Lesbian, Gay, Bisexual, and Transgender Ageing
advertisement

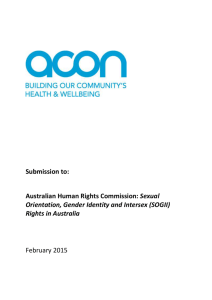
Community, Connection, and Well-Being: Promoting and Sustaining our Mental Health in Older Adulthood Daniel Parker PhD Clinical Psychologist email:danielparkerphd@aol.com This presentation: Suicide prevention in context of LGBTI older adult mental health and services LGBTI older adults & ageing services: Addressing increased risks & decreased service access Improving our community responses to longevity & ageing What can we do to minimise MH risks and increase positive ageing? A few key points: Depression and suicidality are not normal parts of ageing Higher levels of depression, anxiety and suicidal ideation among LGBTI adults, but Unclear picture for LGBTI older adults Aged care services, including mental health, may not be seen as welcoming of older LGBTI people Need a focus on inclusive services, outreach, and decreasing obstacles accessing mental health supports Standing Strong, Living Long: In a time of significant change Ageing and longevity: 14% of LGBTI Australians are 65 and older; by 2050, 23% of us will be 65 and older. “REDESIGNING LONG LIFE” Mental health focus on severe illnesses of later life is both necessary, and Mental health services for OA must be integrated, expanded and broadened LGBTI communities currently lack an ethos of ageing that is much better than the mainstream (Australian Government, 2010; ABS, 2010) (Stanford Center on Longevity) Social debate on ageing: How will it impact mental health? Is longevity a gift or a burden? How will care for those with dementia? Can we afford to live longer? How will our lives be structured as we age? What are the responsibilities of older adults? The Best Exotic Marigold Hotel, And What If We All Lived Together? We know there is a complex relationship between: Occurrence and presentation of older adult mental health disorders and Conditions of life for older adults, and Beliefs about ageing held generally & by older adults themselves, and Whether and how older adults use mental health services to address these Common issues LGBTI seniors share with all older adults: A focus on mental and physical health in ageing. Issues of continued workplace and community involvement, Making informed choices about retirement, health and volunteering; Defining new longevity and increased years in ways that feel rich and meaningful; Common issues LGBTI seniors share with all older adults: The impact of chronic diseases and illnesses of older adulthood, including dementia; Concerns about living situations and environments; Needs for interpersonal care and support, as well as institutional supports; Shared changes in the experience and structure of social relationships, including with friends and family; Needs to focus at times on issues of bereavement and end of life preparations. (IOM, 2011) Demographic Change 1: What we know about normal ageing, and the mental health of older adults (Carstensen, 2009) “Paradox of ageing”: Many emotional aspects of life improve as we get older Stress, worry, anger all decrease with age Fewer report psychological distress Even the very old report better emotional well-being than younger people Demographic Change 2: Living Longer with Chronic Health Conditions ABS 2007 data: Rates of MI decline for older adults but physical health comorbidities are high Many more will live with dementia Prediction: Living well with chronic conditions will increasingly be a focus in MH services LGBT older adults seem to have more chronic health conditions & disabilities HIV has made this a focus in LGBTI mental health for many years Demographic Change 3: “Social Capital” and Implications for Mental Health (Laidlaw & Pachana 2008) Family structures, patterns of partnership, marriage, childbearing and extended family structures are changing “Social capital” is seen to change, generally decrease for older adults Mental health in older adulthood heavily impacted by “social capital” issues Central to debates over the impact of ageing and caregiving Demographic change 4: “Retirement” and Work in Later Life Mark Freedman (2007): Current views of retirement are a recent and probably temporary response to increased longevity Is “retirement” socially and personally unsustainable? Rapidly changing beliefs about and plans for “retirement years” will be a major focus in psychotherapy and be intertwined with presentations for depression and anxiety. ABS 2007 National Survey of Mental Health & Well-being In 2007 did ask about sexual orientation Looked at lifetime and 12-month prevalence of a range of mental disorders and health conditions 12 month prevalences for those 16-85: Any MH Disorder 20.0% Anxiety Disorders 14.4% Affective Disorders 6.2% Substance Disorders 5.1% ABS 2007 National Survey of Mental Health & Well-being 12 month prevalence rates decline with age: For those 16-54: 25% (approximate) For those 55-64: 13.6% For those 65-74: 8.6% For those 75-84: 5.9% For older adults: More anxiety than affective disorders, and few substance issues Consistently more anxiety & affective disorders for women, substance use for men Suicide: LGBTI people and the broader population ABS (2007): .3% of men, .5% of women attempt suicide each year 65,000 non-fatal suicide attempts each year 11.9% of men, and 16.6% of women report suicidal thoughts over their lifetime 3 times as many men as women complete suicides Private Lives & LGBTI: 16% had SI within 2 weeks SPA: LGBTI completed suicides may be 3.5 to 14 times higher than mainstream And a variable picture for older adults experiencing depression and suicidal ideation… WA, 1986-2006: Decrease in rates of suicide among the elderly, possibly due to increased diagnosis, treatment 2009: Highest age-specific suicide death rate was among men 85+ Older adult mental health: Greater prevalence of depression and comorbid physical illnesses Increased lethality in suicide attempts Less warning or explicit clues, and increased lethality Less likely to access help and can’t assume will tell GPs LGBTI Older Adults: Likely risk factors… Within “LGBTI” our differing experiences Lifetime histories of suicidal ideation, self-harm behaviours and depression Possibly higher rates of substance use Impacts of stigma, exposure to violence Presumed increased social isolation due to being single, living alone, lesser supports from biological kin Possibly increased health issues, disability, lesser incomes Fears about aged care services LGBTI Older Adults: Possible protective factors? Resilience, “crisis competence” Possibly fewer gender differences, and lessened risks for G,B vs. heterosexual men Strong “family of choice” and community supports More varied but strong caregiver supports More experience using MH services, and in more varied ways “Prepared for ageing” by living as LGBTI LGBTI ageing as an emerging focus The stage of documenting and developing strategies to address significant health/mental health disparities GRAI National LGBTI Health Alliance Recent Developments in LGBTI ageing Aged Care Act—”Special needs group” & funding for cultural competency training MindOUT: Focus on mental health & suicide prevention Commonwealth National LGBTI Ageing and Aged Care Strategy Why look at issues facing LGBTI older adults? Legal and ethical responsibilities/duty of care issues LGBTI older adults now a “special needs” group under Aged Care Act Older adults a growing sector of LGBTI community, as in the broader population Can learn from the issues and solutions of LGBTI older adults Before the Therapeutic Alliance: How LGBTI elders approach older adult services Access to healthcare and providers with cultural competence major issues for LGBTI older adults Actual homophobia, transphobia and fears of encountering this Limited disclosure with health care providers Delay accessing services As the result of discrimination, possible increased health, mental health, substance use issues. Older Adult Services, Service Access and LGBTI Elders LGBT seniors report feeling lack of support from, and unwelcome in mainstream ageing programs. (SAGE, 2010) Few programs engage in outreach to LGBT seniors. Most unprepared to address discrimination by workers and other clients. (SAGE, 2010) The recent historical context for LGBTI mental health… Religion, law and mental health: Three structures defining life for LGBT people 1973: End of homosexuality as mental disorder in the DSM (later for ICD) Gender Identity Disorder and DSM-V Cohort differences: 1969 and Stonewall “The closet” to “don’t ask, don’t tell”. Impact of HIV/AIDS in the 80s and 90s. The impact of policies of exclusion on LGBTI mental health