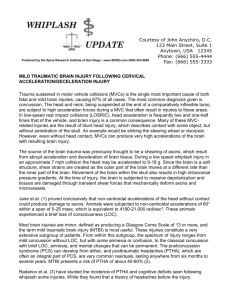
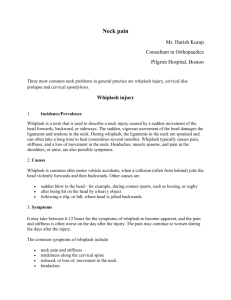
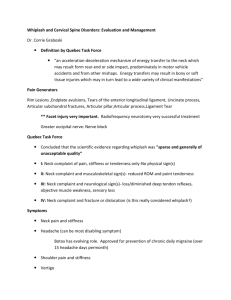
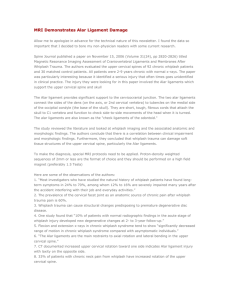
An Overview of Cervical Facet Injury Due to RearImpact Automobile Collisions DR. BARRY L. MARKS PRACTICE OF CHIROPRACTIC --EMPHASIS ON AUTOMOBILE & INDUSTRIAL INJURIES ORANGE, CALIFORNIA (714) 938-0575 “S” Shape Spine the Source of Damage to Cervical Facet Joints in “Whiplash” Injuries In 1997 MM Panjabi and JN Grauer of the Dept. of Orthopaedics and Rehabilitation at Yale University School of Medicine conducted “whiplash” studies on human cadavers. The cadavers were subjected to forces simulating a rearimpact automobile collision while high speed motion x-rays caught the effects on film. Researchers made a startling new discovery. It was always thought that hyperextension occurred in the neck, which resulted in “whiplash” injuries. This study in 1997 found that the lower vertebrae of the neck (C5-6) actually changed their axis of motion and spun backwards causing their posterior joints (facets) to collide, while the top of the neck was bent forward momentarily. At a given point into the collision, the neck actually formed an “Sshape”.[1] This study found much attention and in 1998 Panjabi MM, Cholewicki J, Nibu K, Grauer JN, Babat LB, Dvorak J and Bar HF repeated the study at the Yale University School of Medicine only this time using live human subjects. The principles of the 1997 study were able to replicate the results of the previous test on live human volunteers. The same “Sshaped” configuration was noted and the lower cervical facet extension was noted. The test was performed at various collision speeds to find the human tolerance for such an injury. The results were shocking. The “S-shape” configuration was observed in speeds as low as 2.5 mph.[2] In 1999 Koji Kaneoka, Koshiro Ono, Satoshi Inami and Koichiro Hayashi of the Department of Orthopedic Surgery at the University of Tsukuba, Japan repeated the second Panjabi study, again on live human volunteers. The results were the same. This third study confirmed for the world of spinal researchers the mechanism by which human spines are damaged in rear-impact automobile collisions.[3] Analysis & Summary of Panjabi & Kaneoka Studies Human subjects were placed in vehicles that were subjected to rear-impact collisions at various speeds. The spine was recorded using high-speed motion X-rays, called cineradiography. At 50 milliseconds into the impact, the lower cervical vertebrae at C5-6-7, rotate into extension causing stretching and tearing of ligaments in front of the spine and compressing of facet joints resulting in facet joint surface damage. At maximum extension of C5-6-7, the upper vertebrae flex forward making an S-shape curve, stretching and tearing soft tissues of the back of the neck. The damage occurs in fractions of a second, before the patient is aware of the collision. The tests proved: 1. The spine deforms into an S-shape 2. Damage of the facets occurs in rear-impact collisions due to the rotation of the lower vertebrae into extension without “hyperextension” 3. The damage occurs prior to consciousness and before reflexes can protect the neck 4. Damage occurs at very low speeds, as low as 2.5 mph “The study of Kaneoka et al now fills a critical gap in the story of cervical facet pain. It provides the missing biomechanical link. Theirs is the most significant advance in biomechanics of whiplash since the pioneering studies of Severy et al in 1955” “As a result of this study, we no longer rely on inference or speculation; we have a direct demonstration of the mechanism of injury in whiplash.”