Overview of Comp for students. 2014
advertisement

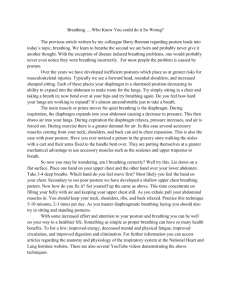
Medical Conditions I-DPTR 5301 Comprehensive Skills Outline I. There will be several case scenarios for the competency. II. Each student will have 15 minutes for the exam and 5 minutes to receive feedback from the instructor – 20 min total per student. III. When you draw a case scenario, you will be asked to explain and perform the examination and/or intervention techniques as outlined in the case. IV. The rubric will provides an “overview” of the grading that will be used for the competency (see page 2-4). V. For percussion/postural drainage, the instructor will tell you the diagnosis and area of the lung which needs to be addressed. You will be expected to assess breath sounds and “diagnostic” percussion before your intervention and after your intervention as indicated by the case. VI. For each scenario where the stethoscope is needed, you will be expected to “listen” with the diaphragm (breath sounds and normal heart sounds) and the bell (abnormal heart sounds). VII. For BP, you will be expected to perform the technique “by the book” – see below: assess the radial pulse and determine the radial occlusion pressure; deflate the cuff fully, identify the brachial pulse and then re-inflate the cuff to 30 mm Hg above the point where the radial pulse was occluded. Deflate the cuff in a controlled manner and determine the BP. Repeat if necessary (wait 1-2min btw) VIII. For cough or breathing techniques, your instructor will tell you which technique she would like for you to perform so be prepared to demonstrate any of them. IX. The scenarios can be either inpatient or outpatient so please practice with having your partner in gowns or in an outpatient setting where a patient may be wearing a tank top/jog bra. X. We will use the dual stethoscopes for BP, heart and lung sounds so please practice with these. They are in 3400 in the cabinet beside the sink, which should be unlocked. If you have problems accessing the stethoscopes, please let me know. XI. Please wear “lab attire” since access to the chest wall/ thorax is necessary XII. Please bring a watch with a second hand which allows you to assess HR and RR. 1 Example of Grading Rubric General – Communication 1. ______ Introduces self to patient 2. ______ Explains overview of encounter 3. ______ Obtains Patient Consent 4. ______ Uses patient appropriate language General - Positions and drapes the patient as needed 1. ______ Maintains modesty of patient 2. ______ Appropriate positioning 3. ______ Makes area of body available for examination/intervention Breath Sounds 1._______ Knows to use diaphragm directly on skin 2._______Student is systematic and uses proper anatomical positions – e.g.: auscultates at least 1 spot for each lobe bilaterally; listens top to bottom & left to right for comparison Auscultation o Listening Techniques/ Procedures: Sit patient up; roll patient – don’t just listen for the convenient sounds Breathe deep through mouth Stethoscope on skin Systematic comparison of L and R, and all lobes (goal is to auscultate at least 3-4 spots looking for SYMMETRY BILATERALLY) 4._______Listens at each spot, full cycle of inspiration & expiration 5._______Can explain normal breath sounds (bronchial (tubular/ tracheal); bronchovesicular; and vesicular) and knows where each should usually be auscultated 2 6. ______ Can explain abnormal breath sounds (e.g.: crackles, wheezing) particularly in the patient scenario provided (e.g.: surgical patient versus hypersecretion of mucus versus pneumonia …etc.). o Tracheal/Bronchial/Tubular BS Over Trachea Loud, high pitched, harsh E>I w/ short pause Heart in other location = abnormal (lung = consolidation (PNA)) o Bronchovesicular BS Sternum, scapula, anterior RUL I=E duration & loudness, no pause More muffled than bronchial o Vesicular BS Lung periphery I>E Medium pitch and loudness o Abnormal Breath sounds Bronchial or bronchovesicular in vesicular or more peripheral area consolidation, fluid Fluid transmits better than