G. Rosenstreich: Discrimination, LGBTI mental health and suicide (2011) Fear and shame, social bullying, invisibility and “minority stress” Community responses of “Pride”, community, coming out, and identity Mental health outcomes: Increased stress, depression, suicidality, and anxiety What do we understand about mental health for LGBTI older adults? LGBTI people have different and higher rates of MH disorders across the lifespan It is unclear whether improvements in mental health with age occur for LGBTI older adults LGBTI people are active MH consumers Data for LGBTI people poorly integrated with broader OA MH literature Limitations to data about LGBTI elders Existing LGBTI health data fragmentary LGBTI studies include few older adults Differing ways of measuring sexual orientation: Sexual attraction, behaviour, and identity And with depression: Emotional state/mood, symptom cluster or clinical diagnosis? Considerable diversity among LGBTI people, and between age cohorts No MH intervention studies for LGBT seniors, or of services that exist. National Suicide Prevention Framework and Strategy are the only national policies to address LGBTI people (Carman et al. 2012) Recent Australian summaries of research: GRAI (GLBTI Retirement Association Incorporated) and Curtin Health Innovation Institute, Curtin University. (2010). Retirement accommodation and aged care issues for non-heterosexual populations: Literature Review. Perth, WA. Australian Research Centre in Sex, Health and Society (2008): Feeling queer and blue: A review of the literature on depression and related issues among gay, lesbian, bisexual and other homosexually active people. Melbourne, VIC. LGBT Older Adults: Recent US summaries Institute for Multigenerational Health (2011). The Aging and Health Report: Disparities and Resilience among Lesbian, Gay, Bisexual, and Transgender Older Adults. Seattle, Washington. Institute of Medicine (2011): The health of lesbian, gay, bisexual, and transgender people: Building a foundation for better understanding. MetLife (2010): Still out, still aging: the MetLife study of lesbian and gay baby boomers. SAGE and MAP (2010): Improving the lives of LGBT older adults. ABS 2007 National Survey of Mental Health & Well-being: Higher 12 month prevalence rates for LGB vs. Heterosexual respondents 45 40 35 30 25 Homosexual/Bisexual Heterosexual 20 15 10 5 0 Anx Affective SU Any MH Lifetime prevalence of mental health problems (Fenway Guide to LGBT Health, 2008) Higher levels of mood disorders, anxiety and suicidal ideation/behaviour (Ruble & Forstein, 2008) Higher rates of utilisation of mental health services by both lesbians (over last 12 months, 66% vs. 35.8%, and gay men (56.7% vs. 24.9%) Ruble & Forstein, 2008) Increased lifetime prevalence of suicidal ideation for G/L people, but not completed suicides Ruble & Forstein, 2008) For bisexuals levels of distress and mental health challenges at least as high as for lesbians and gay men: Higher rates of depression, suicidal ideation, and eating disorders When control for impacts of environmental and social stressors, some of differences may disappear Private Lives 2 (2012): Survey of 3835 LGBTI Australians 16-89 Older adults only 2.3% of sample, N=125 Those 65+ report good-to-excellent health more than other Australians While only suggestive, MH of LGBTI older adults appears to improve compared to those younger Private Lives 2 (2012): Factors Impacting Mental Health & Treatment Until 55, distress rates 2-3 times those of mainstream peers In the last 3 years, 30.5% diagnosed/treated for depression, 22.3% for anxiety Bisexual and trans men and women continue to have higher rates of MH issues than G & L peers 34.6% report occasionally or usually hiding their sexual orientation from care providers 31% said they had not told their GP their sexual orientation Significant numbers had experienced harassment or violence related to being LGBT in the last year: Verbal abuse Written threats or abuse Harassment (gestures, spitting) Threats of or actual assault 25.5% 6.6% 15.5% 8.7% US Institute of Medicine Summary: LGBTI Mental Health in Later Life (2011) “LGBT people in later adulthood typically are well-adjusted and mentally healthy.” Depression levels and suicidality appear to be elevated among older lesbians & gay men (less research on bisexual and transgender