[4] Nikolai Bogduk, MD, PhD, DSc, FAFRM Dept. of Anatomy and Musculoskeletal Medicine University of Newcastle Newcastle Bone and Joint Institute Royal Newcastle Hospital Newcastle, New South Wales, Australia The Facet Joints are the Primary Area of Damage and Pain in the Neck from Whiplash Injuries “Cervical (facet) joint pain is common among patients with chronic neck pain after whiplash… and has proven to be of major clinical importance”[5] Nikolai Bogduk, MD, PhD, DSc, FAFRM Due to the S-shape deformation of the cervical spine on impact, the facet joints are severely compressed causing damage to the articular cartilage surface. This results in predictable pain patterns that are readily identified on physical examination. The pattern of pain from an injured facet joint has been referred to as “Sclerotomal” pain. Unlike dermatomal pain, which describes pain from a nerve root to it’s corresponding body part like in a herniated cervical disc radiating pain into the arm or hand, Sclerotomal pain corresponds with embryonic origin of tissues so that a source of pain may be widely separated from it’s radiation pattern and has no corresponding neurologic connection. In the cervical spine facet joints, damage sends pain to the lateral aspect of the neck and down into the scapula region. It can be aggravated for diagnostic purposes by bending the neck laterally and into extension, compressing the facets and reproducing the pain pattern. Facet joint injuries CANNOT be found on MRI or electrodiagnostic tests like EMG and NCV, but objective proof can be found if the practitioner knows how to find it. Sclerotomal pain pattern of the cervical facet joints as described by Dwyer, Fracs, Aprill and Bogduk in December 1989 Annals of Surgery Delay in Onset of Symptoms Is Common and Can Affect Prognosis Delayed onset of symptoms is common according to the scientific literature.[6],[7],[8] More severe injuries, such as disc herniation and severe ligament tearing usually become symptomatic very quickly. Other less destructive injuries may take over 48 hours to materialize. A Spanish study found that 31.5% of rear impact crash victims reported to an ER between one and three days after the crash. [9] Later onset of symptoms has actually been linked to longer treatment duration and poorer prognosis. Richter et al found that symptoms lasted nearly twice as long as average for those with a delay in onset of more than 24 hours.[10] Another aspect related to delayed symptoms is the “second wave” phenomenon. This has been described by several authors. Wherein a whiplash victim initially complains of neck pain and then later, weeks, and even months later, a “second wave” or second phase of symptoms emerge. Bring and Westman (450) reported a second wave of symptoms occurring many months later. Gargan and Bannister (456) reported a late onset of neck pain, extremity pain or paresthesia, interscapular pain, tinnitus, headache, dizziness, and visual disturbance after 1 week supporting the “second wave” phenomenon. This accounts for those patients who are initially treated, found to be stationary and released only to return later with a return of old symptoms and often new complaints such as carpal tunnel syndrome, tedninopathies, post concussion syndrome, disc derangements, and others. Documenting Facet Joint Injuries As we have seen cervical facet joints are the leading factor in neck pain form automobile collisions. We have also learned that they occur even in very low speed collisions and that they cannot be visualized on MRI or with EMG or NCV tests. The documentation of facet joint injury and damage is done in two manners: 1. Clinical examination Subjective pain patterns for facet joints are predictable and reproducible. Careful documentation of the patient’s complaints leads to a suspicion of facet joint damage after a MVC. Objective examination procedures that provoke the facet joints can be employed and is a reproducible means of locating facet joint damage. Particularly, simultaneous lateral flexion and extension of the suspected joint will yield the characteristic pain pattern described earlier. Other compressive type tests, such as foramina compression and maximum cervical compression may also elicit the tell-tale findings. 