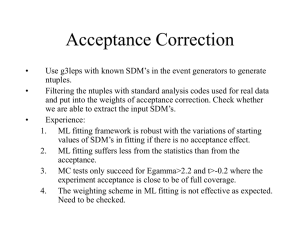
SDM® and Critical Thinking in Child Welfare Assessment
advertisement

SDM® and Critical Thinking in Child Welfare Assessment TRAINEE CONTENT Table of Contents Introduction ………………………………………………………………………... 3 My Learning Goal ………………………………………………………………….. 5 Benefits of Standardized Assessment ……………………………………………. 7 Decision Making …………………………………………………………………… 15 Minimum Sufficient Level of Care ………………………………………………… 19 Safety and Risk …………………………………………………………………….. 23 Safety and Risk Worksheet ………………………………………………………... 25 SDM Flow Chart Worksheet ………………………………………………………. 27 Protective Capacity ………………………………………………………………... 29 Family Friendly Interview Sample ………………………………………………… 33 Common Core | SDM and Critical Thinking: Trainer's Guide | Version 1.21, 2011 1 This page intentionally left blank. Common Core | SDM and Critical Thinking: Trainer's Guide | Version 1.21, 2011 2 Introduction This trainee content contains icons indicating content related to California’s themes of practice: Fairness & Equity Family & Youth Engagement Strength-based Practice Outcomes-informed Practice Evidence-based Practice These themes are interwoven throughout the Common Core Curricula in California. Trainees are encouraged to pay special attention to the themes and make efforts to incorporate the concepts in their daily practice. Common Core | SDM and Critical Thinking: Trainer's Guide | Version 1.21, 2011 3 This page intentionally left blank. Common Core | SDM and Critical Thinking: Trainer's Guide | Version 1.21, 2011 4 My Learning Goal Reviewing the learning objectives at the beginning of the training allows the adult learner to identify priority learning goals and gain a better understanding of what to expect from the training. Select a priority learning goal for yourself. Use the space below to note the goal. My priority learning objective is: Common Core | SDM and Critical Thinking: Trainer's Guide | Version 1.21, 2011 5 This page intentionally left blank. Common Core | SDM and Critical Thinking: Trainer's Guide | Version 1.21, 2011 6 Benefits of Standardized Assessment Child Welfare Assessment Practice Public child welfare agencies exist with one primary goal: to prevent the recurrence of maltreatment of children who come to the agency’s attention. One key child welfare effort toward meeting this goal is accurate and timely assessment. Our efforts to provide children and families with the best possible assessments, those backed by research and supported by ongoing quality assurance have led us to use standardized assessment tools. Beyond the effort to use the best practice tools available to provide assessment, there are six additional reasons we use standardized assessment tools: 1. The Law Requires It The Adoptions and Safe Families Act (ASFA), as well as prior legislation mandate the goals for child welfare: safety, permanence, and well being. State law (Welfare and Institutions Code, Section 300, and related Penal Codes) and state regulations (Division 31 and related regulations) provide the legal means and policy and procedure for intervening in families where maltreatment is suspected. 2. Our Professional Standards and Values Support It The Standards and Values for Public Child Welfare Practice adopted by the County Welfare Directors Association (CWDA) and the California Department of Social Services (CDSS) in 1996 and revised in 2005 include many references to the importance of high quality, fair, and equitable assessment (California Social Work Education Center, 1997). 3. The Practice Defines Agency Parameters Effective assessment allows social workers to identify children in need of intervention thereby limiting unnecessary intrusion in the lives of families where safety and risk are not an issue. 4. The Practice Promotes Consistency in Decision making Using a tool to complete safety and risk assessment promotes consistent decision making and interventions that “clarify the agency’s responsibility in the protection of children” (Brittain, C.R., & Hunt, D.E. [eds.], 2004). 5. The Practice Supports Focused Interventions Assessment of safety, risk and protective capacity helps to focus in on the most immediate issues and “drive” specific interventions. By identifying the factors that lead to an unsafe household, the service plan specifically identifies the services needed to alleviate risk. Common Core | SDM and Critical Thinking: Trainer's Guide | Version 1.21, 2011 7 6. The Practice Supports Accountability Factors identified in the tools structure the assessment practice and help identify the safety, risk and protective capacity concerns in behavioral terms. Once an assessment has identified the concerns, subsequent assessments can determine whether the services have helped to alleviate the safety concerns. “Well-constructed assessment models assist in managing accountability” (Brittain, C.R., & Hunt, 2004). The Value of Research-based Tools Imagine a patient going to a doctor with an upset stomach and having the doctor recommend immediate surgery without completing any assessment, testing or diagnosis. The patient would want to know how the doctor arrived at that decision and would not be happy if the doctor said, “On the surface it seems like a simple virus, but I have a gut feeling it’s something far more serious” or “my mother and grandmother both died of cardiac arrest because someone ignored their presenting problem of indigestion. I’m not going to let that happen to any of my patients.” Next, imagine that something went bad with the treatment plan and the doctor’s explanation was, “I have experience and education, and based on that when I considered this case I made my decision.” Imagine that in medicine, there were no research trials, no diagnostic tests, no diagnostic decision trees, and no generally accepted standards of practice. In medicine, there can be differences of opinion--that’s why second opinions are sought. But imagine the inconsistency being so great, that whether you were given an aspirin, a cast or an operation depended more on who you went to see rather than on your medical need. Critical Thinking Supported by Evidence Based Tools The Structured Decision Making (SDM) assessment system provides social workers with a standardized set of tools to help social workers make assessments at critical points in child welfare cases. While social workers must use critical thinking and engagement skills to make assessments, accurate use of the SDM model used in conjunction with critical thinking and engagement provides