elders). For those with mental health issues, existing systems are often ignorant, neglectful or overtly discriminatory. Some evidence of crisis competence (resilience and perceived hardiness) within older LGBT populations, but more research is needed. The Aging and Health Report (2011) US federally funded, community-based study of 2500 LGBT older adults 71% rate overall mental health as “good” and 74% satisfied with lives Poor health, poverty and lower education associated with poorer mental health 30% reported clinical depression, 24% told had anxiety disorder, & almost 50% reported disability The Aging and Health Report: Concerning rates of health and mental health issues 53% reported loneliness 30% reported clinical depression 40% reported contemplating suicide at some point 24% had been told they have anxiety disorder 47% reported disability - 26% obese – 9% HIV+ Lesbians: 53% disabled – 34% obese Gay men: 41% disabled - 19% obese – 14% HIV+ Transgender older adults higher risk for disability, depression, suicidal ideation, & loneliness than non-T 62% disabled The Aging and Health Report: Wellness and Social Supports 91% engage regularly in wellness activities 82% do moderate physical exercise 38% attend spiritual or religious services or activities 90% feel good about belonging to their LGBT community Average level of social support = 3.1 (on a 4 pt. scale) ( 83% report someone w/whom to do something enjoyable) Assets and Liabilities: Looking at LGBT Older Adults’ “Social Capital” Expect to see the impact of unequal treatment under laws, programs, and in services We do know that LGBT people have differing, non-traditional patterns of care and support Older adult services may not evaluate this area accurately LGBT Care and Support Networks More likely to live alone, to be single or never partnered. Up to 42%, vs. 27% of general population. (MMI National Boomer sample). In some urban samples: Up to 65-75% lived alone. More likely to be poor, and with higher education earn less than peers. Mitigating factors: Social networks and supports LGBT elders generally not isolated and lonely. Many have children and grandchildren. “Logical kin”, “families of choice” and the role of friendships. 2/3 identify “chosen family”. (IOM, 2011) “Crisis competence” and doing for oneself. Community organising as a public health measure: “prevention and early intervention”. Political, community organisations and agencies: Significant majorities belong to at least one. Over 70% say “being LGBT helps prepare me for ageing” (MMI National Boomer sample) LGBTI caregiving: Using latent social capital LGBT Baby Boomers are active as caregivers (Met- Life, 2010) Reversal of gender expectations: Gay men a bit more so than lesbians “Halving it All”: Necessity dictates changes in roles more than ideology HIV epidemic: The emerging of caregiving groups out of friendship networks (Deutsch, 1999) Working with Older LGBTI Clients There is no evidence that anxiety, depression or suicidal ideation manifest differently in LGBTI clients, and one can work around these issues in standard ways. Summarising what we do know about LGBTI older adults and suicide prevention: Until proven otherwise, should assume higher risks for LGBTI older adults, and We should expect LGBTI older adults to be less likely to come forward and access generic services than age peers; and therefore Outreach to LGBTI elders needs to be targeted, clearly inclusive and repeated Sex differences in willingness to access services may be less pronounced MH services need to prepare now to work effectively with increased numbers of LGBTI older adults, and to ensure their comfort and safety within services (especially inpatient and residential services) Replicable/sustainable LGBTI-specific services? Looking at the GRC-SAGE program Specific focus on LGBTI older adults as “at risk” population, and on prevention/early intervention. Easy access: Could self-refer, low or no costs, in a non-clinical setting. Age-friendly: Center was both a venue for services, and a project developed and run by older adults Retirement, education, and work: Paid staff and older volunteers equally. Use of “secondcareer” psychology registrars. Effective MH models: CBT models used in LGBTI community settings with supervision Characteristics of GRC program: “Prevention and