2. Imaging Digital Motion Fluoroscopy is the imaging procedure used by Panjabi and Kaneoka in their landmark studies on whiplash injuries. It is a high speed x-ray that is able to display the skeleton as it actually moves. In essence, it is a live x-ray video. The images can then be analyzed by a radiologist for defects in motion. The most common defects found are of the alar and accessory ligaments of the C1-C2 vertebrae, which manifests as excessive lateral movement of the C1 segment and the facet capsular ligaments of C2 through C7, which appears as excessive gapping of the involved facet joint(s). Chiropractic Treatment Best for Whiplash Injuries Facet joint injuries require appropriate treatment to minimize or prevent later complications such as arthritis. A 1996 study by renowned researchers Gargan and Bannister, indicated: "…benefits can occur in over 90% of patients undergoing chiropractic treatment for chronic 'whiplash' injury." "No conventional (medical) treatment has proven to be effective in these established chronic cases." [11] Therefore, chiropractic care is the patient's best chance of improving when suffering from whiplash injuries, even late or chronic whiplash. Chiropractic treatment benefits the patient with damaged facet joints by restoring normal motion and mechanics to the cervical facet joints through manipulation and rehabilitative therapies and exercises. Croft Guidelines for Whiplash Severity & Treatment In 1993, Arthur Croft, D.C., M.S., M.P.H., F.A.C.O., F.A.C.F.E., published a set of management guidelines in the ACA Journal. These guidelines have also been published in Whiplash Injuries: the Cervical Acceleration/Deceleration Syndrome, second edition, in 1995 and in a recent Canadian practitioner's guide to whiplash injuries, sanctioned by the Canadian Chiropractic Association. The Croft Guidelines have been a part of our literature now for eight years. No competing guidelines relative to CAD treatment have been published during that time, with the exception of the Quebec Task Force Guidelines on WAD, but these are only applicable for patients who remain on disability. Several American state chiropractic organizations and associations, as well as in at least one Canadian province, have now adopted the Croft Guidelines. Grades of Severity of Injury Grade 1 - Minimal; No limitation of motion; No ligamentous injury; No neurological findings Grade 2 -Slight; Limitation of motion; No ligamentous injury; No neurological findings Grade 3 - Moderate; Limitation of motion; Ligamentous instability; Neurological findings may be present Grade 4 - Moderate to Severe; Limitation of Motion; Some ligamentous injury; Neurological findings present; Fracture or disc derangement Grade 5 - Severe; Requires surgical management and/or stabilization Guidelines for Frequency and Duration of Care in Cervical Acceleration/Deceleration Trauma Daily TN Grade I <21 Grade II <33 Grade III Grade IV Grade V 3x/wk 2x/wk 1x/wk 1 wk 1-2wk 2-3 wk <4 wk 1 wk <4 wk <4 wk <4 wk 1x/mo --1 TD <11 wk <4 mo <29wk 1-2 wk <10 wk <10 wk <10 wk <6 mo<56 wk <76 2-3 wk <16 wk <12 wk <20 wk --2 --2 --2 Surgical stabilization necessary - chiropractic care is post-surgical TD = treatment duration; TN = treatment number 1 = Possible follow-up at 1 month 2 = May require permanent monthly or p.r.n. treatment The most common whiplash injuries are Grade II and Grade III. Occasionally, Grade IV’s will present, but they are fairly rare. Grade V’s are seen only after extensive and invasive treatment has been performed through an orthopedic or neuro surgeon. Grade I’s are fairly rare also as the pain level may not be enough to prompt the patient to seek evaluation and/or they have been examined by another medical provider who did not recognize the need for care in these patients. Duration of Care for Whiplash Injuries Medical researchers point to the fact that a minimum of 25% of all motor vehicle collisions result in chronic pain that may take up to 2 years before becoming stabilized.[12] Other authors have stated the figure to be over 40%.[13] Schofferman and Wasserman in SPINE Vol 19, Number 9, 1994 found the “average” collision induced injury to take 7 months and 1 week before becoming stable. They mentioned “tough” cases take approximately 108 weeks or about 2 years. Lastly, Ryan and Taylor, et al found 66% of patients had not recovered 6 months post-accident.