air Wheeze Hear on expiration Smaller airways = high pitched, larger = low pitched Caused by narrowed airways from secretions, edema, bronchospasm (airway collapsing when it should be open) Crackles Discontinuous notes “bubbling” “pop” “fizz” Hear on inspiration Large airways = low pitch = “coarse”, small = high pitch = “fine/Velcro” Diminished or absent BS Hyperinflation (air trapping), air/fluid/blood between lung and chest wall, airway blockage (mucus, tumor, foreign body), obesity Other info… o Normal I:E ratio = 1:2, obstructive = 1:3 or greater 3 o o Breath patterns Chyne-Stokes breathing: abnormal pattern w/ oscillation of ventilation between apnea and tachypnea w/ crescendo-decrescendo pattern in depth of respiration (HF, CVA, TBI, brain tumor) Kussmaul: consistent very deep breathing pattern at normal or increased rate (severe metabolic acidosis, form of hyperventilation) Fremitis Tactile Fremitis = palpable vibration produced during breathing cause by partial airway obstruction Mucus Secretions in airway Bronchial hyperreactivity/constriction, tumor Vocal fremitus Increased = consolidation, large airway secretions, pulmonary edema Decreased = pneumothorax, pleural effusion Heart Sounds 1.________Knows four locations (Aortic; Pulmonic; Tricuspid; Mitral) (1) (2) (3) (4) Aortic 2nd right ICS, right sternal border Pulmonic 2nd left ICS, left sternal border Tricuspid 5th left ICS, left sternal border Mitral 5th left ICS, mid clavicular line 2.________Uses diaphragm for S1, S2; bell for abnormal heart sounds (S3; S4; murmurs) 3.________Can explain what causes S1, S2 S1 = closure of AV valve S2 = closure of atrial semilunar valve 4.________Can explain what causes S3 S3: CHF – early diastolic sound = after S2 preceding S1 o S3 = HEART FAILURE (if managed well won’t hear this) o Low compliance of ventricles – S3 caused by crashing of blood into ventricles S4: s/p MI; HTN o S4 Happens very very late in diastole (just before S1) o Turbulence in atrium causing swishing but still caused by decreased compliance of the ventricles Blood Pressure: 1. _______ Assess the radial pulse and determine the radial occlusion pressure 2.________ Deflate the cuff fully, identify the brachial pulse and then re-inflate the cuff to 2030 mm Hg above the point where the radial pulse was occluded. 3. _______ Positions arm at level of heart & deflates the cuff in a controlled manner to determine the BP. 4.________Repeat if necessary Pulse palpation 4 1._______Can identify radial, carotid, dorsalis pedis pulses Check bilaterally, only 1 carotid at a time. 2._______Knows to extend time of palpation due to irregularity of rhythm if assessing pulse rate If irregular must assess apical pulse, and must assess for longer duration (30s-1min) 3. _______Can describe “quality” of pulse (regular/ irregular; strong, normal, thread) +4 = bounding +3 = full, increased +2 = normal +1 = diminished, weak 0 = absent (thread) Percussion (diagnostic) 1._______ Uses proper technique (see picture) Snap wrist At least 3-4 in front At least 3-4 in back Must make sure you assess upper, middle and lower. (back, side and front) 2._______ Can determine differences between normal resonance, hyperresonance (tympanic) and dullness 5 o (diaphragm descends to ~T7-T12) o Cause of changes in percussion Tympany Pneumothorax Air trapping (COPD) Dullness Consolidation (PNA) Atelectasis Pleural effusion Chest wall excursion 1._______ Assess in 3 places (see picture from lab PPT); can also asses laterally for anteriorposterior excursion 6 Upper chest – should feel pump handle 2. ______ Can offer hypotheses for chest wall asymmetry (e.g.: compliance changes; muscle guarding; pain …etc.) • • Deviates Towards • Atelectasis • Fibrosis Deviates Away • Pleural Effusion, • Tension Pneumothorax • (usually fatal) = hole in lung and there is no place for that air to go – no external injury, so air escapes from lung into interpleural space (disrupts pressure induced cardiac filling (R atrium, etc.) 1) Sides moving equally? Why not? a) Hemidiaphragm/paralysis b) Pneumothorax