early intervention” of late life depression Clients were ambulatory, not housebound, with less severe health issues, and few had major cognitive impairments LGBT-specific services in community center with 900 members, and social, fitness, educational, food programs California Prevention and Early Intervention Initiative: Service Components: In-home MH services (PEARLS – Program to Encourage Active & Rewarding Lives for Seniors). Caregiver support groups and services. Elder Suicide Prevention outreach and services. Outpatient psychotherapy: CBT for Late- Life Depression ReStart Counselling Program: Use of evidenced-based therapy models PEARLS: Program to Encourage Active and Rewarding Lives for Seniors. Designed for home-bound clients. Minor, major depression, dysthymia. Solving problems contributing to depression (PST). Increasing social, physical and pleasant activities. CBT for Late-Life Depression Funds for training mental health staff in work with LGBTI elders using these models Mental Health Services offered in coordination with: Living a Healthy Life with Chronic Conditions: Peer-led Chronic Disease Self-Management Program. And with additional GRC support groups: Caregivers Bereavement Cancer Support Drug & Alcohol Recovery/ 12 Step Alzheimer’s & Parkinson’s Support Exercise, health, social activities. Building mental health and suicide prevention services for LGBTI Older Adults Evidenced-based services can be provided in non-traditional settings, and are tied to range of other wellness services. Because suicidal ideation is common and risks can be high, ties to LGBTI-inclusive higher level MH services are needed. While separate services are not essential, increasing LGBTI service access needs to be planned and proactive. Developing mental health services for LGBTI older adults… Suicide prevention must be addressed explicitly, and within a spectrum of MH services. A mental health focus on depression is far too narrow. Couples issues, issues around sexuality and relationship enhancement need more attention. Group therapy may be under-utilized, is popular, reinforces behavioural changes and allows for collectively addressing issues of meaning and community. A comprehensive and holistic mental health approach… Full inclusion in the benefits and responsibilities of ageing & longevity Build protective factors for older adults, and address those most isolated Counter the invisibility of older adults within our communities and become models for change Suicide prevention within a broad mental health fabric National LGBTI Health Alliance: Strategies for change Promote awareness, expertise and linkages in older adult/aged care sector: Train OA mental health services in LGBTI issues Build our own community supports and organisational capacity Influence policy and research, and integrate LGBTI data into existing MH and ageing data Having specific LGBTI mental health services can be important as part of an array of services What do we define as best practices for LGBTI older adult mental health and suicide prevention? Community awareness and services for those most at risk Levels of interventions, from prevention/early intervention to crisis intervention Have mainstream inclusive services, as well as LGBTI specific mental health services SP services visible and accessible to LGBTI older adults MH services in venues where older adults can and will access them, including in the home Minimise stigma around MH services, and integrate services with chronic disease management, wellness and healthy ageing programs. A few ways to address these issues now in our work: Follow developments in LGBTI aging DoHA National Ageing & Aged Care Strategy: Make comments, and use it as important guide Use GLHV’s or GRAI’s guidelines to make services inclusive REFERENCES: Barrett, C., Harrison J., & Kent, J. (2009). Permission to speak: Determining strategies toward the development of gay, lesbian, bisexual, transgender and intersex friendly aged care agencies in Victoria. www.matrixgulidvic.org.au Barrett, C., & Stephens, K. (2012). Beyond: “we treat everyone the same”. A report on the 2010-2011 program: How to create a gay, lesbian, bisexual, transgender and intersex inclusive service. Melbourne: gay and Lesbian Health Australia. Bradford, M., & Mayer, K. H. (2008). Demography and the LGBT Population: What