[14] These figures roughly approximate the Croft Guidelines and can be simplified to generalize that: Grade I injuries can take up to 3 months to stabilize Grade II injuries can take up to 7 months to stabilize Grade III injuries can take up to 14 months to stabilize Grade IV injuries can take up to 2 years to stabilize Poor Prognosis for Chronic Whiplash “25% of whiplash injuries will progress to chronic symptoms. These patients injured their discs or facet joints. These patients will not resolve spontaneously and they do become chronic. They may improve over a period of 2 years, but are unlikely to improve after 2 years.” “10% of patients with whiplash injuries develop constant severe indefinite neck pain.”[15] Other studies have found the chronic cases number to be even higher. A consensus of recent research found the chronicity rate to be 38%[16] Osteoarthritis 6 Times More Likely After Whiplash Damage to the facet joint surface leads to breakdown of the tissue and permanent arthritic changes. Studies by Hohl and Miyamoto et al. report increase incidence of osteoarthritis following whiplash that is permanent often leaving the victim with years or perhaps a lifetime of residual pain and disability.[17],18,19 Summary The latest scientific and medical research indicates that it is the "S" configuration of the spine tat results in damage to the neck in rear-impact motor vehicle collisions. These injuries can occur at very low speeds. The facet joints are the most commonly damaged structures within the neck from these collisions. There may be a delay of symptoms from hours to days and in some cases even longer. Clinical and radiological tests can readily detect these injuries. Chiropractic has been shown to be the preferable treatment of these injuries and is particularly helpful in chronic or late whiplash. Late whiplash occurs in up to 38% of cases and increases the chance to develop early osteoarthritis. References [1] Panjabi MM, Grauer JN (1997): "Whiplash produces a S-shape curvature of the neck with hyperextension at lower levels. " Spine 22 (21): 2489-94. [2] Panjabi MM, Cholewicki J, Nibu K, Grauer JN, Babat LB, Dvorak J, Bar HF (1998-12-01): "[Biomechanics of whiplash injury]." Orthopade 1998 Dec; 27(12): 813-9. [3] Koji Kaneoka, Koshiro Ono, Satoshi Inami and Koichiro Hayashi (99-04-15). "Motion analysis of cervical vertebrae during whiplash loading." Spine 24(8): 763-770 [4] [5] Spine 1996; 21: 1737-1745 Pain, 54 (1993) 213-217 Gotten N: Survey of one hundred cases of whiplash injury after settlement of litigation. JAMA 162(9):865-867, 1956. [7] Deans GT, Magalliard JN, Kerr M, Rutherford WH: Neck sprain--a major cause of disability following car accidents. Injury 18:10-12, 1987. [8] Braaf MM, Rosner S: Symptomatology and treatment of injuries of the neck. NY State J Med 55:237-242, 1955. [9] Loro MBG-M, Yuste PG, Perez CG, Garcia MTM, Lorenzo AH. Epidemiology of traffic crashes in a general hospital. 43rd Annual Proceedings of the Association for the Advancement of Automotive Medicine. September 20-21, 1999, Barcelona, Spain, 437-438. [10] Richter M, Otte D, Pohlemann T, Krettek C, Blauth M. Whiplash-type neck distortion in restrained car drivers: frequency, causes and long-term results. European Spine Journal 9:109117, 2000. [11] Injury 27(9): pp. 643-645 [12] Barnsley, Lord, Bogduk, Whiplash Injury Clinical Review, Pain 58, 1994, pp. 283-307 [13] Woodward, Cook, Gargan and Bannister (1996) "Chiropractic treatment of chronic 'whiplash'." Injury 27(9): pp. 643-645. [14] Ryan, G., V. Taylor, et al. (1994). “Neck strain in car occupants: injury status after 6 months and crash-related factors.” Injury: International Journal of the Care of the Injured 25 (8): 533-537. [6] [15] Whiplash Injury Clinical Review Lord, Barnsley and Bogduk Pain 58, 1994, 283-307 9th Annual SRISD Scientific Conference, Coronado, CA November 2004 [17] Foreman, D. and Croft, A., Whiplash: The Cervical Acceleration/Deceleration Syndrome, 1989, Williams & Wilkins 18 Hohl M: Soft tissue injuries of the neck. Clin Orthop Rel Res 109:42-49, 1975 19 Miyamoto S: Spine 16(10):5495-5500, 1991 [16]
 0
0
advertisement
Related documents


Download
advertisement
Add this document to collection(s)
You can add this document to your study collection(s)
Sign in Available only to authorized usersAdd this document to saved
You can add this document to your saved list
Sign in Available only to authorized users