an evidence based tool to guide social workers in the decision making process. The SDM tools were developed with a significant amount of research evidence and real world experience: the Children’s Research Center (the developer of the SDM model) has long standing roots, starting in 1986 to the present, in the United States and internationally SDM has been implemented in California and over 30 other child welfare jurisdictions, including Alaska, Florida, Georgia, Nevada, Illinois and parts of Australia and Canada. Common Core | SDM and Critical Thinking: Trainer's Guide | Version 1.21, 2011 8 Assessments and Improvement in Federal Outcomes State and federal reviews focus on data indicators of improved safety, permanency and wellbeing and funding is tied to ongoing improvements in these outcomes. The SDM model does not address every single one of these indicators, but it does address many of them. In particular, the SDM model is designed to, and in many instances has evidence that it does: • Reduce future referrals and substantiations • Reduce future foster placements • Reduce time to permanency Many programs are designed to achieve these same goals, and the SDM model alone does not guarantee success. What makes the SDM model unique is the way it contributes to meeting these goals. The SDM model helps improve assessments by increasing consistency and accuracy. Good assessments, however, have no value unless the results directly affect practice. In the SDM model, assessment results lead to presumptive case actions that are designed to increase the effectiveness and efficiency of available resources. Finally, because every assessment completed by a social worker contributes to a pool of rich aggregate data, managers and administrators are given information they need to make good policy, program, budget, and other decisions. Social workers who use the SDM system accurately can expect the following benefits: 1. Reduced rate of subsequent abuse/neglect referrals and substantiations through improved ability to identify and address key factors associated with safety, risk and protective capacity. 2. Reduced rate of subsequent abuse/neglect injuries to children. 3. Reduced rate of subsequent foster care placement. 4. Reduced length of stay for children and time to permanency in foster care. 5. Improved assessments of family situations to better ascertain the protection needs of children. 6. Increased consistency, accuracy, and equity in case assessment and case management among child abuse/neglect staff within a county and among counties through improved ability to focus on the same factors for all families. 7. Increased efficiency of child protection operations by making the best use of available resources. Common Core | SDM and Critical Thinking: Trainer's Guide | Version 1.21, 2011 9 8. Improved availability of data for program administration, planning, evaluation, and budgeting. Limiting the Effect of Random Chance The absence of standardized assessment in child welfare allows chance to play a large role in child welfare outcomes: A 1997 study of child welfare removals found that social worker assignment better predicted likelihood of removal than any information about safety. The study concluded that chance played a key factor in predicting outcomes (Rossi et al, 1997). The SDM model addresses this element of chance by focusing assessment on key factors linked to safety and risk. Accurate use of SDM provides clear connections between safety and risk factors in the home and decisions made by social workers to ensure safety and mitigate risk. Identifying Key Factors In addition, the SDM model effectively helps social workers identify and address key factors associated with safety and risk: In 1995, several years after Michigan first implemented the SDM model in a group of 12 counties, outcomes were measured in SDM counties and compared to the outcomes from a set of matched comparison counties (Wagner, D., Hull, S., & Luttrell, J., 1995). Approximately 900 families entering CPS in each group were followed for 12 months after the initial investigation. Families in SDM counties were much less likely to experience subsequent referrals, substantiations, foster placements, and abuse-related injuries. Addressing Disproportionality In order to be fair and in an effort to address disproportionality in child welfare outcomes, it is important to use the same criteria for assessing all families. SDM helps social workers ensure that all families are assessed on the same criteria. Children of color, particularly African-American and Native-American children, continue to be over-represented in the child welfare system relative to their proportion of the population. According to the 2004 National Fact Sheet on Disproportionality (Child Welfare League of America): The challenge [in child welfare services is]…. the considerable evidence of the following trends among children of color, particularly African-American and Native-American children: Greater likelihood to be removed from their mothers as infants Higher rates of foster care entry Common Core | SDM and Critical Thinking: Trainer's Guide | Version 1.21, 2011 10 More time spent in foster care Fewer services and less contact with child welfare staff Lower reunification rates Longer time to adoption and lower adoption rates Part of this disproportionality relates to the ability of the child welfare system to conduct fair and equitable assessments throughout the life of a case. As you can see from the table below, data from 2009 reveal the continued overrepresentation of African American and Native American children in the child welfare system in California (Needell et al, 2010). California: Ethnicity and Path Through the Child Welfare System, 2009 (missing values & other race excluded from % calculations) *includes children age 18 100% 90% 0.5 10.6 0.8 4.0 1.0 3.8 1.2 3.2 1.1 3.2 1.3 2.6 80% 70% 60% 52.9 53.4 49.7 45.9 48.3 Asian/PI 51.1 50% Hispanic 40% 24.4 30% 20% 27.4 26.5 25.6 25.6 31.8 10% 0% Native American 6.0 Population (9,992,333) White Black 15.0 15.3 Allegations (471,809) Substantiations (92,231) 20.2 Entries (31,588) 25.7 21.7 In Care (59,509) Exits (37,382) CRC (the developer of the SDM model) is committed to ensuring that SDM assessments are equitable across ethnic groups and they have conducted research to show that the SDM model does not disproportionately identify children from any ethnic or racial group as being unsafe or at risk. Their research completed in California demonstrates that the