Ossification of the Petrotympanic Fissure
advertisement

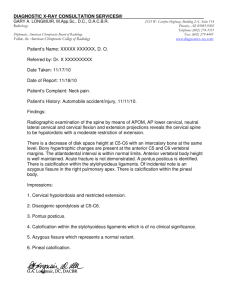
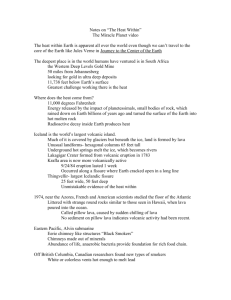
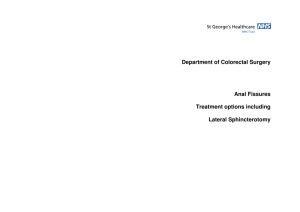
• PHYSIOLOGY Ossification of the Petrotympanic Fissure: Morphological Analysis and Clinical Implications Joào Carlos Castro Monteiro, D.D.S.; Jussara Peixoto Ennes, D.D.S., Ph.D.; José Roberto Zorzatto, Ph.D. 0886-9634/2904284$05.00/0, THE JOURNAL OF CRANIOMANDIBUUVR PRACTICE, Copyright ©2011 by CHROMA, Inc. Manuscript received May 10, 2010; revised manuscript received Juiy 30, 2010; accepted July 31, 2010 Address for correspondence; Dr. Joao C.C. Monteiro SQN215, BiocoG, Apt. 402 Brasiiia DF, Brazil 70.874-070 E-mail; jccmdf@hotmaii.com ABSTRACT: The petrotympanic fissure, a narrow slit in the temporal bone, aliows the temporomandibuiar joint (TMJ) and the middle ear to communicate. Both the chorda tympani and the ligament cross the fissure between the posterior region of the joint disk and the maileolar ossicle. The parasympathetic fibers of the chorda tympani spread into the major saiivary giands and are responsible for the taste sensibiiity on the anterior two-thirds of the tongue. After chronological identification of 30 human skulls, petrotympanic fissures were macroscopically and stereomicroscopicaliy analyzed for the presence and disposition of ossification areas. Digitaiized images were analyzed using computer program UTHSCSA ImageTooi 3.0 (developed by the Department of Dental Diagnostic Science at The University of Texas Health Science Center, San Antonio, Texas). The total extension of the fissures and ossification areas was measured. The macroscopic analysis did not constitute an appropriated method for this evaluation and the ossification of the fissures increased with aging, suggesting its influence on the causes of otalgia in cases of TMJ dysfunction. T he petrotympanic fissure, located at the mandibular fossa of the temporal bone, is crossed by two ligaments connecting the temporomandibular joint (TMJ) to the middle ear, both adhered individually to the collum mallei. The discomalleolar ligament, firstly described by Pinto', extends from the retrodiscal region of the articular capsule to the malleus ossicle and the anterior ligament of the malleus, which becomes continuous to the sphenomandibular ligament.- These ligaments were supposed to be related with the otological symptoms because of the involvement of the middle ear determined by the anterior displacement of the disk or by the excessive mandibular movements, which would determine the excessive traction of the discomalleolar ligament.•'•'' However, this consequent traction of the middle ear ossicles has been questioned, since it is admitted that the fissure may have limiting dimensions where the intrafissural arrangement of the soft tissues would not allow the transmission of forces.' Cases in which the material injected for arthroscopy of the TMJ would have determined otological complica- Dr. Joào Carlos Castro Monteiro received his D.D.S. degree in 2001 from the University of Brasilia (UnB). Brazil and his certificate of conclusion of the Residency Progratn in Oral Surgery at the University of Mato Grosso do Sul (UFMS), Brazil, in 2008. He became a volunteer professor of oral surgery at the University of Brasilia in 2009. At the time of this mcmti.script submission, he was working to finish the Specialization Program of Implantology at the University of Sao Leopoldo Mandic, Brazil. He works as an oral surgeon at the Regional Hospital of Planattina and at the College Hospital of the University of Brasilia. 284 MONTEIRO ET AL. OSSIFICATION OF THE PETROTYMPANIC FISSURE tions, like otalgia and tympanum perforation, suggest that the way of communication between the articulation and the middle ear would he evident.