Does prompt treatment of UTI in
preschool children prevent renal scarring?
Louisa Hemington
ST5 General Paediatrics
Oct 2015
Aim
• To determine whether prompt active management of
UTI’s by primary and secondary care providers can
reduce renal scarring rates.
Objective
• Assess validity and reliability of a relevant paper
• Ponder whether local practice needs to change
Paper
Does prompt treatment of urinary tract infection in
preschool children prevent renal scarring: mixed
retrospective and prospective audits.
Malcolm G Coulthard, Heather J Lambert, Susan J Vernon, Elizabeth W
Hunter, Michael J Keir, John N S Matthews
Arch Dis Child 2014;99:4 342-347
Current practice
• Management of UTIs is likely to be variable across
primary/secondary care despite NICE guidance
• Our local guideline states that
– Decision to treat with antibiotics is based on a combination of
clinical features together with a significant growth of bacteria in
the urine
• Most childen that present with temperature have a urine
sample
• In practice, UTIs are often ‘missed’ and patients called
back and treated several days or even weeks after initial
presentation
Methods 1
• Compared two cohorts
– 1990’s group (retrospective)
• All children <16y in Newcastle between 1992-1995
• With first diagnosis of UTI
• Imaged as per the 1991 recommendations
– 2000’s group (prospective)
• Audited the impact of a PCT adopted ‘direct access’ (DA)
service for UTI Mx which was implemented in Newcastle on a
cohort of children born after 1/1/04 with UTI
• Imaged as per 1991 recommendations (only difference
children >3.5y had MAG3 in place of MCUG)
• Didn’t follow NICE guideline until study complete
Methods 2
• ‘Direct Access’ service
– DA service nurse
– Encouraged GPs to start antibiotic treatment on clinical
suspicion of a UTI immediately after urine collected , and then
stop in culture negative cases rather than refer all cases to
hospital
– Urgent microscopy advocated
– Counsel parents of children with VUR to seek early medical
attention/urine microscopy
– Offer trimethoprim prophylaxis
– Imaged children as per 1991 guidelines
– If UTI recurrence occurs repeat DMSA scanning
Outcome measures
• 1990 group
– Focal DMSA defects consistent with scarring
– Time to treat
• 2000 group
–
–
–
–
Focal DMSA defects consistent with scarring
Attendance interval (Sx onset - GP attendance)
Prescription interval (attendance – prescription) in days
Total: Symptom – Prescription time ‘Time to treat’
Results
• Similar numbers of girls and boys referred with UTI in
1990 group and 2000 group
– girls 8.7% v 10.6%
– boys 3% v 3.1%
• Mean no of children
– 1990s – 9376/year group for 4 years
– 2000s – 4426/year group with decreasing FU
• Number imaged
– 1990s – 2262 imaged
– 2000s - 1664 imaged
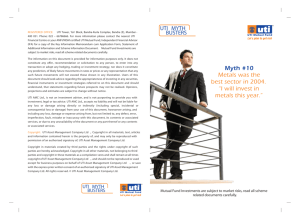
Malcolm G Coulthard et al. Arch Dis Child 2014;99:342-347
Copyright © BMJ Publishing Group Ltd & Royal College of Paediatrics and Child Health. All rights reserved.
Cumulative referral rates of girls and boys with a urinary tract infection (UTI) in Newcastle,
using a conventional UTI management model up to the age of 16 years during 1990s (open
circles), and using the direct access model up to the age of 8 years during the 2000s (filled
circles).
Children were
referred younger
in the DA access
group 2000s
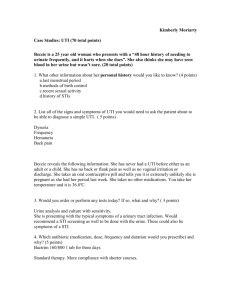
Malcolm G Coulthard et al. Arch Dis Child 2014;99:342-347
Copyright © BMJ Publishing Group Ltd & Royal College of Paediatrics and Child Health. All rights reserved.
Percentage rates for focal scarring (black bars) and isolated vesicoureteric reflux (grey bars)
among girls and boys in Newcastle after a urinary tract infection.
