Maryland's Mental Health Initiatives

Healthy Transitions Initiative:
An Effective Approach to Mental Health Services
Katie Herring, M.S.
Steven Reeder, M.Ed., CPRP, CRC
Kati Stein, Ph.D.
Sharon Stephan, Ph.D.
Acknowledgements
Maryland’s Healthy Transitions Initiative was funded by the US Department of Health and Human Services –
Substance Abuse and Mental Health Administration as part of the Emerging Adults Initiative (Grant Number SM-09-
008).
Characteristics of
Transition Age Youth with EBD
National Longitudinal Transition Study-2 (NLTS-2) found that the majority of youth with EBD:
• Male
• Living in poverty
• Head of household has no education past high school
• ADHD
• Disability is identified later (age 9 or after)
• 40% have attended five or more schools
• History of social adjustment problems
• Suspended or expelled at least once
Outcomes
• It is estimated that at any point in time, 13% of young adults ages 18-26 are experiencing some form of a mental health condition, and the majority of these individuals do not receive related services or supports.
• The results of the (NLTS-2) indicated that young adults who were identified as an EBD, and received special education services under the
Individuals with Disabilities Education Act (IDEA):
• Experienced a greater high school dropout rate, and lower post school employment (42% compared to 66%) than their non-disabled peers or peers with other disabilities (Wagner & Newman, 2012).
• Furthermore, young adults with serious mental health conditions may experience unemployment, substance abuse, incarceration, unnecessary disability, homelessness, and suicide at greater rates than the general population (Koerner, 2005).
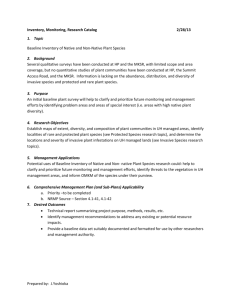
Comparison of Transition Domains Between the General
Population and Young People with Emotional/Behavioral Disorders
70%
63%
60% 58%
56%
50%
45%
General Population
40%
33% EBD
30%
25%
21%
20% 18%
11%
10% 8%
0%
Dropouts Employed Post-Sec.
Ind. Living Arrested
Challenges
•
Parents and youth themselves blamed for the disability
•
Stigma
•
Ignorance; disability identified late and treatment delayed
•
Presence of disability is not always obvious
•
Limited Family Involvement
•
Limited youth involvement and engagement
Barriers to Service Delivery
• Services through special education, the foster care system, and state child and adolescent mental health systems often end at the age of 18 or 21, and provisions for smooth transitions into adult mental health systems are rare;
• Adult services are often more fragmented than child mental health services; therefore, individuals may have to interact with several agencies to enroll in different programs to get the range of services they need;
• Eligibility criteria are typically much more restrictive in adult mental health systems as compared to child and adolescent mental health systems (Koroloff, Davis,
Johnsen, & Starrett, 2009; Koyanagi & Alfano, 2013).
The Emerging Adults Initiative
• The Emerging Adults Initiative (EAI) was a five year systems change project funded by the Substance
Abuse and Mental Health Services Administration
(SAMHSA). Seven states were awarded funding:
Georgia, Maine, Maryland, Missouri, Oklahoma,
Utah and Wisconsin.
• In Maryland this program is called the Healthy
Transitions Initiative (HTI)
• HTI is a state/community partnership aimed at addressing issues transition-age youth encounter as they transition to adulthood.
HTI in Maryland
• The Healthy Transitions Initiative (HTI) is a program designed to provide services that meet the distinct needs of transition-age youth (TAY) ages 16-
25 with emotional and behavioral disorders (EBD) in Frederick and Washington Counties.
• Evidence-Based Practice (EBP) Supported
Employment + EBP Assertive Community
Treatment + Transition to Independence Process
(TIP) + Peer/Family support
Description of HTI Population
• DSM-IV diagnosis indicates severity of need
– a psychotic disorder (i.e., schizophrenia, schizoaffective disorder);
– a major mood disorder (major depression, bipolar disorder); or
– a major anxiety disorder (generalized anxiety disorder, obsessive compulsive disorder, panic disorder, post-traumatic stress disorder, or social phobia) – most have multiple and complex diagnoses.
Description of HTI Population
• Functional Impairment
– A clear, current threat to the ability to live or be maintained in the
community.
– A significant inability to negotiate the developmental tasks of emerging adulthood and to assume normative adult roles, including but not limited to: exploring opportunities for employment, school, housing, and social relationships, and making life course decisions.
This significant inability, or dysfunction, is not solely defined as the failure to fully meet societal expectations of residential stability, stable employment, school completion, or establishment of a family.
