Chest Exam
advertisement

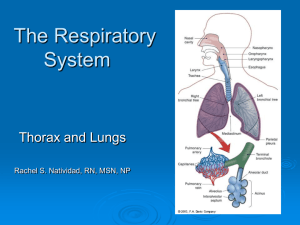
Examination of the Chest 2004 Examination of the Chest • Anatomic review • Brief survey of chest and respiration • Inspection • Palpation • Percussion • Auscultation Bony Structures of the Thorax Ribs 1-7 articulate w sternum 8-10 w costal cartilage 11-12 “floating” Costal cartilage Sternum Clavicles Scapula Thoracic vertebrae Content of the thoracic cavity: • Parietal pleura • Pleural space • Visceral pleura • Lungs • Mediastinum – Aorta, trachea, R and L mainstem bronchi, lymph nodes, vagus nerves, esophagus, heart • • • • Part of the liver Part of the spleen Part of the kidneys Part of the stomach Structure of Lungs Figure 16-10. p. 453. Slide 16-10 Mechanics of Respiration Figure 16-10. p. 454. Slide 16-11 Anterior Thoracic Cage Figure 16-1. p. 448. Slide 16-1 Posterior Thoracic Cage Figure 16-2. p. 449. Slide 16-2 Reference Lines Figure 16-3. p. 449. Slide 16-3 Vertebral, Scapular Lines Figure 16-4. p. 450. Slide 16-4 Anterior, Posterior, Midaxillary Figure 16-5. p. 450. Slide 16-5 Anterior Location of Lungs Figure 16-6. p. 451. Slide 16-6 Posterior Location of Lungs Figure 16-7. p. 451. Slide 16-7 Right Lateral Location of Lung Figure 16-8. p. 452. Slide 16-8 Left Lateral Location of Lung Figure 16-9. p. 452. Slide 16-9 Brief Survey of Chest and Respiration • Is the patient in distress? • Observe the rate, rhythm,and depth of respiration. • Audible sounds? • Respirations should be easy, quiet, and regular. Respiratory Inspection • AP diameter of chest as compared to the lateral diameter ( 1/3 to 1/2) ? Barrel chest • Sternal abnormalities pectus excavatum or pectus carinatum • Rate, depth, rhythm of respirations • Abnormal breathing patterns - Kussmaul • Skin color, clubbing • Spinal curvatures kyphosis, scoliosis, kyphoscoliosis Visual Examination of the Chest Breathing Patterns Rate, Depth, Regularity Normal Ataxic breathing Adults:12-20/min Infants: 44/min Biot’s breathing Irregularly irregular Tachypnea Rapid, shallow breathing Cheyne-Stokes breathing Regular rate, irregular depth MAY be normal Hyperypnea Rapid, deep breathing Hyperventilation Kussmaul breathing Sighs Bradypnea Hyperventilation syndrome 1 sigh per 200 breaths Configuration of Thorax Barrel Chest Normal Adult Pectus Excavatum Table 16-4. p. 483. Pectus Pectus Carinatum Cariatum Slide 16-25 Round Thorax in Infant Figure 16-25. p. 475. Configuration of Thorax Scoliosis Kyphosis Table 16-4. p. 484. Slide 16-26 Position of the Trachea Systemic Signs of Pulmonary Disease Clubbed Fingers Systemic Signs of Pulmonary Disease Cyanosis Systemic Signs of Pulmonary Disease Systemic Signs of Pulmonary Disease Clues to Increased Work of Breathing • • • • • • Nasal flaring. Intercostal/Supraclavicular retractions. Accessory muscle use. Pursed-lipped breathing. Disrupted speech. Thoraco-abdominal dissociation. Anterior Chest • • • • • • Inspection Palpation Expansion Tactile fremitus Percussion Auscultation Posterior Thorax • Inspect for: shape, symmetry, deformity, skin lesions • Palpate for tenderness or over any findings or abnormalities • Thoracic spine • CVA percussion • Respiratory expansion Posterior Chest • • • • Tactile fremitus Percussion Level of diaphragm Diaphragmatic excursion • Auscultation – Diaphragm – Apices downward – Compare side to side Symmetric Chest Expansion Figure 16-13. p. 461. Slide 16-12 Tactile Examination of the Chest Tactile fremitus • Palpable vibration of the chest wall from sounds transmitted from the phonating larynx. • “Ninety-nine.” • Compare symmetry. • Abnormality MAY be ‘ed or ‘ed. Tactile Fremitus Figure 16-14. p. 462. Slide 16-13 Assess Tactile Fremitus Figure 16-22. p. 472. Slide 16-21 Abnormal Tactile Fremitus Increased Tactile Fremitus Decreased Tactile Fremitus Rhonchal Fremitus Table 16-6. p. 485. Pleural Friction Fremitus Slide 16-28 Percussion • Systematic • Progress from apices to base • Side to side • Intensity, duration, and pitch • Normal = resonance • Note location of abnormalities PERCUSSION • RESONANCE - NL • HYPERRESONANCE - too much air such as emphysema or pneumothorax • DULLNESS - abnormal density due to possible pneumonia, pleural effusion, atelectasis or tumor Emphysema Consolidation Sequence for Percussion Figure 16-15. p. 463. Slide 16-14 Sequence for Percussion Figure 16-23. p. 473. Slide 16-22 Expected Percussion Notes – Posterior Chest Figure 16-16. p. 463. Slide 16-15 Expected Percussion Notes Figure 16-24. p. 473. Slide 16-23 Diaphragmatic Excursion Figure 16-17. p. 464. Slide 16-16 Auscultation • Listen for: – Intensity – Pitch – Duration • Normal breath sounds – Vesicular – Bronchial – Bronchovesicular • Adventitious sounds – Crackles – Wheezes – Rhonchi • Voice Sounds – Bronchophony – Egophony – Whispered pectoriloquy Breath Sounds Normal Adventitious (Vesicular, bronchovesicular (Inspiratory and/or expiratory) Transmitted Voice Sounds Bronchial, tracheal) Correct Location Incorrect Location Whispered pectoriloquy Discontinuous Continuous Wheezes Fine Coarse Crackles Crackles Rhonchi Bronchophony Egophony Auscultation of the Chest Surface Projections Auscultation of the Chest Examination Points = sites for both percussion & auscultation Breath Sounds •BS generated by movement of air thru the bronchial tree •Turbulence, vortex shedding (whirl pools), and oscillation and vibration of lung tissue Breath Sounds Normal Adventitious (Vesicular, bronchovesicular (Inspiratory and/or expiratory) Transmitted Voice Sounds Bronchial, tracheal) Correct Location Incorrect Location Whispered pectoriloquy Discontinuous Continuous Wheezes Fine Coarse Crackles Crackles Rhonchi Bronchophony Egophony Breath Sounds: Normal: Tracheal Tracheal • Inspiratory and expiratory sounds are about equal • Very loud • Relatively high pitched • Heard over trachea in the neck Breath Sounds: Normal: Bronchial Bronchial • Expiratory sounds are longer than inspiratory • Loud • Relatively high pitched • Heard over manubrium, if heard at all Breath Sounds: Normal: Vesicular (Alveolar) Vesicular • BS attenuated by air-filled parenchyma • Soft • Relatively low pitched • Heard over most of the lungs • Inspiratory sounds are longer than expiratory – Note: true expiratory phase is 2-3x longer than inspiratory phase Breath Sounds: Normal: Bronchovesicular BronchoVesicular • Inspiratory sounds and expiratory sounds about equal • Intermediate • Intermediate pitch • Heard often in the 1st and 2nd interspaces anteriorly and between the scapula Auscultation of the Chest Breath Sound Characteristics Intensity of Pitch of Duration Expiratory Expiratory of sounds Sounds Sounds Vescicular Inspiration > Expiration Relatively low Both lung fields Intermediate 1st & 2nd interspaces anteriorly; between scapulae Loud Relatively high Over manubrium (?) Very Loud Relatively high At sternal notch Softer Broncho- Inspiration Intermediate vescicular = Expiration Inspiration Bronchial < Expiration Tracheal Inspiration = Expiration “Normal” Location Breath Sounds Normal Adventitious (Vesicular, bronchovesicular (Inspiratory and/or expiratory) Transmitted Voice Sounds Bronchial, tracheal) Correct Location Incorrect Location Whispered pectoriloquy Discontinuous Continuous Wheezes Fine Coarse Crackles Crackles Rhonchi Bronchophony Egophony Stridor Inspiratory • Continuous • High pitched – Stidor Wheezes Expiratory • Continuous • High pitched, musical • Narow airways – Wheeze Rhonchi Expiratory • Continuous rattle; fluid in large airways • Low pitched – Rhonchi Crackles Short, popping; Sudden inflation of alveoli Early Crackles Fine Crackles Crackles heard In consolidation Pleural Friction Rub Grating, leathery; inflammed pleura Breath Sounds Normal Adventitious (Vesicular, bronchovesicular (Inspiratory and/or expiratory) Transmitted Voice Sounds Bronchial, tracheal) Correct Location Incorrect Location Whispered pectoriloquy Discontinuous Continuous Wheezes Fine Coarse Crackles Crackles Rhonchi Bronchophony Egophony Normal Voice Sounds • Voice-generated sounds radiate through the airways and lungs out through the chest wall and are heard well through the stethoscope. • They are best heard over the trachea and large airways but less well peripherally. • It is hard to understand individual words with the stethoscope, and with whispering, nothing is usually heard. Bronchophony: • Voice sounds are increased and clearer, even though one can not detect words. • Heard under similar circumstances as bronchial breath sounds, such as when there is consolidation of the lung but the airways leading into the consolidation are open. Whispered pectoriloquy • Pectoriloquy means “chest speaking.” • When a normal person whispers it is poorly heard with a stethoscope. • With whispered pectoriloquy one can hear words that are whispered with the stethoscope. This is usually heard under the same circumstances as bronchial breath sounds and broncophony has similar significance. • Normal Egophony • The word egophony means "goat sound" from the Greek root "ego" (goat). • This term describes a high-pitched bleating sound heard through an area of parenchymal consolidation Egophony: • When a normal individual says "E" it is