Disruptive Behavior
Disorders
Creating an understanding for elementary
and middle school teachers by piecing
together the puzzle of
disruptive behavior disorders.
Amelia Weishaar
Learner Objectives
Participants in this seminar will be able to:
• Identify symptoms and characteristics of
disruptive behavior disorders (DBDs)
• Recognize the potential causes of DBDs
• Describe risk and protective
factors for DBDs.
Identification and
Characteristics of
Disruptive Behavior Disorders
“DBDs are the most common mental health disorder
among children with a rate of 4-9% of all children
from birth to 18 years old.”1
(Journal of the American Academy of Child &
Adolescent Psychiatry, Official Action, Jan 2007)
What is a Disruptive
Behavior Disorder?
The main category in the DSM-IV-TR that Disruptive Behavior
Disorders fall into is:
Attention-Deficit Disorder and Disruptive Behavior Disorders
Disruptive Behavior disorders are split into three more specific
diagnoses:
• Oppositional Defiant Disorder
• Conduct Disorder
• Disruptive Behavior Disorder (NOS)
Oppositional Defiant Disorder
(ODD)
2
DSM-IV-TR Definition
“A pattern of negativistic, hostile, disobedient and defiant
behaviors. Children display four or more of these
behaviors for more than 6 months
•
•
•
•
•
•
•
•
Loses Temper Easily
Argues with Adults
Actively Defies Adults Requests or Rules
Deliberately Tries to Annoy Others
Blame others for their own misbehavior and mistakes
Seems touchy or is annoyed easily
Angry and resentful
Spiteful or Vindictive”
Oppositional Defiant Disorder
• Average age of onset is 6 years old, symptoms can be seen in
children as early as 3 years old3
• Symptoms usually manifests by 8 years old, with most
children diagnosed during preadolesence1
• Children with ODD have a significantly higher rate of
having more that one psychiatric disorder4
• Most children, 67%, will ultimately exit from the diagnosis
after a 3-year follow-up5
• Early onset of ODD is more likely to
persist and lead to subsequent
development of CD6
Conduct Disorder (CD)
1
DSM-IV-TR Definition
“Repetitive and persistent pattern of behaviors in
which the basic rights of others or rules of society
are violated. Three or more of the following
behavior will have occurred within the last 12
months.
• Aggression Toward People and Animals
• Destruction of Property
• Deceitfulness or Theft
• Serious Violation of the Rules”
Conduct Disorder
Childhood-onset vs. Adolesent-onset7
Childhood-onset –
- Average age is 9 years old
- Males more likely to be affected
- Prognosis is poor as the earlier the age of CD syptom
onset, the more severe the disorder is likely to be
Adolescent-onset –
- Usually less severe
- Tends to coincide with family or peer problems.
- Aggression may or may not be present.
- Males = females for prevalence rates.
- Adolescent-onset of CD has a much
better progonsis
Disruptive Behavior Disorder
Not Otherwise Specified
1
(DBD NOS), DSM-IV Definition
This category of DBD was created for children who
demonstrate similar behaviors as children with
ODD or CD but do not display the same
frequency /severity and only met one or two of the
behavior criteria for this disorder.
Like ODD and CD, this disorder causes significant
impairment in the child’s life.
How many children are
diagnosed with DBDs?
• A summary of 34 studies suggested the prevelance
rate for children 4 – 18 years old is:8
ODD – range 3% to 22.5% with median of 3.2%
CD – range 0% to 11.9% with a median of 2.0%
• Another study indicated that ODD has a wide
range of prevelance from 1% -16% of children,
depending on which criteria and assessment
methods are used9
• Research presents evidence that
the prevelence and the severity
of this disorder are increasing10
Overlapping of disorders
It is rare for ODD/CD to occur outside the context of
other psychiatric disorders11
- Most common is ADHD
65% of children diagnosed with ADHD also had ODD
80% of children diagnosed with ODD also had ADHD
- Anxiety disorders
45% of children diagnosed with an anxiety disorder also had ODD
- Severe depression
70% of children diagnosed with severe depression also had ODD
- Bipolar
85% of children diagnosed with bipolar disorder also had ODD
- Language processing disorder (LPD)
55% of children diagnosed with LPD also have ODD
What causes
Disruptive Behavior Disorders?