we know, don’t know, and how the information helps to inform clinical practice. In H. J. Makadon, K. H. Mayer, J. Potter, & J. Goldhammer (Eds), The Fenway Guide to Lesbian, Gay, Bisexual, and Transgender Health. Philadelphia: American College of Physicians. Carstensen, L. L. (2009). A Long Bright Future: An Action Plan for a Lifetime of Happiness, Health and Financial Security. New York: Broadway Books. Ciechanowaki, P., Wagner, E., Schmaling, K., Schwartz, S., Williams, B., Diehr, P., Kulzer, J., Gray, S., Collier, C., LoGerfo, J. (2004). Community-integrated homebased depression treatment in older adults: a randomized controlled trial. Journal of the American Medical Association, Apr 7;291(13):1569-77. Corboz, J., Dowsett, G., Mitchell., A, Couch, M., Agius, P., and Pitts, M. (2008). Feeling Queer and Blue: A Review of the Literature on Depression and Related Issues among Gay, Lesbian, Bisexual and other Homosexually Active Peoiple. LaTrobe University: Australian Research Centre in Sex, Health and Society. De Vries, B. (2011, June). LGBT Ageing: Current Research Issues and Implications. Presentation and discussion at a community forum, Golden Rainbow Center SAGE, Palm Springs, CA Erikson, E. H., & Erikson, J. M. (1997). The Life Cycle Completed: Extended Version with New Chapters of the Ninth Stage of Development. New York: W.W. Norton and Co. Gallagher-Thompson, D., & Thompson, L. W., (2010). Treating Late-Life Depression; A Cognitive-Behavioral Therapy Approach. Therapist Guide. New York: Oxford University Press. Gardner A., & Mockus D. (2009). Out and Grey: Lesbian, Gay, Bisexual and Transgender Elders of Riverside County. Riverside County Office on Ageing. Riverside, CA. GRAI (GLBTI Retirement Association Incorporated). (2011). Best practice guidelines: Accommodating older gay, lesbian, bisexual, trans and intersex (GLBTI) people. www.grai.org.au Grant, J. M., Mottet, L. A. , Tanis, J., Harrison, J., Herman, J. L., & Keisling, M. (2011). Injustice at Every Turn: A Report of the National Transgender Discrimination Survey. Washington, DC: National Center for Transgender Equality & National Gay and Lesbian Task Force. Institute on Medicine. (2011). The health of lesbian, gay, bisexual, and transgender people: Building a foundation for better understanding. Washington, DC: The National Academies Press. Kimmel, D., Rose, T., & David, S. (Eds.) (2006). Lesbian, Gay, Bisexual, and Transgender Ageing: Research and Clinical Perspectives. New York: Columbia University Press. Laidlaw, K. (2010). Enhancing cognitive behavior therapy with older people using gerontological theories as vehicles for change. In N. A. Pachana, K. Laidlaw, and B. G. Knight (Eds.), Casebook of clinical geropsychology: International perspectives on practice (pp. 17-31). Oxford, U.K.: Oxford University Press. Laidlaw, K. & Pachana, N. (2009). Aging, mental health, and demographic change: Challenges for therapists. Professional Psychology: Research and Practice, 40, 601-608. Laslett, P., (1991). A Fresh Map of Life: The Emergence of the Third Age. Cambridge, MA: Harvard University Press. Leonard, W., Pitts, M., Mitchell, A., Lyons, A., Smith, A., Patel, S., Couch, M. & Barrett, A. (2012) Private Lives 2: The second national survey of the health and wellbeing of gay lesbian, bisexual and transgender (GLBT) Australians. Monograph Series Number 86. Melbourne: TheAustralian Research Centre in Sex, Health & Society, La Trobe University. MetLife. (2006). Out and ageing: The MetLife study of lesbian and gay baby boomers. Westport, CT: MetLife Mature Market Institute. MetLife. (2010). Still out, still ageing: The MetLife study of lesbian and gay baby boomers. Westport, CT: MetLife Mature Market Institute. Miller, M. D., (2009). Clinician’s Guide to Interpersonal Psychotherapy in Late Life. New York: Oxford University Press. PEARLS Program, Community-Based Depression Treatment. (Available from CHAMMP Training Institute, 325 9th Avenue, Box 359911Seattle, WA 98104) SAGE & Movement Advancement Project. (2010). Improving the Lives of LGBT Older Adults. http://www.lgbtmap.org/file/advancing-equality-for-lgbt-elders.pdf Thompson, L. W., Dick-Siskin, L., Coon, D. W., Powers, D. V., Gallagher-Thompson, D. (2010). Treating Late-Life Depression: A Cognitive Behavioral Therapy Approach. Workbook. New York: Oxford University Press.