Acid – Base Physiology
advertisement

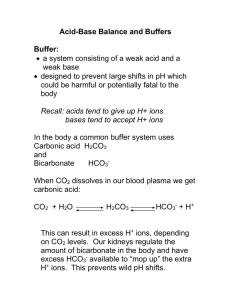
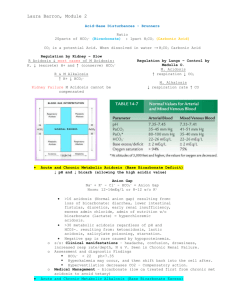
Acid-Base Physiology The pH of the body is controlled by 3 systems: 1. The chemical acid-base buffering by the body fluids that immediately combine with acids or base to prevent excessive changes in pH. 2. The respiratory center which regulates the removal of volatile CO2 as a gas in the expired air from the plasma and therefore also regulates bicarbonate (HCO3-) from the body fluids via the pulmonary circulation. This response occurs in minutes. 3. The kidneys which can excrete either acid or alkaline urine, thereby adjusting the pH of the blood. This response takes place over hours or even days, but represent a more powerful regulatory system. Acid-base Distrubances in the pH The abnormal loss of acid (as in vomiting gastric HCl) or addition of a weak base can lead to the condition of Metabolic Alkalosis: increasing pH above 7.4. In contrast, abnormal removal of HCO3- or another alkali or addition of acids other than CO2 or H2CO3 (as can happen in renal failure) can lead to Metabolic Acidosis: decreasing pH below 7.4. Since the pH of a CO2/HCO3- solution depends upon the ratio of these 2 buffer pairs, and because the lungs control CO2, but the kidney controls HCO3, the overall description of their interaction might be described as pH = k + KIDNEY / LUNG (Not a real reaction equation, but rather a descriptive relationship between the regulating components of pH in the body) Respiratory Acidosis is the inability of the lungs to eliminate CO2 efficiently; so the equilibrium shifts toward increased H+ and HCO3-; therefore, pH decreases. Respiratory Alkalosis is excessive loss of CO2 through ventilation driving the equilibrium to the left away from H+ therefore, pH increases. Respiratory Acidosis: CO2 + H2O H+ + HCO3- Respiratory Alkalosis: CO2 + H2O H+ + HCO3Normally, 1.2 M/L of CO2 is dissolved in plasma, which is a pCO2 of 40 mmHg. In biological systems, the total buffering of pH and the effects of acid-base disturbances is due to a complex interaction of many buffering systems, open and closed, with differing buffering capacities. all HB (n+1) H+ + all B (n) Predictions of the effects of these disturbances is done using a “Davenport Diagram.” Combining chemical buffers with CO2/HCO3 such that CO2 + H2O HCO3- + H+ + B(n) HB(n+1) Now, the final pH depends on two buffering pathways that affect the [H+] with two different equilibria equations. Davenport diagram: the blue curve is the pCO2 isobar represents the relationship between pH and HCO3 at a pCO2 of 40 mmHg. Orange line is in respiratory alkalosis (pCO2 = 20). The green line is respiratory acidosis. These occur due to changing pCO2 via altered respiratory function In the right panel. The red lines represent the influence of non CO2/HCO3- buffering systems. Point A1 would occur if these did not exist. Point A if these exist at 25 mM/pH (normal for whole blood) , and A2 if these buffering systems were infinite. Note that this red line to point A is shown in panel A and describes the changing buffer capacity of the non CO2/HCO3- systems during each respiratory disturbance. The Davenport Diagram is a nomogram to predict the different “disturbances” in acid base balance, based on the blood pH and the amount of HCO3in solution. Acidosis will shift the balance to the left, and alkalosis will shift it to the right. Since respiratory disturbances will shift the amount of HCO3- in solution the opposite of CO2, then respiratory acidosis will be in the top left, and respiratory alkalosis in the lower right corner of the nomogram. Partial pressures of CO2 Respiratory responses occur along this axis as the pH will be inversely related to the lungs ability to eliminate CO2 After the acute changes in buffering pH with chemical acid-base buffering systems, the LUNGS represent the second line of regulation of pH. Increased pCO2 will lead to a decrease in pH. The lungs ability to release CO2 from the blood allows it to regulate pH, as increased ventilation