• It is thought that children with severe behavior
disorders may be more influenced by neurological
and genetic factors12
• However mild to moderate DBDs are believed to
appear in children who have an accumulation of a
high number of risk factors and a low number of
protective factors in all contexts of their lives7
• This imbalance of risk to protective factors may
determines the presence and severity of
a child’s DBD. 5 6 7
Risk Factors
A risk factor is
a characteristic within the
individual
or a circumstance of the
individual
that increases the probability of a
Disruptive Behavior Disorder.
Biological Risk Factors
• Difficult Temperament at birth – irritable, easily
frustrated, angry and hard to soothe13
• Aggression is highly influenced by genetic factors in
boys and girls.12
• In severe cases of DBDs neurological factors may
cause the brain to function differently compared to
how an average child’s brain may function.12
• Children diagnosed with both ODD/CD and
ADHD (ADHD being highly genetic)
are likely to have greater symptom
severity and increased risk of future
disorders11
Individual Risk Factors
• Underdeveloped emotional regulation skills
• Low tolerance of frustration
• Little to no problem solving capabilities
• Inability to adapt to new situations
• Language development impairment11
Family Risk Factors
• Young age of the mother at birth of first
child
• Insecure Parental Attachment
• Coercive parent – child interactions
Parental behaviors include inconsistent/harsh discipline, poor monitoring/
supervision, low levels of warmth/nurturance, high numbers of negative
verbalizations towards the child.
• Depressed or “distressed” mother
• High levels of substance abuse and
antisocial behaviors in parents7 14
Contextual Risk Factors
• Living in urban, low-socioeconomic
settings.
As the magnitude of poverty increases, so too does the severity of
aggression and conduct problems7
• Living in a disadvantaged neighborhood
Characterized by dilapidated housing, high crime rates, isolation,
lack of economic resources and unsafe conditions.15
• Witness of violence or being the
victim of violence or abuse7
• Stressful live events16
School Risk Factors
• Zero-tolerance discipline which is highly punitive
and erratic, escalating with little or no attention to
students’ good behaviors or efforts to achieve10 17
• Negative interactions with adults, typical school
experience for these students is highly negative10
• Discipline including punishments that takes
students away from the academic environment17
• Deficits in social skills lead to rejection by
prosocial peers7
• Affiliation with “deviant” peers7 10
Non – Factors
• No significant evidence has been found that
demonstrates increased occurrence of DBDs
in relation to race and ethnicity 7 18 19
• Although controversial, most researchers
have concluded that there are no IQ
differences between children with and
without CD.7 19
Protective Factors
Protective factors reduce the
likelihood of children
confronted with risk factors
to develop maladaptive
behaviors associated with
Disruptive Behavior
Disorders.
Resilience in Childhood
Resilience, a positive adjustment occurring in
children at-risk, seems to result from a
combination of internal and external
resources that function as protective factors.7
Child Protective Factors
• Easy Temperament
• Good intellectual functioning
• Self-confidence
• Empathy
• Talents3 7
Family Protective Factors
• Good supportive relationship with a
parent
• Close supervision by parents when not in
school
• Positive parent-child relationships:
warmth, structure, high expectations
• Connection to extended supportive family
networks 5 7 8
School Protective Factors
• Children with ODD/CD who had a
positive teacher-child relationship showed a
decrease in aggression.20
• Friendship with prosocial peers7
• Bonds to prosocial adults outside the
family7 17
• Attending effective school3
Interventions
Interventions will be more
successful if they not only reduce
the risk factors, but also promote
the protective factors observed in
resilient children.7
School-wide Interventions
• Create a positive school climate
• Define behavioral expectations
- Small set of general expectations and specific expectations for
different locations in the school
• Support positive behavior
- Monitor behavior especially during common problem times,
acknowledge and reward positive behavior, use reminders and review
of behavior expectations.
• Respond to problem behavior consistently
and effectively
- Use consistent procedures in responding to minor and
serious problem behaviors. Institute procedures for
problems solving meetings.
Classroom Interventions
• Establish and teach the classroom rules and
procedures
- Classroom rules and procedures need to be established and clearly stated,
explicitly taught, closely monitored and consistently followed.