*" The calcification process of the sutures of calvarium occurs in the second decade of life^ from both the endocranial and ectocranial* surfaces. Likewi.se, the calcification process of the petrotympanic fissures could occur in the same sequence and direction; however, the description of the ossification pattern in this fissure remains inconclusive. The clinical implications of the ossification pattern of the petrotympanic suture can be better understood in light of morphological descriptive knowledge. The aim of this study is to morphologically characterize the calcification in the petrotympanic fissure through three observations: naked-eye macroscopic observation, stereomicroscopic observation, and measurements made from digital images. the length of the calcified regions using the ImageTool program (University of Texas Science Center in Santo Antonio, TX) (Figure 1). The petrotympanic fissures were photographed in full-length under lOx magnification, with liO dpi vertical and horizontal resolutions. Materials and Methods Thirty human skulls were studied for the classification of chronological age, according to the degree of calcification of the latero-anterior sutures, through the ectocranial surface, as described by Meindl; Lovejoy.'* Sutures on the right side were observed, (Table 1). Left and right petrotympanic fissures were analyzed macroscopically, stereo-microscopically, and also in digital images captured in a Leica MZ 125 stereomicroscope with a Leica DC 300F system of image capture (Leica Microsystems, Heerbrugg, Switzerland). Millimeter patterns were used to create proportionality in the measurements of the total length of petrotympanic fissures and Table 1 Sum of Calcified Suture Marks for Each Skull Studied to DeterrTiine the Presumed Chronological Age at Death* Sum of calcified suture marks 0 (no calcification) Presumed chronological age under 32 1 2 3 ,4, 5, 32 36 41 6 7,8 43 45 9, 10 51 11, 12, 13, 14 56 15 (total calcification) over 56 "Adapted from Meindl & Lovejoy (1985) OCTOBER 2011, VOL, 29, NO, 4 Figure I Digitalized itnage of the right tnandihular fossa of skull no, 28. with identification tag and pattein in mm. By macroscopic evaluation, the areas of possible calcification were identified and recorded. Stereomicroscopically, using a I Ox magnification, the petrotympanic fissures were observed along their full length in the latero-medial direction. The calcification regions were identified and recorded in a drawing, based on their anatomy (Figure 2). The open-to-discussion regions were assessed with 15, 20, and 30x magnifications, respectively. In some cases, these regions have still been analyzed with gradable variations of light intensity caused by the adjustment of the stereomicro.scope so that deeper regions in the fissure could clearly be identified. The values of the total length of the fissures and each calcified region yielded, in percentage, the calcification index for each fissure. In order to investigate whether there were differences between the fissure length and the percentage of calcification according to age, the skulls were separated into two groups. Group I was comprised of 18 individuals aged 41 years old or younger and Group II, 12 individuals who were older than 41. The age of 41 years was chosen based upon the number of individuals needed in each group to give an adequate statistical analysis of the results. The statistical analysis of the results, in order to check for differences in the parameters of both groups evaluated, considered the level of significance a=0.05%, i.e., the difference between the medians of the two groups was THE JOURNAL OF CRANIOMANDIBULAR PRACTICE 285 OSSIFICATION OF THE PETROTYMPANIC FISSURE MONTEIRO ET AL. Figure 2 Schematic drawings of individual records of skulls nos. 88 (left) and 93 (right), representing the petrotympanic fissures observed and evaluated using a stereoniicroscope. Note the observations made in regard to the anatomical length of the fissures and the presence or absence of calcified considered statistically significant when p (probability of signiflcance) of the test was lower than the level of significance of 5%. Results The macroscopic analysis of the petrotympanic fissures revealed suggestive calcification areas in 27 fissures (45%). From the total of fissures that supposedly presented a calcification area, 13 were relative to the right side and 14 to the left side of the skulls. The stereomicroscopic analysis of the fissures showed calcification areas or bridges that were superficial and, in some cases, deep in 40 petrotympanic fissures, i.e., in 66.6% of the total (Figures 3-7). Among these, 18 were relative to the right side of the skulls and 22 to the left. In most