Differential Diagnosis
advertisement

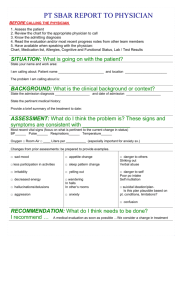
Documentation The other cornerstone of Western medicine Initial thoughts. . . Documentation is essential to providing skilled medical care. . . Serves a variety of purposes: Provides written record of presentation, evaluation, and treatment – to be reviewed by oneself or by consultants Allows for formal chart review of appropriate care and documentation – “peer review” Provides written proof of patient consent, medication instructions, etc. Directs support staff in the care of the patient Peer Review A formal evaluation of a certain percentage of a physician’s work Performed on a regular basis at almost all U.S. medical institutions A physician’s peers review outpatient and inpatient records for clarity, accuracy, appropriate documentation, and provision of standard of care medicine. So, what exactly do physicians document? Patient care related documentation The “Notes” Admission and Discharge The “Orders” Legal Documentation and Consent Administrative Documentation Routine admission, disposition forms Birth and Death certificates Insurance or billing paperwork The Notes An abbreviated notation of the facts – similar to the “notes” one might take during a lecture and refer to while studying before a test Allows colleagues and other medical personnel a chance to review the case Allows oneself a chance to review initial presentation and evaluation In later review of the chart one often finds subtle areas previously left unexplored The Notes In addition to recording Subjective and Objective portions of the patient presentation, documentation allows the physician to convey his or her own thoughts on the case – this is done in the Assessment portion of the note Next, the physician documents their Plan for further diagnostic study and/or treatment The Notes Careful attention is paid to internal consistency It is not necessary to explain every single laboratory test or treatment modality in detail It is necessary to provide ample facts such that any competent physician would be able to easily deduce your reasoning Finally, the fact that you discussed your thinking, the plan, and the expected outcome with your patient is documented Ms. Fukai, a 23 y/o o/w healthy Japanese ♀, presented today for ℅ acute onset R ear pain following daily swimming in the local pool over the previous week. Pt. has exp’d 36 hrs ↑’ing R otalgia assoc. w/ ↑’ing mucoid d/c. Afebrile and w/o any signs or symptoms of illness. Denies trauma/diving. Meds: Eucerin, occasional topical hydrocortisone 2% ointment Allergy: NKDA PMH/PSH/FH: Atopic dermatitis well controlled on current tx. o/w N/C Soc Hx: No tobacco, occasional EtOH (<2 drinks per week) VS’s: GEN: HEENT: LUNGS: CV: SKIN: Dx: T=37°C, P=68, RR=12, BP=120/64 Alert, NAD PERRLA/EOMI – B Nares patent/NL turbinates, L TM Θ with + movement to insufflation, R TM partially visualized and mobile to insufflation with + mucoid otorrhea in canal, + pain on manipulation of right pinnae, neck supple/Θ lymphadenopathy CTAB RRR without M/R/G NL S1/S2 Warm, moist – Ø evidence of atopic Δ’s Otitis Externa 2° to excessive H2O exposure Plan: Ofloxacin otic – 6-8 drops AD TID X 7 days Avoid H2O exposure throughout duration of tx RTC if discharge/pain ↑’s, swelling of neck/face, no response to tx Discussed etiology, pathophysiology, medication use, f/u Patient expresses understanding and concurrence Andrew W. Schiemel, MD, FAAP Shorthand from previous slide y/o o/w ♀ ℅ R exp’d hrs ↑’ing assoc w/ d/c w/o NKDA tx N/C EtOH NAD PERRLA EOMI = = = = = = = = = = = = = = = = = = = years old otherwise female complaint of right experienced hours increasing associated with discharge without no known drug allergies treatment non-contributory alcohol no acute distress pupils equal round and reactive to light and acc. extra ocular movement intact Shorthand continued B L TM Θ + CTAB RRR M/R/G NL S1/S2 Ø Δ’s Dx 2° H2O AD TID X RTC ↑’s f/u = = = = = = = = = = = = = = = = = = = = = bilateral left tympanic membrane negative positive clear to auscultation bilaterally regular rate and rhythm murmur, rub, gallop normal first and second heart sounds no (none) changes diagnosis secondary water aure dextra (right ear) three times per day for (X 7 days = for seven days) return to clinic increases follow up Review of sample note Clearly explains the patient’s presentation and makes reference to the patient’s overall health/medication use, etc. Pertinent positive and negative historical and physical facts are included. Although sufficient information to rule-out every known cause of otorrhea is not included, one can adequately discern between the two main diagnostic possibilities (otitis externa or ruptured tympanic membrane) with the information provided. Review of sample note Working diagnosis and treatment plan are clearly and succinctly laid out Exact medication directions are recorded, including dose, route, frequency, and duration of therapy. Indications for returning to the clinic are addressed and the physician notes that the patient expresses understanding and acceptance of the plan. Finally, the chart entry is signed and dated – with the physician’s printed name provided for accuracy. Admission and Discharge Admission H&P’s and discharge summaries are perhaps the most tedious of all medical documentation. Standard pre-printed forms for each are in common use so