• Manage common problem times: transition, seat
work, other unstructured times of the day
• Promote social and emotional functioning
• Use rewards effectively
• Use mild punishment effectively
• Manage angry/acting out behavior
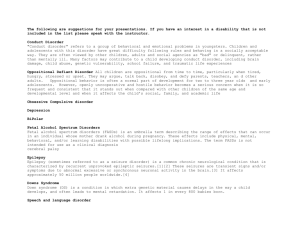
Three-level: Triangle Approach
School-Based Interventions
Green-Zone
Positive behavior
support interventions
that are school-wide
will support all
children. This
foundational level is
sufficient for
promoting positive
behavior for
approximately 80%
of students
Red-Zone
Comprehensive and
individualized interventions that
focuses on 5% of children with
significant difficulties
Yellow-Zone
Early interventions for children at
risk, will affect 15% of children
Individual Interventions
• Consistently reinforce good behavior
• Use of proactive and instructive teaching
strategies to teach adaptive behaviors and
problem solve with the student
• Train student to self-monitor disruptive
behaviors
• Use positive reinforcement when
students reaches behavior goals.
IDEA Classification
Special Education Interventions
• If a student with DBDs is labeled “emotionally
disturbed” they are included under and given all
protections under the Individuals with Disabilities
Education Act (IDEA)
• But, if a student with DBDs is labeled “socially
maladjusted but not emotionally disturbed”,
they are denied any protection under
IDEA and special education services10
Piecing it all together:
What does all of this mean for a
teacher?
Parent Involvement
• Home-school collaboration has the potential
to significantly increase academic success for
students with DBDs
• Teacher and parent use a “partnership
approach” to child’s success in school
• Send daily report card home
about the student’s behavior
• Encourage positive parental
reinforcement of specific
desired behaviors
What teachers should avoid
• Use of only reactive behavioral strategies
• Model antisocial behaviors by yelling or
insulting student, instead teachers should
model prosocial or problem solving
behaviors.
• Use of harsh punishment
• Only coercive interactions
with student
What teachers should do
• Understand that teaching children with DBDs may
take a “superhuman tolerance for interpersonal
nastiness” 10
• Directly teach adaptive behavior strategies
• Model and teach prosocial skills, problem solving,
empathy and self-control
• Use individual interventions for
students with DBDs
• Understand the teacher-student
conflict cycle and how to avoid it
The Conflict Cycle
Retrieved from:
http://cecp.air.org/interact/authoronline/april98/3.htm
Questions?
Glossary
• DSM IV - DSM-IV (Diagnostic and Statistical Manual of Mental
Disorders, Fourth Edition)
An official manual of mental health problems developed by the
American Psychiatric Association. Psychiatrists, psychologists, social
workers, and other health and mental health care providers use this
reference book to understand and diagnose mental health problems.
Insurance companies and health care providers also use the terms and
explanations in this book when discussing mental health problems. (site
is the
• Prosocial behavior -The term prosocial behavior describes acts that
demonstrate a sense of empathy, caring, and ethics, including sharing,
cooperating, helping others, generosity, praising, complying, telling the
truth, defending others, supporting others with warmth and affection,
nurturing and guiding.
• Antisocial behavior – The term anitsocial behavior describes behaviors
that are unacceptable in our society. Examples are acts of aggression or
malice, over-reactive displays of anger, inability to work or get along with
others, disrespectful towards others, and abusive towards others.
References
1. AACAP Official Action, (2007). Practice parameters for the assessment and
treatment of children and adolescents with oppositional defiant disorder.
Journal of the American Academy of Child & Adolescent Psychiatry, 46(1), 126-141.
2. American Psychiatric Association. (2000). Diagnostic and statistical manual of
mental disorders. (4th text revision ed.). Washington DC: Author.
3. Quay, H.C., & Hogan, A.E. (1999). Handbook of disruptive behavior disorders.
New York: Kluwer Academic/Plenun Publishers.
4. Angold, A., Costello, E.J. & Erkanli, A. (1999). Co-morbidity. Journal of Child
Psychological Psychiatry, 40: 1205 – 1212.
5. Lahey, B.B., & Loeber, R. (1994). Framework for a developmental model of
oppositional defiant disorder and conduct disorder. In D.K. Routh (Ed.),
Disruptive behaviors disorders in childhood. New York: Plenum.
