be noted on this quarterly Case Record Review report. Review data will be shared with the Leadership Team, PQI Committee, Program Committee, Board of Trustees and all other interested parties. 17 18 BOYS AND GIRLS HAVEN Performance Improvement Plan (PIP) Worksheet* Directions: Answer the first two questions below for your PIP. Then as you plan to test changes to meet your aim, answer question 3 below and plan, conduct, and document your PDSA cycles. Remember that a PIP will usually involve multiple PDSA cycles in order to achieve your aim. Use as many forms as you need to track your PDSA cycles. Model for Improvement: Three questions for improvement 1. What are we trying to accomplish? What is the goal? 2. How will we know that change is an improvement? Describe the measureable outcomes we want to see. 3. What change can we make that will result in an improvement? a. Define the processes currently in place b. Identify opportunities for improvement that exist c. Look for root causes of problems that have occurred d. Decide what you will change in the process e. Engage in PDSA cycles 4. Determine intervention(s) based on your analysis *This document references materials developed by the Centers for Medicare and Medicaid Services; www.cms.gov 19 BOYS AND GIRLS HAVEN PLAN-DO-STUDY-ACT TOOL* Program/Department: ________________________ Start Date: _______________________ Plan What change are you hoping for? What do you predict will happen and why? What data will you collect and how? Who will be involved in this PDSA cycle? How long will the change take to implement? What resources will they need? Identify specific steps needed to test this change. List your action steps along with person(s) responsible and time line(s). Do Carry out the test on a small scale. Document observations, including any problems and unexpected findings. Collect data you identified as needed during the “plan” stage. Describe what actually happened when you ran the test. 20 Study Study and analyze the data. Determine if the change resulted in the expected outcome. What lessons were learned? Summarize what was learned. Look for: unintended consequences, surprises, successes, failures. Act Based on what was learned from the test: Adapt: modify the changes and repeat PDSA cycle. Adopt: consider expanding the changes in your organization to additional residents, staff, and units. Abandon: change your approach and repeat PDSA cycle. Describe the measured results and how they compared to the predictions. Describe what modifications to the plan will be made for the next cycle from what you learned. *This document references materials developed by the Centers for Medicare and Medicaid Services; http://www.cms.gov/Medicare/Provider-Enrollment-andCertification/QAPI/downloads/PDSACycledebedits.pdf 21