Craniosynostosis: a case of Apert Syndrome
advertisement

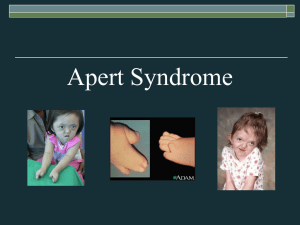
CRANIOSYNOSTOSIS: A CASE OF APERT SYNDROME Victoria Schunemann, MS4 THE CASE 6 yo Romanian female with: Apert syndrome ADD Speech delay PSurgHx R syndactyly release “Hip” surgery FamHx No Apert syndrome or non-syndromic craniosynostosis Physical Exam HEENT: turribrachycephaly; hypertelorism; proptosis; midface retrusion; relative prognathia Ext: previously repaired syndactyly on R, fused fingers on L; b/l fused toes Neuro: PERRL, EOMI, CN II-XII intact; moves all extremities equally with good strength THE CASE *NOT actual patient* THE CASE THE CASE Xray THE CASE Xray THE CASE CT THE CASE CT THE CASE CT THE CASE CT THE CASE CT APERT SYNDROME 1894 – Wheaton 1906 – Apert Triad Craniosynostosis Bilateral coronal sutures Midface hypoplasia Symmetric syndactyly hands AND feet Other findings Megalencephaly Hypoplasia of corpus callosum Aplasia of septum pellucidum Developmental delay Fusion of other joints Including cervical spine APERT SYNDROME Anomalies CNS Hydrocephalus Distorted ventricles Chiari malformations Orbits Proptosis Hypertelorism Strabismus Amblyopia Midface Impaired respiration Obstructive sleep apnea APERT SYNDROME Epidemiology 4.5% of cases of syndromic craniosynostoses Incidence 1 in 160,000 births Prevalence 1 in 55,000 births M~F Asian; Hispanic APERT SYNDROME Cranial development Matrix theory Base – endochondral ossification Calvaria – intramembranous ossification http://wps.aw.com/bc_marieb_happlace_7_oa/42/10965/2807221.cw/index.html APERT SYNDROME Genetics Autosomal dominant Majority de novo mutations 85% vs. 15% Risks Advanced paternal age FGFR2 2 missense mutations 755C->G, resulting in Ser252Trp 758C->G, resulting in Pro253Arg APERT SYNDROME FGFR Tyrosine kinase receptor Functions Embyronic development mesoderm induction antero-posterior patterning limb development ossification neural induction neural development Mature tissue angiogenesis keratinocyte organization wound healing processes https://www.qiagen.com/geneglobe/pathwayview.aspx?pathwayID=180 APERT SYNDROME Molecular Biology Gain of Function Increased affinity for ligands Loss of ligand binding specificity Epithelial – mesenchymal interaction TREATMENT Combined craniofacial case with plastics Monobloc with distraction and cranial vault remodeling TREATMENT Bicoronal sinusoidal incision TREATMENT Flap raised with exposure to orbits and zygomatic arches Pericranium dissected of f cranium for flap Bi-frontal craniotomy Recontouring of frontal bone with barrel staves and burring Dissection down to foramen cecum TREATMENT Gingival incisions Osteotomies – zygomatic arches, sphenoids, orbits, posterior nose, lateral pterygoid plates Free midface from cranium Disimpaction forceps to mobilize face TREATMENT Distractor placement and mobilization to 15 mm before returning to 3mm Frontal bone plated to supraorbital bar APERT SYNDROME Summary Triad Craniosynostosis of coronal sutures Bilateral syndactyly of fingers and toes Midface hypoplasia Mutations in FGFR2 Majority de novo Can be familial Gain of function Treatment Surgery at early age Can require continued surgeries Family support POST-OP THANKS TO… UCSD Neurosurgery Rady Children’s Hospital Dr. Meltzer Dr. Cohen WORKS CITED Agochukwu NB, Solomon BD, et al. Impact of genetics on the diagnosis and clinical management of syndromic craniosynostoses. Childs Nerv Syst. 2012 Sep;28(9);1447-63. Epub 2012 Aug 8. Bruce DA.Consensus: Craniofacial synostoseS: Apert and Crouzon syndromes. Child's Nerv Syst (1996) 12:734736. Carinci F, Pezzetti F, Locci P, et al. Apert and Crouzon syndromes: clinical findings, genes and extracellular matrix. J Craniofac Surg. 2005 May;16(3):361-8. Cunningham ML, Seto ML, et al. Syndromic craniosynostosis: from history to hydrogen bonds. Orthod Craniofacial Res 10, 2007; 67–81. Goodrich J. (2008). Craniofacial Syndromes, In B. Brandenburg & I Ip (Eds.), Principles and Practice of Pediatric Neurosurgery (289-309). New York: Theeme Medical Publishers, Inc. Ibrahimi OA, Chiu ES, et al. Understanding the molecular basis of Apert syndrome. Plast Reconstr Surg. 2005 Jan;115(1):264-70 Katzen JT, McCarthy JG. Syndromes involving craniosynostosis and midface hypoplasia. Otolaryngol Clin North Am. 2000 Dec;33(6):1257-84, vi. Kimonis V, Gold J, et al. Genetics of Craniosynostosis. Semin Pediatr Neurol 14:150-161. Morriss-Kay GM, Wilkie AOM. Growth of the normal skull vault and its alteration in craniosynostosis: insights from human genetics and experimental studies. J. Anat. (2005) 207, pp637–653.. Ocal E, Sun P, Persing J. (2008). Craniosynostosis, In B. Brandenburg & I Ip (Eds.), Principles and Practice of Pediatric Neurosurgery (265-288). New York: Theeme Medical Publishers, Inc. Rice DP (ed): Craniofacial Sutures, Development, Disease and Treatment. Front Oral Biol. Basel, Karger, 2008, vol 12, p 91-106