6. Burke JD, Loeber R, & Birmaher, B. (2002) Oppositional defiant and conduct
disorder: A review of the past 10 years, part II. American Academy of Child
Adolescent Psychiatry, 41:11, 1275 – 1293.
7. Bloomquist, M.L. & Schnell, S.V. (2002). Helping children with aggression and
conduct problems: Best practices for intervention. New York: Guilford Press.
8. Lahey, B.B., Miller T.L., Gordon, R.A. and Riley, A.W. (1999). Developmental
epidemiology of the disruptive behavior disorders. In H. C. Quay & A. E.
Hogan (Eds.), Handbook of disruptive behavior disorder (pp. 23 – 48). New
York: Kluwer Academic/Plenum Press.
References
9. Loeber, R, Burke JD, Lahey BB, Winters A, Zera M. (2000) Oppositional
defiant and conduct disorder: a review of the past 10 years, part I. American
Academy of Child Adolescent Psychiatry, 39, 1468 -1484.
10. Kaufman, J. M. (2005) Characteristics of emotional and behavioral disorders
of children and youth. New Jersey: Pearson Prentice Hall.
11. Greene, R.W., Ablon, J.S., Goring, J.C., Fazio, V., & Morse, L.R. (2004).
Treatment of oppositional defiant disorder is children and adolescents. In
P.M. Barrett & T.H. Ollendick (Eds.), Handbook of interventions that work
with children and adolescents: Prevention and treatment (pp. 369 – 393).
New Jersey: John Wiley & Sons.
12. Pliszka, S.R. (1999). The psychobiology of oppositional defiant disorder and
conduct disorder. In H. C. Quay & A. E. Hogan (Eds.), Handbook of
disruptive behavior disorder (pp. 371 – 396). New York: Kluwer
Academic/Plenum Press.
13. Sanson, A. & Prior, M. (1999). Temperment and behavioral precursors to
oppositional defiant disorder and conduct disorder. In H. C. Quay & A. E.
Hogan (Eds.), Handbook of disruptive behavior disorder (pp. 397 – 417). New
York: Kluwer Academic/Plenum Press.
14. Loeber, R., Wung, P., Keenan, K., Giroux, B. , Stouhamer-Loeber, M.
VanKammern W.B., & Maughan, B. (1993). Developmental pathways in
disruptive child behavior. Development and Psychopathology, 5, 101 – 131.
References
15. Kupersmidt, J.B., Griesler, P.C., DeRosier, M.E., Patterson, C.J., & Davis, P.W.
(1995). Childhood aggression and peer relations in context of family and
neighborhood factors. Child Development, 66, 360 – 375.
16. Attar, B.K., Guerra, N.G., & Tolan, P.H. (1994) Neighborhood disadvantage,
stressful life events, and adjustment in urban elementary-school children.
Journal of Clinical Child Psychology, 23, 391 - 400.
17. Walker, H.M., Colvin, G., Ramsey, E. (1995). Antisocial behavior in school:
Strategies and best practices. California: Brooks/Cole Publishing Company.
18. Patterson, C.J., Kupersmidt, J.B., & Vaden, N.A. (1990). Income level, gender,
ethnicity and household composition as predictors of children’s school based
competence. Child Development, 61, 485 – 494.
19. Bolger, K.E., Patterson, C.J., Thompson, W.W., Kupersmidt, .B. (1995).
Psychosocial adjustment among children experiencing persistent and
intermittent family economic hardship. Child Development, 66, 1107 – 1129.
20. Hughes, J.N., Cavell, T. A., & Jackson, T. (1999). Influence of the teacherstudent relationship on childhood conduct problems: A prospective study.
Journal of Clinical Child Psychology, 28, 173 -184.
21. National Resource Center on AD/HD, (2005). What we know, 5b, AD/HD
and coexisting conditions: Disruptive behavior disorders. Maryland: Children
and Adults with Attention-Deficit/Hyperactivity Disorder (CHADD).
22. Honig, A. & Wittmer, D.S. (1996). Helping children become more prosocial:
Ideas for classrooms, families, schools, and communities. Young Children, 51,
(pp. 62-70).