Happy Friday!
advertisement

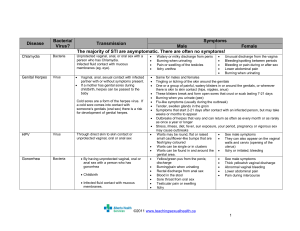
Good Morning Semantic Qualifiers Symptoms Acute /subacute Chronic Localized Diffuse Single Multiple Static Progressive Constant Intermittent Single Episode Problem Characteristics Ill-appearing/ Toxic Well-appearing/ Non-toxic Recurrent Localized problem Systemic problem Abrupt Gradual Acquired Congenital Severe Mild New problem Recurrence of old problem Painful Nonpainful Bilious Nonbilious Sharp/Stabbing Dull/Vague Illness Script Predisposing Conditions Age, gender, preceding events (trauma, viral illness, etc), medication use, past medical history (diagnoses, surgeries, etc) Pathophysiological Insult What is physically happening in the body, organisms involved, etc. Clinical Manifestations Signs and symptoms Labs and imaging Predisposing Conditions Adolescents/young adults African American, southeastern rural U.S. Multiple sexual partners Vaginal douching Untreated episode of GC or Chlamydia (10-40%) Past history of STD or previous PID Menstruation IUD Protective factors** Appropriate condom usage Other barrier protection Oral contraceptives** (decreases the risk by up to 7-fold) in face of gonococcal cervicitis Pathophysiology Ascending genital tract infection…”salpingooophoritis” Inflammation of: Endometrium Fallopian tubes Ovaries Peritoneum Organisms **Immature cervix More ectopy (exposed columnar epithelium) Further predisposing adolescents to the condition GC/Chlamydia (50% of cases) Other Bacteroides Peptostreptococcus Gardnerella vaginalis H. influenza Strep species Enteric GNR Genital Mycoplasms **Polymicrobial Clinical Manifestations** Lower abdominal pain, worse with movement Vaginal discharge Irregular bleeding Fever Nausea/vomiting Dyspareunia, dysmenorrhea, dysuria Physical Exam Cervical motion tenderness Adnexal tenderness Mucopurulent vaginal or cervical discharge Evaluation** Detailed history Abdominal and pelvic exam** Diagnostic tests** Cervical cultures for Gonorrhea and Chlamydia ○ Nucleic Acid Amplification Test (NAAT) – Urine, vaginal, or endocervical swab Wet prep to rule out concurrent infections (yeast, BV, or trichomoniasis) Pregnancy test UA +/- urine culture, CBC, ESR, CRP Consider pelvic ultrasound Screen for other STDs** (i.e. HIV, Syphilis) Hospitalization** Treatment** Fitz-Hugh-Curtis Syndrome** Infection spills into peritoneum and tracks superiorly through the hepato-colic gutter Inflammation of the hepatic capsule (perihepatitis) Symptoms Colicky, RUQ abdominal pain Vomiting LFTS typically normal RUQ US often normal…but can show inflammation of the capsule **Must be considered when evaluating sexually active adolescent with RUQ pain!! Other Complications** Tubo-ovarian abscess Recurrent infection Chronic abdominal/pelvic pain pain Ectopic pregnancy Seven-fold increase!! Infertility Risk increases with delayed diagnosis, younger age of infection, Chlamydial disease, and severe PID Patient Counseling Be abstinent for at least 1 week after treatment Contact sexual partners and encourage their treatment “Expedited partner treatment” – give an advance prescription to patients to assist with treating sexual contacts Future safe sex practices Thanks