heard under normal circumstances as an "E" with a stethoscope. • With egophony this "E" becomes "A" when listening through a stethoscope. • Usually heard under the same conditions as bronchial breath sounds and bronchophony and has similar meanings. Normal Egophony • Egophony is thought to be the most sensitive physical finding for consolidation. • Egophony may also occur over atelectatic or fibrotic regions of the lung, as well as above pleural effusions due to the upward compression of the lung by the underlying fluid. Common Respiratory Conditions Normal Lung Atelectasis Bronchitis Lobar Pneumonia Table 16-8. p. 486. Slide 16-29 Common Respiratory Conditions Asthma Emphysema Emphysema Pleural Effusion Congestive Heart Failure Slide 16-30 Table 16-8. p. 491-492. Putting It All Together Physical Signs in Selected Chest Disorders Trachea Percussion Note Breath Sounds Tactile Fremitus Adventitial Sounds Normal None Normal Decreased Wheezes Normal Midline Resonant Bronchial, Bronchovesicular, Vescicular Obstructive lung disease Midline Resonant Hyperresonant Normal Distant Lobar Consolidation To involved side Dull over involved site Bronchial over involved site Increased Late inspiratory crackles Pleural effusion From involved side Dull to flat over fluid Decreased to absent Decreased None (Pleural rub?) Pneumothorax To involved side Hyperresonant, Tympanitic over pleural air Decreased to absent Decreased None (Pleural rub?) Video Chest/Pulmonary Exam •Inspection, palpation (including tactile fremitus), percussion, auscultation of the posterior, lateral, and anterior chest. •Examination of the anterior chest may be conducted with the patient supine or sitting •Examination of the lateral chest may be incorporated into examination of the anterior and/or posterior chest Anterior Chest Anterior Chest (lying or sitting or at 30 0) 73. Inspection: For symmetry, fully exposed (in female patient may cover with gown as in photo) Anterior Chest 7Palpation: For tactile fremitus Palpation: Alternates from side to side or may use both hands simultaneously Anterior Chest: Percussion: 76-78 Percussion: Must be done: Bilaterally Symmetrically Good tone Must alternate from side to side Anterior Chest: Auscultation •(Starting above clavicles, 3-4 places, listens throughout inspiration and expiration) • Patient instructed slow, deep breath, mouth open • Auscultation: Alternates from side to side • Auscultation: At least 3-4 areas auscultated on each side Posterior Chest 84. Inspection: For symmetry Posterior Chest: Palpation A. B. A. Place hands on the patient’s posterior/lateral chest B.Ask the patient to take a deep breath Apply moderate pressure-- Your thumbs will move apart and the “dimple’ in the skin will go away Move hands up and towards the midline creating a “dimple” in the skin between the thumbs.- Feel and visualize the chest expanding Arrows denote direction of hand movement Posterior chest: Palpation :Tactile Fremitus Start above the scapula •Use the ulnar aspects of the hands •May use one hand and alternate from side to side or may use both hands moving inferiorly •Ask the pt to say “99” and feel the vibrations Posterior Chest--Percussion • Percussion: includes percussion, diaphragmatic excursion, and percussion over the costovertebral angle Percussion--(At level of the diaphragm) •This is done during normal (tidal) breathing •Start above the scapula •Alternate from side to side •Continue inferiorly until dullness of percussion occurs Posterior Chest-Percussion Percussion Diaphragmatic movement •Once the level of the diaphragm has been detected during tidal respiration ask the patient to take a deep breath and hold it •This will move the diaphragm more inferiorly Begin to percuss moving more inferiorly until dullness is encountered again •Begin to percuss moving more inferiorly until dullness is encountered again Repeat this process for the other side Percussion over costovertebral angle •Place the ball of one hand firmly over the patient’s costovertebral angle. •Use the ulnar side of your other hand to strike the hand you have placed on the patient. •Use enough force to cause a perceptible but painless jar or “thud” •Repeat on the opposite side Posterior Chest Auscultation: 92-96 •Patient needs to be in the correct position with arms folded and hands on opposite shoulders •Use the diaphragm of the stethoscope •Start above the scapula •Ask the patient to take deep breaths with his/her mouth open •Listen to complete inspiration and expiration •Move from side to side working your way inferiorly •Listen to at least 3-4 places