that important details are not overlooked. The assessment portion affords the physician the opportunity to express the logic effecting specific decisions. Admission and Discharge The assessment is often written as a narrative. The physician may report competing diagnoses, concerns regarding reliability of diagnostic testing or treatment side effects, anticipated outcome, etc. The plan portion of the admission paperwork typically lays out a variety of diagnostic and treatment actions. Essentially, it is a list of tasks to be accomplished during the admission. One should include “indications for discharge” in every admission plan. Admission and Discharge The discharge summary is simply a wellorganized running dialogue that delineates the patient’s presentation, hospital stay, and condition on discharge First, details regarding the initial presentation are summarized Strict delineation of subjective opinions from objective facts is often overlooked Instead, the key here is to summarize the basics of the presentation so that anyone reading the discharge summary understands how you arrived at your admitting diagnosis Admission and Discharge Secondly, the physician outlines the patient’s hospital stay, remarking on general trends observed from day to day – hopefully ending in resolution of disease or significant improvement. If, for example, the patient was steadily weaned from supplemental oxygen, there is no reason to list out a variety of pulse oximetry readings and subsequent changes to oxygen delivery. Admission and Discharge Instead the physician simply states: “Throughout the admission, supplemental oxygen initially supplied at 10LPM via non-rebreather face mask - was weaned entirely. At discharge the patient was consistently saturating >98% via pulse oximetry on room air alone.” The Orders Physician orders are written instructions for patient care. Historically the physician’s orders were written using medical shorthand in an effort to save time. Recently, however, there has been a push to revise this system and allow for minimal abbreviation use due to concerns regarding medication and treatment errors. The Orders Inpatient charting involves two varieties of medical orders – admission or transfer orders and daily orders. In an effort to remember all the specifics of admission orders, students and junior staff alike use the acronym, ADCVAANDIMLS pronounced “A-D-C van Dim-els” The Orders Admit to – Physician notes the specific location within the hospital where the patient should be admitted Diagnosis – The working diagnosis or diagnosis to be excluded Condition – One word reference to the patient’s general condition – e.g. Good/stable/guarded or poor/fair/critical Vital signs – Frequency of vital signs is listed - to include mention of any continuous monitoring such as cardiorespiratory monitor (CRM) – standard orders involve “q shift” or “every shift” vital signs – indicating that they are to be taken at change of the nursing shift Allergies – Patient medication allergies are listed (if none, no known drug allergies (NKDA) is listed The Orders Activity – Allowable patient activity is listed here (e.g. bed rest, bed rest with bathroom privileges, normal activity, limited activity, etc.) Nursing – Any specific nursing instructions (e.g. change patient position every 4 hours to avoid bed sores, sponge bath every morning, record fluid intake and output (strict I/O’s), indications to call on-duty physician such as “call medical officer for temperature greater than 39.5 degrees,” etc.) Diet – Allowable diet for patient (e.g. nothing by mouth (NPO), clear liquids (no solids), full liquids, soft diet, soft mechanical, regular, American Dietary Association 2000 calorie diet (ADA 2000), low-sodium, low protein, lactose restricted, etc.) The Orders IV fluids – Standard orders for intravenous (IV) fluids are listed here; although every admission does not involve IV fluid administration, this section allows for a dedicated space to indicate such therapy. Attention should be paid to details regarding the fluid composition, the volume to be given and the rate at which the fluids are to be run. Medications – Standing medication orders – that is, medication to be taken on a recurring basis throughout the admission; be sure to mention dosage, frequency, route, and indication where appropriate (e.g. acetaminophen 500 milligrams by mouth every 8 hours as needed for fever) The Orders Labs – This includes laboratory or radiological studies to be ordered at the time of admission and/or any recurrent lab/rad orders (e.g. 1. Acute abdominal series at admission, 2. CBC with differential count every morning, etc.) Special – Any orders that are non-medical in nature (e.g. patient may have off-ward privileges during the day. Or perhaps, patient does not want any visitors) The Orders • Transfer orders follow this same format, however the orders begin with “Transfer to ______” instead of “Admit to _____.” As the patient is being sent to an entirely different section of the hospital, all orders must be re-written. Simply writing a one-line order for “Transfer patient to ______” is not sufficient. Legal Documentation Remember, the entire chart is a legal document – this is not only the physician’s personal record of patient care – it is also available for perusal by the ancillary staff, the patient, or the patient’s lawyer! Written consent for