cases, the deep calcification areas (Figure 7) could only be observed under stereomicroscope when light intensity was increased. (Figures 4 and 5). The localization of the calcification areas was not regular when considering the total length of the diverse flssures and its division into medial and lateral regions, randomly occurring along the total length of the petrotympanic fissures. A Wilcoxon test for two-related samples, with p=0.229, showed no statistically significant difference for fissure length in relation to the sides. Likewise, p=0.225 showed that the difference in calcification percentages was not statistically significant for either the right or left sides (Table 2). The Mann-Whitney test, for independent samples, with p=0.4588 for the right side and p^O.2899 for the left, showed that there were no statistically significant 286 THE JOURNAL OF CRANIOMANDIBULAR PRACTICE Figure 3 Right petrotympanic fissure of skull no. 88. Pattern photograph for measuring total length of ftssure in mm. Note the calcified (white arrows) and the noncalcifted (black arrows). differences in median lengths of the fissures between Group I and Group II for either the right or left sides (Table 3). The Mann-Whitney test, for independent samples, with p=0.0262, showed that, for the right side of the skull, there is statistically significant difference in the median percentages of fissure calcifications of Groups 1 and II, of different chronological ages; the same observation holds for the left side, with p=0.()277 (Table 4). Discussion The analysis of the 3-dimensional aspects of the anatomical structures demands a suitable device.'" The OCTOBER 2011, V O L 29, NO. 4 MONTEIRO ET AL. OSSIFICATION OF THE PETROTYMPANIC FISSURE ir Figure 4 Right fissure of skull no. 88 with increased luminous intensity. Note the contrast of the calcified (white arrows) and noncalcified (black arrows). tr Figure 6 Left petrotympanic fissure of skull no. 88. Pattern photograph for measuring total length of the fissure in mm. Note the superficial calcification areas (white arrows). ÏÏ ÏÏ Figure 5 Right fissure of skull no. 88 with the same increase in luminous intensity, but from another angle to confirm the central calcification area (white arrows). Figure 7 Left fissure of skull no. 88 with increased luminous intensity Note the contrast of the superficial (white arrows) and the deep (black arrows) calcified areas. analysis of the petrotympanic fissures with a stereomicroscope allowed for the identification of a larger number of calcification areas in the fissures, which could not be identified with the naked eye (Figures 3-7). The macroscopic analysis of the fissures is more reliable in the cases in which a fissure is totally open and when it is totally or practically calcified, which was not seen. Ennes and Consolaro'" observed the direction of the calcification of the middle palatine suture, which was postero-anterior, and related it with the anatomical disposition of the horizontal plane of the palate. The latter, with no condition to transmit forces to the head bone complex, would respond to the convergence of forces with the apposition of the bone, in a way similar to other bone braces, such as the glabella or the menton protuberance; however, the same was not seen in relation to the calcification of the petrotympanic fissure. The calcification areas or bridges were randomly scattered along the length of these fissures. Some factors could contribute to the absence of standardization, such as: longer distances between the bone surfaces delimiting the petrotympanic fissures; more complexity of tissues making up the anatomical structures crossing it; the physiology of these tissues; and the balance resulting from force distribution. The fissures presented similar length and standard ossification on both sides. The latter could be explained by the physiological patterns of the TMJ. Since they are synergic articulations, both sides move simultaneously,' OCTOBER 2011, VOL. 29, NO. 4 THE JOURNAL OF CRANIOMANDIBULAR PRACTICE 287 MONTEIRO ET A L OSSIFICATION OF THE PETROTYMPANIC FISSURE Table 2 Results of the Statistical Descriptive Analysis in Relation to the Fissure Length (in mm), and the Percentage of Calcification, According to Laterally Descriptive