CasePres
advertisement

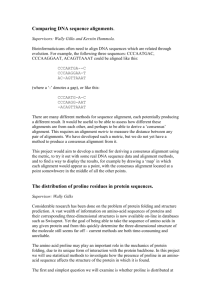
Richard C. Walls Patient Case Presentation PC: 51 yo black F; admitted 6/27/13 87.1 kg, 66” CC: Abdominal pain, ostomy leakage, hyperkalemia HPI: Hx ESRD(iHD), DM2, HTN, fungal/MDR-bacterial peritonitis requiring multiple operations leading to enterocutaneous fistula and TPN-dependence. Peritoneal dialysis -> Peritonitis (MDR citrobacter, bacteroides, enterococcus, candida) -> iHD Following resolution, developed surgical complications (bowel perforation) -> G-tube & wound vac. TPN-dependent due to frozen bowel. Plan for surgical takedown of EC fistula 09/2013. 2 wk PTA: clear liquid diet po -> full liquid -> 1 wk PTA leakage from ostomy bag, irritating abdomen (green/yellow drainage larger in volume than usual), only local pain, no N/V Reports pain at proline site, no redness/swelling/drainage (treated 2m PTA w/vanco, line not removed due to limited access). Afebrile, no chills/nightsweats. ED for management of ab pain/leakage, K+ found to be 6.7 w/peaked T-waves, leading to admission. Received calc gluconate, insulin, D50, 30g Kayexelate, and dialysis. PMH: ESRD iHD MDR peritonitis -> EC fistulas, bowel perf, frozen bowl; TPN DM2 w/neuropathy/nephropathy/foot ulcers Proline-associated cellulitis Chronic pancytopenia due to ESRD & infection HTN GERD PVOD (Pulmonary venoocclusive disease) F/SH: Father—HTN, brain cancer, DM2; Mother—Diverticulitis, arthritis; Sister—Deceased SLE 20 py smoker, no EtOH/illicits; lives with sons in flint, SNF in Saginaw recently Home Meds: Darbepoetin alfa 60 µsq weekly Insulin - Lantus: 10 Uam, 20 Uhs Insulin – Lispro: 2-12 UQID w/meal Gabapentin 300 po qd Fentanyl 75 µ/h q72 h Hydromorphone 2 po q4h prn pain Amlodipine 10 po qd Hydralazine 50 po TID Omeprazole/NaHCO3 20 po qd Folic Acid 1 po qd Allergies: Ciprofloxacin (reaction unsure) Protamine (reaction unsure) Morphine (itching) Clinical Course: 6/27 ED: K+ 6.6; proline site pain -> blood cultures; sysP(80s-90s) overnight 6/28 K+ 5.5 TPN resumed with reduced K+; Increasing proline site pain 6/29 K+ 4.6. Cultures grow GPCs; 1g vanco (11.4 mg/kg) cultures redrawn; pain worsening, refused TPN 6/30 Much improved symptoms, cultures -> coag negative staph; plan for 2 wks of vanco from first negative culture 7/1 Continued symptom resolution, post HD vanco – 9.0; redosed 1g; proline removed 7/2 Fevers overnight w/Stachy, recultured, Zosyn added 7/3 Isolated fever, Zosyn d/ced due to lack of culture growth/gram- suspicion, proline replaced, preHD level 25.5, post HD level 17.7, redosed 1g 7/4 Afebrile overnight, occasional tachycardia 7/5 Fever overnight w/tachycardia, preHD level 30.4, post HD level 22.5, patient cried because she had to stay another day due to large number of iatrogenic complications 7/6 Discharged to complete course of vancomycin Problem List: 1. Hyperkalemia 6.6 in ED w/peaked T-waves Managed with 1 g calcium gluconate, 10 U regular insulin, 25 g D50, & dialysis 5.5 -> 4.6 over 48 h Stable for rest of admission in high 3s, low 4s 2. Proline Associated Bacteremia Presented initially as pain and not treated, although cultures collected. 2 days into stay, patient exhibiting signs of sepsis (hypotension, tachycardia, thrombocytopenia), and blood cultures grow coag negative staph, 1g vanco 6/29. Symptoms improve, 7/1 vanco post HD 9.0, 1 g redose, proline removed. Pt becomes febrile, Zosyn (3.375 q12) added, d/ced next day due to no culture growth. HD levels 25.5/17.7 pre/postHD 7/3, redosed 1g Fevers begin again, patient shows preHD level 30.4, post HD 22.5, dose held Patient discharged to complete dialysis dosed vanco regimen until 7/13. 3. Fevers First present on 7/1 after vanco re-dose, resolve 7/2 afternoon. Isolated fever on 7/4, through 7/5 evening No culture growth apart from initial S. epi. despite sampling HD cath, proline. Leading suspicion is that vanco caused fevers, may want to consider linezolid/daptomycin based on situation for patient in future. 4. ESRD Hgb 10.2 on admit, fairly steady decline throughout admission down to 8.0 on 7/6 Some dilutional effect due to fluids (WBC 7.5 on admit, down to 2.9 on 7/6) MCV 86-92, RDW 16.4-18.0, 4/21—FRTN 972, TSAT 67.5, B12 401, Folate 2.7 Continue darbepoetin 60 qweek, f/u outpatient Phos 6.5-3.4, Ca++ ca 9.0, Alb ca 3.5 Continue paricalcitol 1 MWFw/HD, obtain iPTH outpatient & assess dose