c) M splinting d) Reduced compliance (disease/surgery/scoliosis) e) PNA Airway Clearance Techniques (ACT) - Postural drainage, chest wall percussion & vibration 1._______Student can explain rational behind positioning and ACT Each position requires > 5min 2._______Demonstrates proper body mechanics for chest wall percussion (therapeutic): cupped hands (no slapping), primary motion from elbows and wrists; watch your back! Uses towel layer or sheet or shirt- do not percuss directly on patient’s skin • • performed throughout whole respiratory cycle – inspiration and expiration Perform for at least 5min 7 • • Precautions: osteoporosis, thin skin (cortisteroids) , blood thinners, PAIN, recent pacemaker ABSOLUTE CONTRAINDICATION – pulmonary hemmorage, unstable spine, consider head injury (increase in intracranial pressure), consider pulmonary embolism, consider recent incision for local contraindication 3. _______Demonstrates proper body mechanics for vibration: as vertical as possible over patient, get feedback from patient (i.e. have the patient say “eeeee”) when doing technique • • • Performed only on expiration Deep breath, hold for ~2sec, say “Eeeeee” on expiration as PT vibrates. Continue until remove secretions (decrease or remove crackles), or patient can no longer tolerate. (4-5 breaths) Creates external pressure and vibratory force through lungs to airways to promote movement of secretion 4. ______ Can describe and perform alternative interventions to assist with airway clearance (deep breathing/ incentive spirometry (role: open alveoli via pores of cone/lamberts canals); assisted cough techniques; lateral costal breathing; therapeutic exercises (UE/ LE/ mobilization …etc.) Huff Cough Step 1: Controlled (diaphragm) breathing through nose x 2-3 breaths One hand on upper and one hand on lower chest, assume/feel normal breathing Abdomen expansion Can provide pressure to thorax to teach. Step 2: Hold breath x 2-3 seconds (inspiratory hold) Step 3: Forceful expiration with “open glottis” Max expiratory flow = max airway clearance Active Cycle of Breathing (ACB) o Step 1: Controlled (diaphragm) breathing through nose x 2-3 breaths o Step 2: Deep breathing through the nose followed by a breath hold x 2-3 seconds (inspiratory hold) o Step 3: Huffing o Step 4: Repeat o Hazards Worsening SOB, hopoxemia, pain/injury to chest/spine, dysrhythmia, nausea/vomiting, bronchospasm Providing some pressure upward/inward (scooping) abdomen on expiration, can help activate diaphragm (provides stretch) Assisted Cough Techniques o Heimlich Cough Assist/ “Quad” cough Hand distal to xiphoid process but superior to umbilicus Coordinate with breathing pattern – “thrust” with onset of expiration/cough Costophrenic o Hands on costophrenic angles of lower ribs (lateral) o Follow breathing pattern 8 o As patient is beginning cough, apply pressure downward and medially Increasing abdominal content pressure. Indications/Goals for Airway Clearance Incications o >30mL sputum/day o Hypersecretion mucus o Ineffective mucociliary clearance o Ineffective cough o Immobility & weakness o Dysphagia/aspiration/gastroesophageal reflux Goals o Prevent accumulation, improve mobilization of secretions o Improve breathing through relaxation o Reduce symptoms of dyspnea o Improve CP Ex tolerance Outcome assessment o Increase or decrease sputum, improve symptoms, improve breath sounds, improve SpO2, improve CXR. Breathing Exercises and Breathing Retraining 1. ______ Can describe and perform breathing exercises including diaphragm breathing, deep breathing/ incentive spirometry; lateral costal breathing; segmental breathing 2. ______ Can describe and perform breathing retraining strategies including diagphram breathing combined with progressive postures/ mobilization – pacing of activities; pursed lip breathing 1. Facilitation of diaphragm Semi fowler position; knees bent; neutral spine ( posterior pelvic tilt); abdominals “relaxed” Sniffing i. Ask person to sniff (x3) - may facilitate diaphragm activity ii. After accomplishes the sniff, ask