SDM™ Risk Assessment accurately classifies families into low, moderate, high, and very high risk categories regardless of ethnicity (Johnson and Wagner, 2003). Common Core | SDM and Critical Thinking: Trainer's Guide | Version 1.21, 2011 11 Consistency Ensuring that every social worker addresses a common set of factors appropriate at each decision point is key to improving the consistency of decisions made by social workers. Each decision point and each factor used to make the decision is defined so that there is less chance of varied interpretations. Finally, each tool leads to a presumptive decision. In this way, the relative weight of each item as it relates to the final decision is consistent. It is important to remember that the objective is not uniformity. The field is too new and too complex to expect that everything can be reduced to perfect uniformity. Still, it is appropriate to increase consistency. Consider the following evidence for how SDM tools help social workers improve consistency in their decision making: SDM’s research based risk tool used in Michigan was compared to the 1990’s Fresno risk tool, and another risk tool used in the state of Washington. Four case readers were trained in each model (trained by the proponents of the model to assure adequate training). They were then asked to read case abstracts based on actual cases from four jurisdictions across the country, including Alameda County. The readers used their respective tools to assign a low, moderate, or high risk level to each family. The research based tool achieved perfect agreement in nearly 60% of the cases reviewed. The other tools achieved this in less than 15% of cases. A lower threshold of consistency was evaluated as well: perhaps 100% agreement is too rigorous a standard, but perhaps we could expect that at least 3 out of 4 social workers would agree on the family’s risk level. Nearly 90% of the cases evaluated using SDM achieved 75% agreement. But only about half of the same cases, when evaluated using one of the consensus based tools, had 75% agreement (Wagner, D., Hull, S., & Luttrell, J., 1995). Accuracy SDM tools also increase accuracy. For example, a risk tool’s job is to estimate the likelihood of future maltreatment. So if we had a group of families the tool said were low risk and another group called high risk and we followed those families for a year or two, we would expect to see more incidents of subsequent maltreatment among the high risk families. Common Core | SDM and Critical Thinking: Trainer's Guide | Version 1.21, 2011 12 Consider the following evidence of improved accuracy with the SDM tools: Wagner et al (1995) examined accuracy by assigning a risk rating to families using one of the three tools and then allowing readers to read the rest of the case record to find out what actually happened. The raters using the research based tool from Michigan’s SDM model had excellent results. Families assigned into the low risk category had only half the recurrence rate as moderate risk families, who in turn had only half the rate as high risk families. The Fresno risk assessment, however, had almost no distinction among families assigned to different risk groups. The Washington tool did a little better at distinguishing high from moderate risk groups, but even with this tool families were only about a third as likely to experience future harm. There was no difference between low and moderate risk. In other words, these tools required work to complete, and labeled a family, but that label related poorly to what actually happened. More recent research looking at families over several years, found that social worker assessments completed using the SDM California Family Risk Assessment Tool did a better job at predicting risk than social worker assessments alone (Johnson, 2011). Making the Best use of Limited Resources SDM tools can help jurisdictions determine the best use of limited resources. SDM tools are used to organize information about a family. That information is valuable only to the extent that it matters in terms of what decisions are made. Every SDM tool has policies designed by the jurisdiction (in this case, California), outlining how to use the tool’s results to shape decisions in ways that increase the effectiveness and efficiency of CPS and have the greatest potential to reduce harm to children. Consider the following evidence that identifying high risk families through the use of an assessment tool improves efficiency: Research done in several urban Wisconsin counties revealed that providing CPS services to families at low and moderate risk seemed to have virtually no impact on reducing subsequent harm. In contrast, providing services to high and very high risk families reduced subsequent referrals in half. For example, very high risk families who did not receive services had about double the re-referral rate as families with the same initial risk levels that were opened for CPS services (Wagner, D. & Bell, P., 1998). Common Core | SDM and Critical Thinking: Trainer's Guide | Version 1.21, 2011 13 As effective as SDM tools can be at guiding decisions at the case level, the same information needed for those decisions in each case can be aggregated. This aggregated information is extraordinarily useful for making decisions at the level of the agency and the community. Multiple Benefits Many programs are designed to achieve these same goals, and the SDM model alone does not guarantee success. What makes the SDM model unique is the way it contributes to meeting these goals. The SDM model helps improve assessments by increasing consistency and accuracy. Good assessments, however, have no value unless the results directly affect practice. In the SDM model, assessment results lead to presumptive case actions that are designed to increase the effectiveness and efficiency of available resources. Finally, because every assessment completed by a social worker contributes to a pool of rich aggregate data, managers and administrators are given information they need to make good policy, program, budget, and other decisions. Common Core | SDM and Critical Thinking: Trainer's Guide | Version 1.21, 2011 14 Decision Making Before attempting to employ the SDM tools for assessing children and families, it is important to look closely at the process of making decisions and thinking critically about the key factors involved in the decision making process. The 5 step decision making process outlined below helps social workers go about decision making