Fissure lenqth (mm) Percentaae calcification Right Left Right Left statistics Mean 14.01 13.49 24.41 28.74 Median 24.70 31.08 14.18 13.25 2.34 1.92 24.78 25.26 Std. Dev. Minimum 8.90 0 0 9.53 16.19 82.70 77.80 Maximum 17.93 30 Count 30 30 30 p value 0.229 0.225 Table 3 Results of the Statistical Descriptive Analysis in Relation to the Fissure Length (in mm), and the Percentage of Calcification, According to Age Descriptive Fissure lenqth (mm) - riqht side Fissure lenath (mm) - left side statistics <41 years >41 years <41 years >41 years Mean 14.30 13.59 13.82 13.01 Median 14.21 13.54 14.34 12.98 2.07 1.77 2.12 Std. Dev. 2.73 Minimum 9.53 9.81 10.14 8.90 Maximum 17.93 17.90 16.19 16.06 Count 18 12 18 12 p value 0.4588 0.2899 Table 4 Results of the Statistical Descriptive Analysis of the Percentage of Fissure Calcification, According to Age Descriptive Calcification % on riaht side Calcification % on left side statistics >41 years <41 years >41 years <41 years Mean 15.88 37.21 20.09 41.72 Median 0 40.18 18.78 43.34 Std. Dev. 22.94 22.54 20.19 27.31 Minimum 0 0 0 0 Maximum 66.68 82.70 61.93 77.80 12 18 12 Count 18 p value 288 0.0262 THE JOURNAL OF CRANIOMANDIBULAR PRACTICE 0.0277 OCTOBER 2011, VOL. 29, NO. 4 MONTEIRO ET AL. OSSIFICATION OF THE PETROTYMPANIC FISSURE stimulating the osteogenic membranes symmetrically. The increase of calcification percentages in the petrotympanic fissures was observed to be associated with an increase in chronological age. This is illustrated graphically through the increase of both the average and the median for calcification percentages (Figure 8). The calcification process of anatomical accidents due to aging was previously observed in other studies.'''- the possible movement of ear ossicles would depend on the degree of closure of the petrotympanic fissure during the development and on the points of adhesion of the ligament in the fissure borders. In cases of "big and broad" fissures and/or "ligaments badly adhered to the walls of these fissures," the parafunctional mandibular pathways seen in some sufferers of TMD could result in the traction and movement of the malleus, resulting in otological PERCENTAGES OF CALCIFICATION 37.21 41.72 40.18 43.34 • Average • Median 15.88 0.00 G1D G2D G1E G2E Figure 8 Average and median of the percentages of fissure calcification for Group 1 on the right (GID) and left side (G2D) and for Group 2 on the right (GlE) and left side (G2E) The ossification of the fissure may indicate the discontinuity of the ligaments of the TMJ structure and the tympanic cavity. This observation may be associated with the hypotheses'-*'"• used to try to explain the clinical implications of conditions such as otalgia in cases of temporomandibular disorders (TMD).""' Kim, et al.." reported that the movement of the malleus was observed during the traction of its anterior ligament. This observation could strengthen the hypothesis that associates traction of the malleus by the discomalleolar ligament with the origin of otalgia in TMD. since both ligaments would be adhered to each other."* Authors like Komori, et al.,- Eckerdal,'^ Coleman,'''and Ögütcen-Toller,-" however, claim that there is no evidence that the traction of the discomalleolar ligament could cause the movement in the ossicle chain of the middle ear in adults. Rodríguez-Vásquez, et al.,'* suggests that the traction of the discomalleolar ligament and OCTOBER 2011, VOL. 29, NO. 4 symptomatology. Theoretically, this non-physiological movement of the malleus could inflict any traumatic injury to the tympanic membrane or to the chain of auditory ossicles, since all these structures are closely related.-' The patients could relate earache because the tympanic membrane and the mucous membrane, which constitute the structures of the middle ear, are extensively innervated.-' This could be a possible reason why not all TMD sufferers present with otalgia.'