– A significant inability to manage the symptoms of one’s illness or modulate one’s behavior in response to social cues or societal norms
(not manifested solely by criminal behavior).
Description of HTI Population
• Multiple psychiatric hospitalizations
• Residential Treatment Center placement
• Substance Abuse
• Aggressive Behavior
• Behaviors resulting in danger to self or others
• Psychosis
• Poor reality testing
• High levels of impulsivity, poor judgment, and/or inability to self protect in community situations
Goals of HTI
• Improve outcomes for TAY with serious mental health conditions in areas such as education, employment, housing, mental health and co-occurring disorders, and decrease contacts with the juvenile and criminal justice system;
• Foster youth self determination;
• Engage and support families;
• Enhance core competencies of behavioral health practitioners in developmentally appropriate and empirically supported practices to support the needs of Transition Age Youth;
• Link local implementation to state-level program and policy development to address broader system and financing issues;
• Disseminate and replicate to other geographic locations throughout the state.
How is HTI Different?
HTI services and supports are: Traditional services and supports are:
• Co-designed and selected by youth • Designed and determined by professionals
• Strengths-Based Disability-/ Deficit-Based
• Developmentally-Sensitive
• Non-Stigmatizing
• Culturally Competent
•
•
•
Adult-Focused OR Child-Focused
Unintentionally stigmatizing
Designed for the majority culture
• Appealing to youth
• Convenient for youth and families
• Focused on real life goals/dreams
• Facilitative of youth self-determination
• Delivered in mental health centers
• Focused on skills development
• Empirically-supported
•
•
•
•
•
•
•
Unpleasant or undesirable to youth\
Convenient for professionals
Focused on treatment goals
Custodial and protective of risk
Delivered in natural settings
Focused on service provision
Based on professional judgment/wisdom
HTI Evaluation Overview
• Quantitative
– National Outcomes Measures (NOMs)
– Individual Interviews – Youth and Caregiver
• Domains include background and demographics; living situation; education and job training; employment, career, and finances; parenting; social connectedness; selfdetermination; perceptions of opportunity; efficacy and empowerment; physical health; satisfaction; mental health and substance abuse; and criminal justice.
• Qualitative
– Six focus group interviews – two youth focus group interviews
(one in each county); two caregiver group interviews (one in each county); one staff group interview; one supervisor group interview.
Quantitative Data Collection
NOMs Collected
Assessment
Baseline
6-Month
12-Month
18-Month
24-Month
30-Month
36-Month
42-Month
Total
N
160
72
50
35
28
18
12
5
380
Interviews
Conducted
Assessment
Baseline
6-Month
12-Month
18-Month
24-Month
30-Month
36-Month
42-Month
Total
Youth
15
16
6
9
48
27
25
1
148
Caregiver
4
3
7
7
25
19
18
1
84
Total
22
23
10
12
73
46
43
2
232
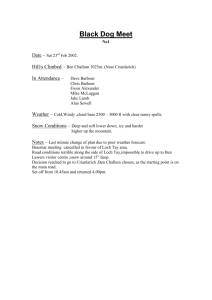
NOMs Analysis
Baseline Demographics
• 56.3% of HTI enrollees are male
• Average age at baseline was 19.4 years
30
25
20
15
10
5
0
50
45
40
35
16 17 18 19 20 21 22 23 24 25
Age
African American
17%
Other Multiracial
4%
Hispanic and
Caucasian
5%
Hispanic/Latino
3%
African American and Caucasian
6%
White/Caucasian
65%
Living Situation
• Baseline living situation
• 14.4% of youth were not retained in the community for the past 30 days
– 8 were homeless
– 6 were in inpatient mental health care*
– 6 were in a correctional facility*
– 1 was in an inpatient substance abuse facility
*1 youth reported being in both inpatient mental health care and in a correctional facility in the past 30 days.