in a way that encourages critical thinking and helps social workers avoid decision making pitfalls such as red herrings, personal bias and crisis driven thinking. This process (adapted from Stein and Rzepnicki, CalSWEC, 2007) can help social workers think about making decisions in a more systematic way through gathering information, applying criteria, using discussion/feedback, implementing a decision and reviewing outcomes. Step 1: Information Gathering The first step in any decision is to gather the relevant information. An important distinction here is that we don’t need all the information, just the right information. The more information we gather, the more confident we feel about our process, but the less accurate our decisions are. Our memories can only hold a limited amount of information and we do not necessarily keep the most important facts. We are more likely to have better recall of facts that are similar to other familiar situations. Also, because gathering and considering extraneous information can introduce bias in the decision making process, the more information you collect the more biased you may become. For example, when preparing a resume or completing a job application, it is best to avoid adding extraneous information unrelated to the job. Such information (e.g.; a favorite movie) is irrelevant to the hiring decision but may introduce bias in the employer (“If this applicant likes that movie, she is probably nerdy or self-righteous. I don’t want to work with someone like that!”). In addition to actively gathering the relevant information, social workers must assess the reliability of the information. As noted by Brittain and Hunt (2004), “to make good decisions, you must have reliable information.” Information for assessment and decision making can be gathered from a variety of sources and people. A crucial activity will be documenting and then further evaluating the information as it is received. In these activities social workers demonstrate their accountability to children, families and the agency. It is important to consider the point of view of the person providing information and gather information from more than one perspective. It is also important to avoid drawing conclusions while you are still gathering information. If you gather information with a specific conclusion already in mind, you may be more likely to interpret facts to support the conclusion you’ve already reached. This introduces bias in the information gathering process. Common Core | SDM and Critical Thinking: Trainer's Guide | Version 1.21, 2011 15 Consider the following activities as you gather information: Preparatory Activities: Get needed training in interviewing adults and children. Read previous reports, case referrals, and dispositions if available. Discuss with your supervisor a strategy for interviewing adults and children. Be prepared for adverse reactions from parents and families. Be clear about your role. When Interviewing: Be open-minded and respectful of the person(s) you are interviewing. Be mindful of cultural issues and use of language. Communicate your concern for family members. Acknowledge and clarify the information that is being told to you. Ask open ended questions to elicit more information. Watch for escalation of feelings and be prepared to de-escalate. Taking notes is recommended. Recognize that the interview process ebbs and flows. When Documenting: Be aware of your county’s policy and procedure on documenting contacts. Documentation includes narrative, court reports, voice mail, email, letters, and memos. When documenting, use facts and statements and only write conclusions in assessment sections as designated by policy and procedure. The data you enter into a computer system is critical in providing accurate information to the agency, state and federal government about outcomes of children and families. With only this first step to think about, the social worker already has a lot to do in gathering information. As we will see when we apply this decision making process, the SDM system helps the social worker by focusing on the most important factors to consider. Step 2: Application of Rules or Criteria After the relevant information is gathered for a given decision point, it must be analyzed by the social worker making the assessment and compared to accepted rules or judgment criteria. For child welfare social workers, this step requires that we apply the relevant facts we have gathered to: a legal definition of abuse or neglect, the associated state and local policies, and an established standard such as a minimum sufficient level of care. Common Core | SDM and Critical Thinking: Trainer's Guide | Version 1.21, 2011 16 In addition to considering individual pieces of information, we must also consider the way all the pieces interact to create a whole. At times the combined effect of all the key factors is significantly better or worse than any individual factor. Individual factors must be weighed against a standard, but the big picture must also be considered in its relationship to legal definitions, policies and minimum sufficient levels of care. This includes considering strengths and mitigating factors. As we learn more about the SDM tools, we’ll see that the tools have their own specific criteria and definitions, which classify certain behavioral and historical factors in terms of the level of risk to the child. When applying these specific criteria, social workers must adhere closely to the SDM definitions in order for the tools to work properly. Step 3: Decision/Professional Judgment The fourth step in the process involves reaching a decision. This step is best achieved with documentation of specific facts and observations and an explanation of how the specific facts and observations lead to the identified conclusion. It is also important to identify how the decision ensures the child’s safety and ensures that the family receives appropriate services. This may mean justifying specific interventions, but it may also mean justifying the lack of intervention indicated by the situation at hand. Both decisions should reflect that information was gathered, applied to a specific standard and discussed with others. There should be a clear relationship between the information gathered and the conclusion. The SDM system supports this step in the process by walking the social worker through the process of considering the right information, applying definitions and policy to the information, facilitating review and documenting