will vent CO2, increase pH by adjusting the [H+]. CO2 + H2O H+ + HCO3- CO2 is constantly formed in the cells as the by-product of metabolic processes. Therefore there is a constant need to get rid of it. If the metabolic formation of CO2 increases, the pCO2 increases, and the ventilation rate must increase to accommodate this change to try and bring the extracellular fluid into equilibrium. Also, the [H+] can affect the ventilation rate, since ventilation rate is directly stimulated by the pO2 because the pH directly affects the solubility of blood for O2. Increased pH decreases O2 and reflexively increases ventilation rate to increase O2 intake, thereby venting out CO2. Negative feedback loop of H+ and alveolar ventilation The respiratory buffering system is a buffering system with limited gain; ie, it can’t completely compensate for changes in pH (only 50-75% compensation), but the relative speed at which it can make significant changes in pH makes it efficient, and helps buffer pH changes until the renal excretion of acids and bases comes into play. Abnormalities in respiratory function reduce the efficiency of this buffering system (such as emphysema or a smokers lung) , and drive the body toward a constant state of respiratory acidosis. Cigarettes smoke also has a high concentration of CO2, making things even worse. Thus, in these conditions the body becomes heavily dependent on the ability of the kidney to compensate for the inability of the lungs to buffer excess H+. RENAL CONTROL OF ACID-BASE BALANCE The kidneys control acid-base balance by excreting either an acidic or basic urine. The kidney filters large volumes of HCO3- and the extent to which they are either excreted or reabsorbed determines the removal of “base” from the blood. The kidney secretes large numbers of H+ into the tubule lumen, thus removing H+ from the blood. The “gain” of the adjustment of pH by the kidney and the acid base balance it regulates is nearly infinite, which means that while it works relatively slowly, it can COMPLETELY correct for abnormalities in pH. The “metabolic” or renal regulation of the balance of H+ or HCO3- excreted will determine if there is a net loss of H+ or HCO3-, and will determine the pH of the urine. CO2 + H2O H+ + HCO3- Filtered Nephron Secreted Reabsorbed Note: the renal regulation of the equilibrium between H+ and CO2 takes place on the “right” side of the equation Urine (excreted) Overall, the kidneys must excrete H+ and prevent the loss of HCO3-. Filtered HCO3- must react with secreted H+ in order to be reabsorbed as H2CO3 The nephrons must secrete a total of 4,320 mEq of H+/day in order to complex with HCO3- to reabsorb (almost all of) it. In addition, an additional 80 mEq/day of H+ is secreted to facilitate the excretion of non-volatile acids (products of protein metabolism that can not be expired via the lung). Thus, the kidney must secrete a total of 4,400 mEq/day of H+ into the tubular fluid. The kidneys regulate extracellular fluid pH by secreting H+, reabsorbing HCO3-, and producing new HCO3During alkalosis, excess HCO3- is not bound by H+, and is excreted, effectively increasing H+ in the circulation and reversing the alkalosis. In acidosis, the kidneys reabsorb all the HCO3and produce additional HCO3-, which is all added back to the circulation to reverse the acidosis. H+ is secreted and HCO3- reabsorbed in all segments of the kidney except for the thin limbs of the loop of Henle. (however, HCO3- is not readily permeable through the luminal membrane). PROXIMAL H+ H+ is secreted via a Na-H countertransport process, coupled to the active movement of Na into the cell via the basalateral Na- K ATPase. HCO3- reabsorption is facilitated by the enhanced conversion of CO2 to H2CO3 (normally slow) via the enzyme carbonic anhydrase Reabsorbed as CO2 + H2O Complexed Secreted filtered H2CO3 H+ + HCO3- Once CO2 enters the cell, it can be quickly driven in the reverse reaction to form carbonic acid (normally very slow) due to the intracellular enzyme carbonic anhydrase) and this pushes the