Education and Employment
• TAY under age 18 at baseline
– 78% enrolled in school or job training
– 3% had completed high school
– 11% were employed part-time and 65% were looking for work
• TAY age 18 and over at baseline
– 41% enrolled in school or job training
– 19% were employed part-time, 9% were employed full-time, and 50% were looking for work
– 71% had completed high school or GED
– 11% had completed some college or university
Substance Use
• Baseline substance use in the past 30 days
Tobacco
Alcoholic beverages*
Cannabis
Cocaine
Prescription stimulants
Methamphetamine
Inhalants
Sedatives or sleeping pills
Hallucinogens
Street opioids
Prescription opioids
Other**
97.5%
9.0.%
96.3%
96.3%
92.5%
65.6%
Never Once or Twice Weekly Daily/Almost Daily
49.4% 6.3% 1.3% 40.6%
67.5%
80.0%
18.8%
8.8%
1.3%
2.5%
6.9%
5.0%
96.3%
93.8%
98.1%
1.3%
1.9%
0.0%
0.0%
0.0%
0.0%
0.6%
1.9%
0.0%
0.6%
2.5%
0.6%
0.6%
2.5%
0.6%
0.0%
0.6%
0.0%
0.0%
0.6%
0.0%
0.0%
5.0%
0.6%
0.6%
2.5%
1.3%
Missing/Refused
2.5%
5.6%
3.8%
1.9%
2.5%
1.9%
1.9%
1.9%
2.5%
2.5%
1.9%
32.5%
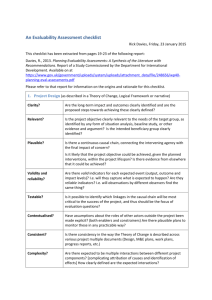
Psychological Distress
• Items asked “During the past 30 days, about how often did you feel... nervous, hopeless, restless or fidgety, so depressed that nothing could cheer you up, that everything was an effort, worthless?”
• At baseline, 73.1% of TAY reported serious psychological distress in the past
30 days.
– Mean scores on the psychological distress scale decreased significantly from baseline
(M=3.01) to the 12-month follow up (M=2.27).
2,5
2
1,5
1
0,5
0
4
3,5
3
3,03
3,35
2,19
Baseline 6-Month 12-Month
Perception of Functioning
• Example items: “I deal effectively with daily problems,” “I am able to control my life,” and, “My symptoms are not bothering me.”
• At baseline, 55% of TAY reported a positive perception of their functioning in everyday life.
– TAY were more likely to report positive perception of functioning at 6-month follow up compared with baseline.
– There was a significant increase in perception of functioning scores for youth with complete baseline through 18-month assessments.
Perception of Functioning Mean Scores (N=12)
3,89
3,51
3,72
4,29
5
4
3
2
1
0
Baseline 6-Month 12-Month 18-Month
Social Connectedness
• Example items: “I am happy with the friendships I have,” “I feel I belong in my community,” and, “In a crisis, I would have the support I need from family or friends.”
– At baseline, 71% of TAY reported the presence of social connections to family, friends, and the community.
– TAY were more likely to have a positive outcome on social connectedness at the 12-month and 18-month follow ups than at
6-months.
Perceptions of Care
• At the 6-month assessment, 92% of TAY reported positive overall perceptions of care.
Staff here believe I can grow, change and recover.
I felt free to complain.
I was given information about my rights.
Staff encouraged me to take responsibility for how I live my life.
Staff told me what side effects to watch out for.
Staff respected my wishes about who is and who is not to be given information about my treatment.
Staff were sensitive to my cultural background (race, religion, language, etc.)
Staff helped me obtain the information I needed so that
I could take charge of managing my illness.
I was encouraged to use consumer run programs
(support groups, drop-in centers, crisis phone line, etc.)
I felt comfortable asking questions about my treatment and medication.
I, not staff, decided my treatment goals.
I like the services I received here.
If I had other choices, I would still get services from this agency.
I would recommend this agency to a friend or family member.
40
64
64
64
61
62
63
63
63
N Minimum Maximum Mean
64
62
1
1
5
5
4.28
4.15
64
64
1
1
5 4.23
5 4.28
63
2
1
1
1
1
1
1
1
1
1
5
5
5
5
5
5
5
5
5
5
3.28
4.36
4.14
4.09
3.64
3.92
4.21
4.29
4.21
4.21
Local Evaluation Interviews
Goal
Perceptions of Opportunity
…to have a good job or career
…to graduate from college
…to earn a good living
…to provide a good home for your family
…to have a good marriage and/or long term committed relationship
Aspiration
(Importance)
Mean Score
2.90
2.71
2.96
2.92
2.54
Perception of
Opportunity
Mean Score
2.58
2.25
2.48
2.63
2.29
Significant
Difference?