the conclusion. It is important to remember that it is still the social worker making the decision; SDM only guides the process. Step 4: Discussion/Feedback Once the information has been gathered and criteria applied, additional resources and feedback are sought to insure an accurate decision. Discussion and feedback may occur in a variety of venues, including consultation with a supervisor, unit case consultations, interdisciplinary meetings, family case conferencing, Team Decision Making and consultation with County Counsel. This can be helpful in situations with no clear direction, but it is also important to seek feedback when the answer seems obvious. Consultation provides an opportunity to identify errors or bias in our decision making. This process involves combining our professional judgment with the professional judgment of others in a cooperative way that ensures multiple points of view are considered and multiple sources of knowledge contribute to the conclusion. This part of decision making is incorporated in the SDM system via the research behind the tools and the supervisor approval process. In addition, if the social worker disagrees with the recommendation of the tool, this opens the possibility of overriding the tool recommendation and indicates a need for further discussion with a supervisor. This provides a good check and balance in the decision making process. Common Core | SDM and Critical Thinking: Trainer's Guide | Version 1.21, 2011 17 Step 5: Ongoing Review As a final step in the process we highlight the continuous nature of information gathering, assessment and decision making. Situations involving children and families are rarely static. It is important to incorporate regular review of key factors and adjust actions as circumstances change. The decision may change as new information is received or as family members take steps to address factors. The SDM system and the court system have identified key points for reassessment, but social workers must remain aware of ongoing changes and adjust as needed to reflect new protective factors or new threats to safety. In conclusion, please note that SDM does not replace clinical skills. Effective use of the tools depends upon good interview and observation skills to conduct thorough assessments. It depends on the skill of the social worker to recognize unique conditions. Rather than replacing clinical judgment, SDM becomes a strong partner providing a research basis for critical decisions related to risk, and structure for increasing consistency and accuracy of other key decisions. Common Core | SDM and Critical Thinking: Trainer's Guide | Version 1.21, 2011 18 Minimum Sufficient Level of Care In order to effectively use the 5 step decision making process described above, social workers must be able to understand and assess the minimum sufficient level of care (MSLC). Correct application of the MSLC standard allows social workers to provide accurate assessments and keep children safe while also interfering as little as possible in people’s lives. The MSLC can be challenging to define. For the purposes of the California Common Core Curriculum for Child Welfare Social Workers, the definition is: The minimum sufficient level of care is the social standard for the minimum of parent behavior below which a home is inadequate for the care of a child. This definition successfully conveys the basic concept that the MSLC refers to the worst possible situation that still fits within the realm of acceptable care. The MSLC does not represent optimum care; on the contrary, it is one step away from unacceptable. The terms “minimum” and “sufficient” are crucial to this concept; the standard is related to the objective of keeping children safe and protected. The terms “minimum” and “sufficient” are used to explicitly differentiate from higher standards. The definition does not convey HOW the social worker establishes the MSLC standard. In order to understand this aspect of the MSLC concept, we have to consider the following: The MSLC is unique for each child and must address the child’s physical safety, emotional well-being and development, including: o Physical care (e.g., safety, protection, food, clothing , shelter, medical and dental care) o Emotional wellbeing (e.g., attachment between child and caregivers, sense of security) o Development (e.g., education, special help for children with disabilities) The MSLC is case specific. A variety of factors must be considered for each child and family, and there are no fixed criteria for assessing when a home falls below this minimum standard. This decision must be made by informed judgment and individual evaluation of each case. The MSLC must reflect contemporary social standards. Many social standards now are codified in law, e.g., definitions of child maltreatment, compulsory school attendance, and child labor. Others are mainly normative, e.g., expectations for how much work/chores children do in order to contribute to the family’s well being. Social standards have greatly changed over the last 100 and even 25-50 years so there is a wide range of accepted social standards. Common Core | SDM and Critical Thinking: Trainer's Guide | Version 1.21, 2011 19 The MSLC must reflect community standards. Ours is a pluralistic society. There are significant community differences present within a single town or region, reflecting differences related to culture, class, and ethnicity. The importance of community standards is explicitly identified in the Indian Child Welfare Act (ICWA) which mandates that the standards applied to a given Native American child reflect the tribe’s standards. The MSLC must remain consistent for the duration of the case. Once the MSLC is developed for a given child, it does not change throughout the life of the family’s case unless the needs of the child change (e.g., child develops a high risk health condition). When a child is in placement, the decision about reunification must be based on the same MSLC baseline as when the child was removed. It is important to avoid increasing the minimum expectations as the case progress and the parents gain more resources or the child’s foster home has a standard that differs from the MSLC. Increasing the standard over time interferes with the reunification plan and may lead to lengthy stays in foster care for children who could safely return home. Implementing the MSLC can be difficult. Establishing the MSLC involves exploration of values and must include application of broader social