The Philosophy of - The Lauterstein
advertisement

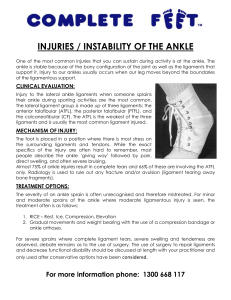
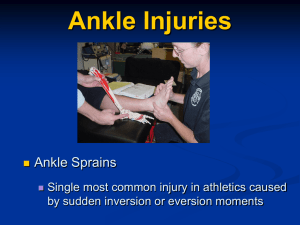
The Philosophy of Dimensional Massage Therapy by Nancy Dail, BA, LMT, NCTMB The body is all connected; it has depth, width and length. The joints in the body provide a network of anatomical structures designed for constant use. In order to properly relax and unwind soft tissue, the massage therapist must manipulate as many of these structures as possible. Each joint is a collection of muscles that work in groups and in paired opposition. By systematically working on specific muscles that share contraction and opposite action, Dimensional Massage Therapy (DMT) helps to create balance to the joint structures. DMT encompasses an approach to technique and structure as well as to the sequence of the specific techniques for a particular soft tissue problem. The techniques are a collection of soft tissue manipulations that are designed to be efficient and sequentially specific to unwind the most resistant hypertonicities. Dimensional Massage Therapy should provide the least amount of discomfort to the client in the therapeutic process, and if performed correctly the techniques should be easy on the therapist’s hands and body. Many DMT techniques first utilize passive shortening of the length of the muscle to efficiently soften fibers. Other DMT manipulations require rhythmically moving a joint at the same time as unwinding specific muscles or alternating clockwise and counterclockwise movements to joints or muscles. These “distractions” provide a mechanism for the client to give up “holding” patterns and the soft tissue fibers release built-up tension. All techniques should be sequenced according to the individual structure of the client. Therapists need to build a large “tool belt” of many techniques to adapt to the wide variety of structures and repetitive actions that plague humanity. Dimensional Massage Therapy provides a philosophical approach, sequence, and methodology of techniques for the massage therapist to utilize in a therapeutic practice. In her workshops, Nancy Dail takes a critical look at how posture and repetitive holding patterns and actions affect soft tissue responses. She presents in-depth lectures on anatomy and kinesiology illustrated with Power Point presentations clearly showing structural perspectives, trigger points, and referred pain patterns for the focus areas. With hands-on practice, Nancy demonstrates DMT techniques on specific muscles and their idiosyncrasies, and the individual structure of the receiving person on the table. Inversion Ankle Sprains Ankle sprains are one of the most common injuries among physically active people. Sprains involve the stretching or tearing of one or more ligaments. Ninety-five percent of all ankle sprains result from excessive inversion, which causes damage to the lateral ligamentous structures, primarily the anterior talofibular ligament and the calcaneofibular ligament. Although the fibula prevents most eversion sprains, excessive eversion forces can occur, causing injury to the deltoid ligament on the medial aspect of the ankle. Ankle sprains can be somewhat avoided by keeping the entire ankle strong and flexible. When the weight of the body is behind a fall and forces the foot into an unnatural, inverted position, it puts too much strain on the ligaments of the ankle. Fluids rush into the painful area and often cause a secondary trauma to the area. The peroneal muscles become stretched in the action, and specific ligaments fall prey to the inversion sprain. The anterior talofibular ligament is located at the distal end of the anterior fibula, attaching distally to the talus. The calcaneofibular ligament is located at the very distal end of the fibula at an angle to the calcaneus. On either side of the calcaneofibular ligament, tacking down the peroneal tendons, are two tissue bridges called the superior peroneal retinaculum and inferior peroneal retinaculum. If the sprain mechanism is significant, these tissue bridges could be torn and the peroneal tendons might ride up over the lateral malleolus as a result. When the sprain involves the ligaments, retinacula, and possibly the extensor digitorum brevis, there will be a great deal of spelling. Ice will help reduce the inflammatory response and possible secondary trauma due to the swelling, but it has to be applied immediately for best results. It is never too late to work on the small structures of the foot. Years after being injured, old sprained ankles can harbor puffiness around the lateral malleolus. A technique that addresses injury to the involved ligaments includes deep transverse friction to the anterior talofibular ligament and calcaneofibular ligament. In a prone position flex the client’s knee joint. Locate the ligaments. Apply your thumb at a right angle to each ligament and draw across it. Walking with a limp affects the knee, hip, and low back. From a dimensional perspective the massage therapist should treat compensatory muscles affected by the injury. A careful medical history including evaluating active and passive ranges of motion for the leg, ankle, and foot lead to a better treatment protocol and appropriate sequence critically thinking about the involved joints and muscles. Bodywork does not have to be mysterious; it should be based on science, the structure of the client, and the art of applying techniques in a knowledgeable fashion. Success is at your fingertips. Nancy W. Dail, BA, LMT, NCTMB co-authored Kinesiology for Manual Therapies published by McGraw-Hill in January 2010. The above philosophy is peppered throughout the text, introducing technique after each major joint in the body. Information about the structure of the ankle and foot can be found in chapter 19 and the techniques are located in chapter 20. Nancy will address ankle sprains and much more in her workshop that will be held at Lauterstein Conway School of Massage on June 7, 8, 2014 in Austin, Texas.