person to breath out slowly. “Scoop Technique” (s) i. Place hand over umbilicus and follow breathing pattern; apply gentle “overpressure” during expiration ii. At the end of expiration, give a slow stretch and “scoop” hand up and into thorax iii. Ask patient to “breathe into my hand” Coordinate diaphragm breathing with activities (supinesittingstanding ambulation) 2. Pursed lip breathing 3. Segmental & Lateral Costal Breathing techniques Lateral costal: place hands on lower ribs, laterally a. Use hands and quick stretch to promote breathing in a certain region b. Ex: atelectasis – want to augment airflow in this region Segmental: place hands over desired lung region – specific region 9 o If person sitting up can use your body as the “table top” laterally o Not resisting on inhalation. o Apply quick stretch on max expiration Ask patient to breathe into my hands – providing biofeedback. a. Don’t remove hand placement b/c want to provide that feedback Add PNF techniques such as “quick stretch” Cardiac &/ or Pulmonary Rehabilitation Principles (exercise prescription) 1. ______ Student can create & implement an exercise prescription for patients/clients with primary cardiac &/or pulmonary disorders including all components: mode; intensity; frequency; duration; progression Cardiac rehab o Exclusions Unstable angina Class IV heart failure Uncontrolled sustained tachyarrhythmias or bradyarrhythmias Symptomatic aortic or mitral stenosis Severe pulmonary hypertension Conditions that could be aggravated by exercise: Systolic BP >200 mm Hg or Diastolic BP > 100 mm Hg Suspected myocarditis or pericarditis Recent systemic or pulmonary embolus Infectious disease processes o Phase 1: Evaluate physiologic response to self-care/ambulation activity Goal 3-5METS HRrest + (20-30bpm) o Phase 2: Outpatient Typical Exercise Rx = HR rest + [(0.5 to 0.85)x(HR max - HR rest)] Lifestyle change – improve CV/P fitness safely, functional Pulmonary Rehab o Mode Aerobic – large muscle groups, rhythmic, Inspiratory m training Strength training LE UE UE/LE isotonic o Intensity – SYMPTOM PARAMETER %HRmax 60-90% HRmax or 50-85% VO2max RPE 10 o o o o High intensity (start 60% goal > 80% peak work rate) Duration Goal 30-40min continuously Intervals Frequency Goal: 3-5x/week If reduced duration/intensity increase frequency Progression – SYMPTOM BASED Assessment HR/ECG, BP, RPE, SpO2, Breath Sounds, (RR) Peak flow/spirometer, weight, JVD, heart sounds Pulmonary rehab does not change mortality – the number one change is symptoms. – no consistent improvement in pulmonary function. Ex capacity, m strength, dyspnea, fatigue, QOL 11 Pulm pathology Summary Pulmon o Restrictive lung disease Reduced expansion lung/chest wall Decreased compliance Dyspnea, tachypnea, hypoxemia, cyanosis (poor gas exchange) Types Pneumonia o Affects alveolar spaces and interstitial tissue Atelectasis Pneumothorax Pleural effusion Pulmonary Edema Idiopathic pulmonary fibrosis (pulmon interstitial disease) Pulmonary interstitial diseases o 2nd ary pulmon HTN, R heart failure (destruction vasculature) o Up FEV1 o Obstructive lung disease Reduced airflow during forced expiration from Airway narrowing Loss elastic recoil Dyspnea, wheezing, reduced ex capacity, +/- mucus production Types COPD o Hyperinflation o Chronic bronchitis, emphysema, and reactive airway disease Emphysema o Pink puffer o loss elasticity, destruction of air space and alveolar walls, wt loss o Hyperinflation, hypertrophy accessory m, clubbing digits, wheezing Bronchiectasis/Cystic Fibrosis o Lots of mucus plugging bronchiectasis and airway obstruction Chronic bronchitis o Blue bloater o Sputum production o R heart failure, DOE, dyspnea, hypercapnia, hypoxemia, cyanosis, o Pulmonary Exam 12 Accessory m. usage WOB Chest wall/thorax (scoliosis) Skin – incision/scar/bruises Cough Sputum Palpation 13 Inspection (Observation) Anterior view of the thorax ~ Rib # 4 RUL LUL RML RLL LLL 14 Posterior view of the thorax ~ Rib # 4-6 LUL RUL LLL RLL Diaphragm position: • Approx. T7 (@ FRC) & T10 (following VT) 15 16