Girls
OR of having a scar
in DA group 0.47
(CI 0.29-0.76)
Less than half as
likely to sustain a
scar in the direct
access group
(2004-2012)
Boys
OR of having a scar
in DA group 0.35
(CI 0.16-0.81)
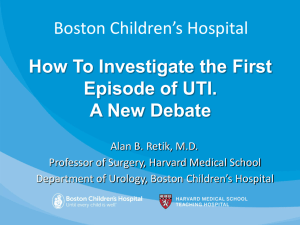
Malcolm G Coulthard et al. Arch Dis Child 2014;99:342-347
Copyright © BMJ Publishing Group Ltd & Royal College of Paediatrics and Child Health. All rights reserved.
Children treated within
3 days of their
symptoms starting had
less than half the
chance of being
scarred
OR 0.37 (CI 0.18-0.75)
Symptom - treatment
interval was longer for
patients with scars
OR 2.7 (CI 1.33-5.56)
Malcolm G Coulthard et al. Arch Dis Child 2014;99:342-347
Copyright © BMJ Publishing Group Ltd & Royal College of Paediatrics and Child Health. All rights reserved.
VUR
• More isolated VUR in 2000 group
– Age adjusted OR 11.9 (CI 4.3 - 33.5) girls
– OR 14.4 (CI 4.3 – 47.6) boys
• 1990s
– 3 infants with isolated VUR (no scarring)
• 2000s
– 103 children with isolated VUR
CASP checklists
• Are the results of the study valid?
– Dealt with a clearly focused issue – sought to prove that by treating UTI
early, scars can be prevented
– Clear outcomes defined of ‘renal scarring’ and ‘time to treat’
– 2 populations – one retrospective, one prospective
• 1990s: Population of of 154,000 <16y olds over 4yrs 1992-95 in
Newcastle & adjacent districts
• 2000s: Population of 70,800 born after 1/1/04 managed by GPs/walk in
centres/ED until 2012 (8 years)
– Populations covered different catchment areas of Newcastle
• Was the cohort recruited in an acceptable way?
• Yes
• Included all referred cases of UTI in the retrospective
and prospective group
• Difference in age of children between the groups
– 1990’s <16y
– 2000’s Only studied 1-8yr olds
• Was the exposure accurately measured to minimise
bias?
• Definition of UTI in both groups
– Pure growth ≥105/mL E coli, Proteus, Klebsiella, Pseudomonas
or Enterococcus spp.
• Urine collection
– 1990’s: no mention of how urine collected
– 2000’s: family friendly urine pads for babies and washed up
potties for toddlers
• How the authors identified all the important confounding
factors?
– Analysed boys and girls separately
– Only used ≤8yrs data from 1990 group for comparison
– But 2 groups not matched in time or place
• Have they taken account of all the confounding factors in
the design and/or analysis?
– In 2000s group they adjusted for the attendance interval
• Was the outcome accurately measured to minimise
bias?
• Yes
• Standardised DMSA scan
• Was the follow-up of subjects
– complete enough?
• Uncertain what proportion of referred patients in the 1990s
group were scanned
• 1664/2069 had an USS and DMSA scan in the DA group
– long enough?
In the 2000 group the follow-up length decreased as the study
progressed with the children presenting in 2004 having 8 years FU
but those presenting in 2011 only having 1 yr
• What are the results?
• Children with a first UTI in the 2000s compared to those in the
1990s,
– were referred younger,
– were half as likely to have a renal scar (girls OR 0.47, 95% CI 0.29
to 0.76; boys 0.35, 0.16 to 0.81),
– and were about 12 times more likely to have VUR without scarring
(girls 11.9, 4.3 to 33.5; boys 14.4, 4.3 to 47.6).
• Children treated within 3 days of their symptoms starting were
about 1/3 as likely to scar as those whose symptoms lasted
longer
– OR 0.33 (CI 0.12-0.72)
• How precise are the results?
• Reasonable confidence intervals
• Do you believe the results?
• Yes
• Can the results be applied to the local population?
• Comparable population to Sheffield
• Difficult to implement locally without resources for a
similar DA service
• Do the results of this study fit with other available?
• One study that concluded that prompt treatment makes
no difference only looked at children with pyelonephritis
and acute DMSA scan changes
• Lots of studies about prophylaxis – remain inconclusive
• What the implications of this study for practice?
• Does raise awareness/add weight to the need for
promptly treating UTIs
Summary & Conclusion
• Clinical bottom line
– Prompt treatment of UTI (within 3 days) in children has the
potential to more than halve the scarring rate
Thanks for listening!