reaction to form HCO3- and H+ to be taken back into the Inside the cell; Carbonic anhydrase CO2 + H2O -------*--------> H2CO3 H+ + HCO3Secreted back Into the lumen Reabsorbed into the circulation Note; this process is all driven by the active transcellular movement of Na+ DISTAL H+ In the intercallated cells of the distal tubule, a H/Cl co-transport is involved with H+ secretion. The formation of H+ inside the cell provides a gradient for the secretion of more H+ into the lumen to complex with and reabsorb more HCO3This distal pathway accounts for only 5% of secreted H+ but the H+ gradient it can form is 900X so it is a major site for creating an acidic urine pH 4.5 In general (under “normal” conditions), the amount of HCO3filtered and the amount of H+ secreted are similar (they are said to “titrate” each other), though there is a slight excess of H+ secreted and excreted. This is not as H+, but rather complexing with other buffers such as phosphate or NH3 to be excreted. In metabolic alkalosis, the filtered HCO3- exceeds the secreted H+, and therefore the HCO3- is excreted in the urine (making it more alkaline). This loss of excess base will slowly correct the metabolic alkalosis. In metabolic acidosis, the excess secreted H+ results in total reabsorption of HCO3-, and the excess H+ is excreted in the urine (making it more acidic). This loss of excess acid will slowly correct the acidosis. The urine can only accommodate a small % of free H+ in solution, so much of the H+ to be excreted must complex with other buffering bases to facilitate its excretion. The major such buffers are phosphates and NH3, but other lesser buffers including urate and citrate also combine with H+ to get it out into the urine. The buffering of H+ by phosphate and urea in the tubular fluid also contribute to the generation of new HCO3-. Phosphate buffering and secretion of H+ The process of driving CO2 to secrete a H+ produces HCO3 de-novo AMMONIUM GENERATES HCO3- ** Ammonium (NH4+) is produced from the cellular metabolism of glutamine in all nephron segments. Ammonium is secreted into the lumen, and 2 HCO3ions are formed and reabsorbed ** NH3 buffers secreted H+ in the collecting duct Secreted H+ combines with NH3 which freely diffuses into the lumen from cells to complex with H+ in the lumen to form NH4+ which is trapped in the lumen and excreted. Again, the loss of a H+ from the cell creates denovo synthesis of a HCO3- molecule to be reabsorbed. Note that “metabolic acidosis and alkalosis move I an axis related to the ability of the kidney to reabsorb HCO3-. Acidosis occurs when plasma HCO3- is low, while alkalosis occurs when it is high and there the ratio to H+ in the nephron is also high. Metabolic Acidosis occurs when the kidneys fail to excrete acids formed in the body, or there is excess ingestion of acids, or the loss of bases from the body. Renal Tubular Acidosis: due to a defect in H+ secretion or HCO3- reabsroption. Diarrhea: Excess HCO3- loss into the feces without time to reabsorb (most common cause). Diabetes mellitus: In the absence of normal glucose metabolism the cells metabolize fats and form acetoacetic acid, reducing pH, and inducing renal acid wasting. Chronic renal failure: decreased renal function results in acid build-up in the circulation and reduced HCO3reabsorption. Acid ingestion: toxins such as aspirin or methyl alcohol result in excess acid formation. Metabolic Alkalosis: occurs when there is excess retention of HCO3- or excess loss of H+ from the body. Diuretic therapy: many diuretics increase tubular flow, resulting in increased Na load, increased Na reabsorption and therefore increased HCO3- reabsorption. Excess Aldosterone: which promotes excess Na reabsorption and stimulates H+ secretion. Vomiting: loss of the acidic contents of the stomach creates a depletion of H+ which is compensated for by removing more H+ from the circulation. Ingestion of alkaline drugs such as Na HCO3- used for upset stomachs and ulcers. Analysis of simple acid base disorders and how they are compensated for by the body.