invasive procedures or experimental/chemotherapeutic medication use is commonplace in Western medicine Forms document specific discussion regarding indication, procedural or treatment plan, and possible complications Legal Documentation Verbiage is included that indicates the patient’s understanding of these issues as well as a willingness to undergo the planned procedure or therapy This form is then signed and dated by both patient and physician Additionally, a witness to the patient’s signature and verbal agreement is present and signs the form This person should not be a direct member of the team which will perform the procedure or treatment Legal Documentation Operation reports and procedural notes are another form of legal documentation The specifics of the procedure or operation are documented in painstaking detail with reference to prepping, draping, sterile technique, and the like Finally both anticipated results and unanticipated complications are addressed For example, a procedural note for lumbar puncture in a 1-month-old infant might look like this: Lumbar Puncture Consent Written consent was obtained and all aspects of the procedure were discussed at length with the family to include indication, procedural technique, and possible complications. The infant was prepped and draped in sterile fashion and sterile technique was followed throughout. A 24 gauge spinal needle was introduced into the spinal canal at the L3/L4 intervertebral space using standard accepted technique – only one attempt was necessary to obtain cerebrospinal fluid (CSF) sample. Approximately 8 ml of CSF was obtained and sent for standard chemistries, cell count, gram stain and culture. Skin site was cleaned and sterile dressing was applied. Infant tolerated the procedure well. There was no blood loss or complication. Legal Documentation Some legal documentation serves only to avoid potential litigation and has no medical purpose – One such example is the documentation of a patient leaving against medical advice This process of self-removal from the inpatient hospital environment is referred to as “leaving against medical advice” or simply AMA Patients who wish to leave the hospital against the physician’s wishes are asked to sign a form that clearly states the same This documentation attempts to lessen the likelihood of litigation against the physician or hospital should the patient suffer a bad outcome as a result of early discharge Administrative documentation Purely administrative forms include routine paperwork associated with admission, transfer or disposition Additionally, completion of birth and death certificates, as well as insurance forms, can be considered mostly administrative tasks Typically these forms will require only the physician’s signature, as the details will have been filled in previously by the administrative support staff Needless to say, as in any situation where your signature certifies acceptance of whatever it is you are signing, it is important to review the information on the form for accuracy before signing Basic Tenets of Documentation Pay attention to prose The most basic requirement of medical documentation is not dissimilar to the basics of any effective writing – penmanship, word choice, and grammar are of paramount importance In documenting the patient encounter, one must ensure that the text is legible – an unintelligible entry is useless Unlike oral presentation, written documentation allows for (and encourages) the use of acronyms and abbreviations Nonetheless, a physician’s written assessment should reflect a sharp medical intellect and a graceful literary style Basic Tenets of Documentation Be efficient Medical records and outpatient chart entries should summarize presentation, evaluation, and care rendered in the most efficient manner possible The documentation of the most minute detail is often unnecessary – an abridged version of the story often is most appropriate With time and experience students learn to master the art of documenting a condensed version of the case The use of accepted acronyms and abbreviations also allows for more concise documentation Students and staff alike should avoid using arcane or little known acronyms or abbreviations Basic Tenets of Documentation Do not sacrifice details for space considerations In focusing your documentation, be sure to include all relevant information – leaving out important details in an effort to conserve space is a mistake that should be avoided Early on in your career it is best to err on the side of including too much information rather than overlooking vital details in an effort to be concise With regard to history and physical this translates into the recording of pertinent positives and negatives – inclusion of everything the patient may have said and the entire physical examination is usually unnecessary Reasoning behind medical treatment or surgical intervention should be recorded clearly The medical record should allow any reasonably experienced member of the medical team to understand your thinking. Basic Tenets of Documentation Ensure that the information flows logically Regardless of the case complexity or medical setting, documentation should follow a logical pattern That is, the basic design of the patient encounter should be reflected in the documentation – just as it is in case presentation Historical facts should be recorded