standards and legal standards in conjunction with community standards. Social workers must be aware that their own values and attitudes may differ from the family or community and they must be vigilant about separating their own individual values from the establishment and assessment of the MSLC. Different cultures have different interpretations of what constitutes the MSLC. Some steps to ensure fairness and equity might include: Developing the MSLC within a team that includes family members and community members. Documenting specific behavioral expectations for meeting the MSLC so the social worker and family will be able to assess progress along the way. Discussing the MSLC during case consultations with a supervisor or a multidisciplinary team. Taking additional training on how to apply MSLC to cases. Working in community partnerships to learn more about how different cultures view MSLC. Systematically considering what the standard was for removal and what the expectations are for return of the child, to assure that the standard is not changing over the life of the case. Although challenging to establish and employ, the MSLC is a key factor in child welfare assessments. It is a valuable tool for social workers for several reasons: It maintains the child’s right to safety and permanence while not ignoring the parents’ right to their children. It provides a practical way to interpret the reasonable efforts provision of PL 96-272. Common Core | SDM and Critical Thinking: Trainer's Guide | Version 1.21, 2011 20 It is possible for parents to reach. It provides a reference point for family members and social workers to mutually assess progress and reach decisions about safety. It protects (to some degree) from individual biases and value judgments. It discourages unnecessary removal from the family home. It discourages unnecessarily long placements in foster care. It keeps team members focused on what is the least detrimental alternative for the child. It is sensitive across cultures. Common Core | SDM and Critical Thinking: Trainer's Guide | Version 1.21, 2011 21 This page intentionally left blank. Common Core | SDM and Critical Thinking: Trainer's Guide | Version 1.21, 2011 22 Safety and Risk In order to effectively assess safety, risk and protective capacity we have to all be clear about the difference between safety (immediate safety compromise) and risk factors (likelihood of future maltreatment). We must also be aware that the SDM system has specific definitions of safety and risk as they are assessed by the safety and risk tools. First we’ll consider a broad definition of safety. Safety refers to: Currently dangerous family conditions that are severe in nature and specifically affect the child A situation which will almost certainly result in severe negative effects on the child (as opposed to something that could be a safety threat) Risk is broadly defined as the likelihood of future maltreatment. Risk includes: Family functioning General child well-being Family situations and behaviors that may need intervention but do not require immediate intervention All aspects of family life relevant to understanding the likelihood of maltreatment Because SDM tools are research based, they use more specific definitions of safety and risk. When assessing safety, SDM tools consider: Specific threats to a child’s imminent safety Evaluating family situations and behaviors that must be immediately managed and controlled in order for the child to remain in the home now When assessing risk, SDM tools consider: The likelihood of future maltreatment Decision making based on the likelihood of harm in the next 18-24 months Common Core | SDM and Critical Thinking: Trainer's Guide | Version 1.21, 2011 23 This page intentionally left blank. Common Core | SDM and Critical Thinking: Trainer's Guide | Version 1.21, 2011 24 Safety and Risk Worksheet A 2 month old has sleep apnea and needs to use an apnea monitor while sleeping. The family home has no electricity. Safety or Risk A 6 year old child is sent to school every day in a t-shirt and jeans in temperatures below 40 degrees. Safety or Risk The mother of a newborn has been diagnosed with schizoaffective disorder and has been hospitalized in the past for emotional problems. Safety or Risk A 3 month old in the home has a spiral femur fracture and the primary caregiver cannot explain how the injury occurred. Safety or Risk The home has two children age 4 and 6 and is dirty with clothes all over the floor, dirty dishes stacked in the kitchen and is infested with rats and roaches Safety or Risk The mother of 4 year old twins was arrested for DUI. The twins were in day care at the time of the mother’s arrest Safety or Risk There is a three year old child in a home with no water service. There is evidence of human waste in the home. Safety or Risk A four year old child reports that her stepfather comes in to her room at night and touches her private area. Safety or Risk A thirteen year old girl reports that her mother shouts at her and slaps her. She has no visible injuries. Safety or Risk A mother slaps a 2 month old baby on the face for crying and says the baby has to be slapped or it won’t be quiet. Safety or Risk An eight year old child is kept home from school several days a month to care for her infant sibling while the mother and father work. Safety or Risk A 3-year-old child has brown spots between his front teeth and has not been seen by a doctor or dentist in 12 months. Safety or Risk Common Core | SDM and Critical Thinking: Trainer's Guide | Version 1.21, 2011 25 This page intentionally left blank. Common Core | SDM and Critical Thinking: Trainer's Guide | Version 1.21, 2011 26 SDM Flow Chart Worksheet Tool? Tool? Tool? Is an inperson response needed? Can the child remain safely at home? What is the ongoing risk? Should we open a case? (Response Decision) (Removal / Placement Decision and Safety Plan) (Allegation Conclusion Decision and Case Opening Decision) Tool? What are the strengths and needs? Tool? In home cases Tool? Out of home cases (Service Needs Identification) What are the current safety threats and risks? How are visits? How much time is left? (Reunification Decision) Common Core | SDM and Critical Thinking: Trainer's Guide | Version 1.21, 2011 27 What is the family history and what progress has been made since the last assessment? (Case Closure Decision) This page intentionally left blank. Common Core | SDM and Critical Thinking: Trainer's Guide | Version 1.21, 2011 28 Protective Capacity Definition Action for Child Protection (2004) defines Protective Capacity as “the ability and willingness to utilize internal and external resources to mitigate or ameliorate the identified safety and risk concerns, and to support the on-going safety of the child.” Action for Child Protection (2004) further clarifies that protective capacity is “a specific quality that can be observed and understood to be part of the way a parent thinks, feels and acts that makes him or her protective.” Assessing parental and/or caregiver capacities allows the social worker to consider systematically the strengths of the parent(s) or caregiver(s), and how they might mitigate safety threats and risk factors. Cognitive, behavioral, and emotional factors are three such characteristics. 