Yes
Yes
Yes
Yes
Statistical Estimates t(47) = 3.92, p< .001
t(47) = 4.88, p< .001
t(47) = 4.86, p< .001
t(47) = 4.01, p< .001
Yes t(47) = 2.72, p= .009
…to have a good relationship with your parent or caregiver
…to have a good relationship with your significant other
…to have a good relationship with your children
…to have a good relationship with your friends
…to stay out of trouble with the law
…to stay clean (off drugs and/or alcohol)
Overall Index
2.67
2.94
2.85
2.78
2.75
2.65
2.75
2.58
2.75
2.73
2.55
2.52
2.52
2.77
No
Yes
No
Yes
Yes
No
No t(47) = 3.08, p= .003
t(47) = 1.35, p= .182
t(47) = -.375, p= .710
t(47) = 1.27, p= .209
t(47) = 2.44, p= .018
t(47) = 1.95, p= .057
t(47) = 5.94, p< .001
Self-Determination
• “Acting as a primary causal agent in one’s life and making choices and decisions regarding one’s quality of life free from undue external influence or interference” (Wehmeyer, 1996)
• At baseline, 51% of TAY reported that generally they “always” regulated their thoughts, feelings, and actions to work toward goals.
• 19% of caregivers reported that their youth “always” regulated their thoughts, feelings, and actions to work toward goals.
Youth
On average, always regulate self
On average, almost always regulate self
On average, sometimes regulate self
On average, almost never regulate self
On average, never regulate self
Frequency Percent
24
20
4
50.0
41.7
8.3
Total
0
0
0.0
0.0
48 100.0
Caregiver
On average, always regulate self
On average, almost always regulate self
On average, sometimes regulate self
On average, almost never regulate self
On average, never regulate self
Total
Frequency Percent
5
9
8
18.5
33.3
29.6
5
0
27
18.5
0.0
100.0
Efficacy and Empowerment
•
3 subscales
– At baseline, 86% of TAY reported that they were “mostly or always” able to self-manage their emotions and mental health
– 96% reported that they were “mostly or always” able to self-manage services and supports
– 77% reported that they were “mostly or always” able to improve or help change service systems
70
60
50
40
10
0
30
20
100
90
80
Youth and Caregiver Satisfaction
100,0
82,0
89,5
96,4
63,2
82,1 82,1
73,7
60,7
55,6
Youth
Caregiver
Qualitative Evaluation
Youth
Female
Male
Total
Caregivers
Female
Male
Total
Staff
Female
Male
Total
Overall Totals
4
0
4
2
4
6
2
1
3
13
Focus Groups
Frederick County Washington County Totals
4
0
4
2
3
5
2
1
3
12
8
0
8
4
7
11
4
2
6
25
Results
•
Services Provided
•
Strengths
•
Additional Needs
Services and Supports
• Transportation
• Dealing with agencies and services
• Assistance during IEP meetings
• Help with driver’s education
• Studying for and taking the GED
• Employment
• Housing
• Respite & emotional support
Strengths
• Availability and commitment of staff
• Flexibility
• Different from other service providers
• Self-directed funds
• Assistance navigating systems and other service providers
• Supports for caregivers
Additional Needs
• Housing
• Increased opportunities for employment
• Social interaction and more peer supports
• Additional supports for transition age youth with mild or moderate disabilities
• Smaller, more manageable case funds
• Increased assistance with Individualized Education
Program (IEP) meetings
Suggestions
• Additional group and social activities for youth
• Increased supports and information for caregivers
• Need for additional resources
• Increased assistance with employment & housing
• More manageable case loads
• Increased availability of housing
The Affordable Care Act
• Under the ACA provision, otherwise independent young adults can receive health care coverage through their parent’s plan up until the age of 26.
• Medicaid coverage is now available to children who have aged out of the foster care system but who are under age 26.
• Under Section 2703 of ACA, the Medicaid Health Home State Plan
Option states have the option to allow adult and child Medicaid beneficiaries with “at least two chronic conditions, one chronic condition and the risk of developing a second, or one serious and persistent mental health condition” to select a specific provider as their health home to help coordinate their treatments.
• Medicaid expansion allows individuals to be eligible for Medicaid at incomes up to 138% of the Federal Poverty Level (FPL).
Next Steps in Maryland
• In September 2014, Maryland was awarded a new five year
SAMHSA grant – Now is the Time: Healthy Transitions.
• This new program will be called Maryland Healthy
Transitions (MD-HT) and will serve TAY in Howard, Calvert,
Charles, and St. Mary’s Counties.
• MD-HT will build on the work of HTI by expanding access to individualized, strengths- and evidence-based supports for youth and young adults with mental health challenges.
• HTI services will be sustained in Frederick and Washington
Counties.
• The overarching goal of this work is to have best practices for serving TAY with mental health challenges adopted statewide.
Questions and Comments
Katie Herring
Kherring@psych.umaryland.edu
Kati Stein
Kstein@towson.edu
Steven Reeder
Steven.reeder@maryland.gov
Sharon Stephan
Sstephan@psych.umaryland.edu