first, with physical findings and diagnostic studies following next Basic Tenets of Documentation Organize your thoughts Documentation format typically reflects case complexity Straightforward outpatient (and sometimes inpatient) charting is organized using the standard S.O.A.P. format while cases of limited complexity are typically organized by problem Significantly complex inpatient care is usually documented utilizing a “by system” approach S.O.A.P – Straightforward Subjective, Objective, Assessment, and Plan This is by far the most commonly used documentation format – as the vast majority of medical practice involves the diagnosis and treatment of common disorders in an outpatient setting As with presentation, clearly delineating the subjective and objective portions is required Within the standard SOAP format, the assessment is often simply a notation of the diagnosis and possibly an indication of the exact etiology The plan is typically a numbered listing of items comprised of treatment, patient education, and follow-up Often the assessment and plan are listed together as “A/P” and the entry that follows is a hybrid of the two S.O.A.P – Straightforward S) O) 33-year-old o/w healthy ♂ with c/o 4-day h/o ↑’ing bilateral eye irritation and discharge. Afebrile - o/w healthy – no chronic medical conditions. + contact with friend experiencing similar sx’s GEN: HEENT: PERRLA - Alert, NAD Bilateral scleral injection and conjunctival hyperemia + mucoid discharge/crusting at lid margin EOMI no pain with movement of eye, NL visual fields - Vision 20/20 No evidence of peri-orbital edema A/P) Conjunctivitis – viral vs. bacterial High probability of viral etiology, however, given increasing symptoms and nonverification of bacterial source via culture, will treat empirically for likely bacterial pathogens Polymyxin B / SUL-TMP ophth soln 4 drops in each eye QID X 5 days as directed RTC if sx’s worsen or persist greater than 5-7 days without improvement, eye pain develops, or visual deficit occurs Dx, etiology, prognosis, disease course, med use/side fx, and hygiene discussed with patient at length By PROBLEM – Limited Complexity In an effort to maintain adequate organization in cases of limited to moderate complexity, a “by problem” approach is used to document the assessment and plan As discussed earlier, the historical and physical data format (subjective and objective) rarely changes, regardless of complexity Quite simply, the by problem approach involves listing out the patient’s individual problems or diagnoses and documenting an individual plan for each “By problem” Assessment and Plan A/P) Atopic dermatitis Acute treatment of symptomatic flare with topical hydrocortisone 2.5% ointment TID for 10 days Regular and liberal use of emollient each day – applied at a minimum in the morning, after water exposure, and before bed Mild Persistent Asthma Continue BID use of inhaled corticosteroids as maintenance therapy Albuterol MDI 1-2 puffs via spacer q4-6 hours prn cough, chest tightness, etc. RTC/ER if required > q4h Allergic Rhinitis Continue nasal corticosteroid inhaler at one spray each nostril qHS for maintenance Patient to follow-up in 6-8 weeks for ongoing care of above – RTC sooner for any increased symptoms or concern By SYSTEM approach – Complex A by system documentation style is reserved for the most complex medical patients Traditionally the subjective and objective data remains at the initial portion of the chart entry, with the assessment and plan alone broken down into systems. In extremely complex and heavily-detailed cases, even the subjective and objective portions may be broken down into systems! “By problem” FEN: Pt has 18 gauge IV site in left antecubital fossae. Full maintenance IVF while NPO awaiting angiocath. Strict monitoring of I/O’s. Chem 7 qAM. Adequate urine output over past 24 hours. CV: Patient with significant history of cardiovascular disease. HTN controlled with daily ACE-inhibitor therapy, history of stable angina with symptomatic relief provided with nitroglycerin sublingual tabs. On exam, patient has RRR with no evidence of M/R/G. Distal pulses are strong. HR is 64 and BP is 140/88. Plan for continued outpatient medication therapy while admitted with strict monitoring of BP (as he remains high-normal despite medication). Classic systems used in documentation include. . . FEN: Fluid, electrolytes, nutrition HEENT: Head, eyes, ears, nose, throat CV: Cardiovascular PULM: Pulmonary GI: Gastroenterological GU: Genitourinary NEURO: Neurological DERM: Dermatological MS: Musculoskeletal By SYSTEM approach – Complex A by system approach is commonly reserved for intensive care unit documentation However, exceptionally ill ward patients may require a by system approach as well As ward patient complexity increases and a by system approach becomes increasingly warranted, you may also want to consider transferring the patient to an intensive care unit setting!! S N O O A T P E Final thoughts. . . Adherence to the principles presented here will guide you toward skillful documentation Students should bear in mind that the goal of documenting patient care is simply to create a clear and concise record of the patient’s presentation, evaluation, and treatment Staying focused on this objective will allow you to develop proficiency in documentation – thus adding another valuable tool to your medical arsenal Questions??