1) Cognitive characteristics as, “the specific intellect, knowledge, understanding and perception that contributes to protective vigilance.” 2) Behavioral characteristics as “specific action, activity and performance that is consistent with and results in parenting and protective vigilance.” 3) Emotional characteristics as “specific feelings, attitudes and identification with the child and motivation that result in parenting and protective vigilance” Cognitive Characteristics Questions to consider include: Is the caregiver oriented to time, place and space? (Reality orientation) Does the caregiver have an accurate perception of the child? Does the caregiver view the child in an “integrated” manner (i.e. seeing the child as having strengths and weaknesses), or do they see the child as “all good or all bad?” Does the caregiver have the ability to recognize the child’s developmental needs, or if the child has “special needs?” Does the caregiver accurately process the external world stimuli, or is perception distorted (i.e., a battered woman who believes she deserves to be beaten because of something she has done)? Does the caregiver understand the role of caregiver is to provide protection to the child? Does the caregiver have the intellectual ability to understand what is needed to raise and protect a child? Common Core | SDM and Critical Thinking: Trainer's Guide | Version 1.21, 2011 29 Does the caregiver accurately assess potential threats to the child? Behavioral characteristics Questions to consider include: Does the caregiver have the physical capacity and energy to care for the child? If the caregiver has any disabilities (i.e., blindness, deafness, paraplegia, chronic illness), how has the caregiver addressed the disability in parenting the child? Has the caregiver acknowledged and shown action to get the needed supports to effectively parent and protect the child? Does the caregiver demonstrate activities that indicate putting aside one’s own needs in favor of the child’s needs? Does the caregiver demonstrate adaptability in a changing environment or during a crisis? Does the caregiver demonstrate appropriate assertiveness and responsiveness to the child? Does the caregiver demonstrate actions to protect the child? Does the caregiver demonstrate impulse control? Does the caregiver have a history of protecting the child given any threats to safety of the child? Emotional characteristics Questions to consider include: Does the caregiver have an emotional bond to the child? Is there a reciprocal connectedness between the caregiver and the child? Is there a positive connection to the child? Does the caregiver love the child? Have empathy for the child when the child is hurt or afraid? Does the caregiver have the ability to be flexible under stress? Can the caregiver manage adversity? Does the caregiver have the ability to control emotions? If emotionally overwhelmed does the caregiver reach out to others, or expected the child to meet the caregiver’s emotional needs? Does the caregiver consistently meet their own emotional needs via other adults, services? Actions When assessing the protective capacity of the caregiver, actions speak louder than words. A statement by the caregiver that he/she has the capacity/will to protect should be respected, but observations of this capacity are very important, as they may have serious consequences for the child. When interviewing the caregiver, it is important to include questions that provide answers and observations that support an assessment of behavioral, cognitive and emotional functioning. Suggested questions and observations include: Common Core | SDM and Critical Thinking: Trainer's Guide | Version 1.21, 2011 30 A history of behavioral responses to crises is a good indicator of what may likely happen. Does the caregiver “lose control?” Does the caregiver take action to solve the crisis? Does the caregiver believe crises are to be avoided at all costs, and cannot problem solve when in the middle of a crisis, even with supports? Watch for caregiver’s reactions during a crisis. This often spontaneous behavior will provide insight into how a caregiver feels, thinks and acts when they themselves are threatened. Does the caregiver become immobile to the point of inaction (failure to protect)? Does the caregiver move to protect him/herself rather than the child? Does the caregiver actively blame the child for the crisis? Recognition of caregiver anger or “righteous indignation” at first is appropriate and natural. How a caregiver acts beyond the anger is the important key. Once the initial shock and emotional reaction subsides, does the caregiver blame everyone else for the “interference?” Can the caregiver recognize the protective and safety issues? What are the dynamics of the relationship of multiple caregivers? Does the relationship involve domestic violence? What is the nature and length of the domestic violence? What efforts have been made by the victim to protect the child? Does the victim align with the batterer? Does the caregiver actively engage in a plan to protect the child from further harm? Is the plan workable? Does the plan have action steps that the caregiver has made? Does the caregiver demonstrate actions that are consistent with verbal intent or is it contradictory? Information from Other Sources Detailed interviewing and information gathering from other sources is critical for an accurate assessment. Suggestions for additional activities include: What do others say about the caregiver’s parenting and ability to protect the child/ What do others say about the caregiver’s history of protecting the child? What is the documented history that indicates the caregiver’s actions toward protecting the child? Assessing Environmental Protective Capacities While the assessment of the caregiver’s protective capacities is critical, an assessment of environmental capacities may also mitigate the safety concerns/risk of harm to a child. Below are several categories of environmental protective capacities, along with questions and considerations that may be considered when assessing them. Formal family/kinship relationships that contribute to the protection of the child o What are the formal kinships within a family? (Grandparents, aunts, uncles, siblings, stepparents and their families, half siblings, gay partners raising children, etc.) Informal family/kinship relationships Common Core | SDM and Critical Thinking: Trainer's Guide | Version 1.21, 2011 31 o What are the informal relationships? (friends of the family, godparents, tribal connections, “pseudo” relatives, mentors, divorced step parent who maintains parental relationship with the child, etc.) Formal agency supports o What are the agencies that have been or are currently involved with the family? Previous agency involvement may have been seen as beneficial and can be called upon again (i.e. drug treatment, children’s hospital, Regional Center, non –profit agencies, food banks, schools, employment training, parenting classes, DV programs, etc.) Informal community supports o What are the community supports that may or may not be readily apparent? (local parent support groups, informal mentors, neighbors, neighborhood organizations, babysitting clubs, library reading times, etc.) Financial supports o Employment, unemployment, disability, retirement benefits o TANF, GA/GR, SSI o Scholarships, grants Spiritual or congregational/ministerial supports o Churches, ministries, prayer groups, synagogues, temples, mosques o Spiritual leaders within a faith Native Americans (the tribe) o Is the family a member of a tribe locally, or elsewhere? Are there ICWA agencies that can provide services? (Elders within a tribe, tribal chairpersons, liaisons to the tribes, Indian health agencies) With all families, it is important to consider the parents’ behavior in light of cultural considerations. Is our assessment of a parent’s behavior based on our own cultural beliefs or are we taking into account the cultural appropriate customs, traditions, history, etc. Concrete needs being met such as food, clothing, shelter o Low income housing, food banks, clothing stores, emergency shelters, subsidized housing. It is the interplay of safety, risk and protective capacity (both internal and external elements) that constitutes the elements of the assessment process. Common Core | SDM and Critical Thinking: Trainer's Guide | Version 1.21, 2011 32 Family Friendly Interview Sample This interview sample involves a mother, Serena, and a social worker discussing an injury to Serena’s infant daughter, Santana. The concern is that Santana has a fractured leg and there is no clear explanation for the injury. The social worker must ask questions about the specific incident, but is also gathering information about all the safety threat factors. The interview is adapted from interview samples in Turnell, A., and Edwards. S. (1999). Signs of Safety. Serena: I don’t have any answers about what happened. I love my baby and I don’t want you to take her away. Social Worker: Well, I am hoping we can discuss a few things, including what may have happened to Santana and what your life together is like so that I can get a clear picture of your family. I hope that you will work with me to get an idea of Santana’s safety with you. I want to make sure you know that I can’t predict what will happen following our discussion, but I may ask you to help me make a plan for Santana’s safety. Serena: I can keep her safe. I have been taking care of her by myself her whole life. She has always been safe. Social Worker: Let me start this conversation by saying I see for myself and have heard from the nurses and doctors here that you and Santana have a strong relationship. Her weight is good and she looks to you for comfort. Those things tell us that you are working hard to take good care of your baby. Serena: I took a class about baby care, so I know about feeding and changing her. Social Worker: That’s great. I know the doctors here have said she is clean and her weight is good. Let’s talk about the injury to Santana’s leg. Do you know what type of injury she has? Serena: They told me it was a spiral fracture, but I don’t know what that means. I don’t think it is all that serious because she doesn’t have a bruise and since she doesn’t walk yet it probably doesn’t hurt her very much. Common Core | SDM and Critical Thinking: Trainer's Guide | Version 1.21, 2011 33 Social Worker: Well a fracture means a broken bone and a spiral fracture means the bone broke during a twisting movement. For people who don’t walk, like Santana, this almost always means some twisting was done to the leg. If you think of a stick being twisted until it breaks, you can imagine the way a spiral fracture happens. Serena: Oh! That sounds like it would hurt a lot! Poor Santana! I really didn’t understand what they meant. I haven’t ever twisted her leg, though. Social Worker: Is there anyone else who takes care of her? Serena: Well, sister and my cousin, but they wouldn’t hurt her. They love her. Social Worker: Is it possible that someone twisted her leg not knowing it could hurt her in this way? Serena: I guess it is possible. I’m not sure. Social Worker: OK. I think we will have to talk to them about it. Would that be OK? Serena: I guess so. Social Worker: Now, I have some questions about other topics that might seem a little unrelated, but we need to ask about some other things that could be affecting your family. We ask these questions of all the families we interview. Can I go through these questions with you? Serena: OK. Social Worker: Do you have problems with alcohol or drugs? Serena: No. I saw what crank did to my sister and I have stayed away from drugs. Social Worker: OK. Is there any domestic violence involving you or anyone else in your house? Serena: I guess my sister has had some trouble with her boyfriend a few times, but she wouldn’t let that happen around Santana. I just don’t think my family would ever let anything happen to my baby. Social Worker: OK. Let’s keep talking about it and let’s bring the family into the conversation so I can get a clear picture of the whole support system and how everyone works together. Common Core | SDM and Critical Thinking: Trainer's Guide | Version 1.21, 2011 34