* With the calcification of the petrotympanic fissure in the later phases of life, the communication between the middle ear and the temporomandibular articulation would not exist. TMD sufferers with otologic symptomatology should report an alleviation of these symptoms with age, since because the fissure is calcified, there would not be any other way for the tensional forces towards the middle ear ossicles to propagate. It is worth noting that the average age of the sufferers corresponds to the age of adults. THE JOURNAL OF CRANIOMANDIBULAR PRACTICE 289 OSSIFICATION OF THE PETROTYMPANIC FISSURE but not in elderly subjects, according to some studies.""" In cases where it is not seen, other theories should explain the origin of these symptoms.'^•'•* MONTEIRO ET AL. 10, 11, 12, Conclusions The macroscopic or naked-eye analysis of the calcification of petrotympanic sutures was unreliable. The stereomicroscope showed the following: an increase in calcification areas or bridges in the petrotympanic fissures related with chronological aging; the inexistence of a relationship between calcification and anatomical position in both sides of the skull; and the nonexistence of alteration in petrotympanic fissure length related to aging. These observations allowed the inference that the continuous calcification process of the petrotympanic fissures could be associated with the presence/absence of otalgia in TMD sufferers. Further studies, however, would be necessary, especially longitudinal clinical studies involving elderly patients to investigate the symptomatology. From the data collected, the diverse theories and/or hypotheses could be related or discarded so as to enable the development of better treatment options for these patients. References Pinto OF: A new structure related to the temporomandibular joint and middle eux. J Prosthet Den 1962; l2(n:95-103, Komori E. Sugisaki M. Tanabe H, Katoh S: Discomalleolar ligament in the adult human, J Craniomandih Pracl 1986; 4(4):3CIO-3O5, Ioannides CA. Hoogland GA; The discomalleolar ligament; a possible cause of subjective hearing loss in patients with temporomandibular joint dysfunction, V Aífl.ri//o/aí-Swr^ 1983; 11;227-23I. Cheynet F. Guyot L. Richard O. Layoun W. Gola R; Discomalleolar and malleomandibular ligaments; anatomical study and clinical applications, 5urg Rflí/ioMnaí 2003; 25; 152-157, Eckerdal O; The petrotympanic tissure; a link connecting the tympanic cavity and Ihe temporomandibular joint, J Craniomandih Pract 1991; 9( I ): 15-22, Schickinger B. Gstoettner W. Cemy C. Komfehl J; Variant petrotympanic fissure as possible cause of an otologic complication during TMJ anhroscopy, J Oral Mavillofac Surg 1998; 27; 17-19, DuBrul EL; Sicher and DuBrul's oral anatomy. St Louis & Tokyo; Lshiyaku Euroamerica Inc. 1988, Todd TW. Lyon Jr DW; Endix-ranial suture closure. Part I, Adult males of white stock. Am J Pins Anihropol 1924; 7;325-384, Meindl RS. Lovejoy CO; Ectocranial suture closure; a revised method for the determination of skeletal age at death based on the lateral-anterior sutures. Am J Phys Anthropol 1985; 68;57-66, 290 THE JOURNAL OF CRANIOMANDIBULAR PRACTICE 13, 14, 15, 16, 17, 18, 19, 20, 21, Ennes J. Consolaro A; Sutura palatina mediana; avaliaçâo do grau de ossificaçào em crânios humanos, R Dental Press Onodon Orlop Facial 2004; 9(5);64-73, Ashley-Montagu MF; Aging of the skull. Am J Phys Anihropol 1938; 3;35575, Manzanares MC. Goret-Nicaise M. Dhem A; Metopie suture closure in the human skull, 7/Imi; 1988; I6I;2O3-2I5, Ash CM. Pinto OF; The TMJ and the middle ear; structural and functional correlates for aural symptoms associated with temporomandibular joint dysfunction, hit J Prosthodoni 1991;4(l);5l-57, Manni A. Brunori P. Giuliani M. Modoni M. Bizzi G; Oto-vestibular symptoms in patients with temporomandibular joint dysfunction, Electromyographic study, Minen'a Sionuitol 1996; 45(l);l-7. Pascoal MIN. Rapop<5rt A. Chagas JFS. Pascoal MBN. Costa CC. Magna LA; Prevalência dos sintomas otológicos na desordem temporomandibular; estudo de 126 ca,sos. Rev Bras Olorrinolaring 2001 ; 67(5);627-633, Tuz HH. Onder EM. Kisnisci RS; Prevalence of otologic complaints in patients with temporomandibular disorder. Am J Orthod Denlofac Orlhop 2003; 123(6);620-623, Kim HJ. Jung HS. Kwak HH. Shim KS. Hu KS. Park HD, Park HW, Chung IH; The discomalieolar ligament and the anterior ligament of malleus; an anatomic study in human adults and fetuses. Surg Radiol Anat 2004; 26;3945, Rodríguez-Vá.squez JF. Merida-Velasco JR. Merida-Vela,sco JA. JiménezCollado J; Anatomical considerations on the discomalleolar ligament, JAnat 1998; 192;617-621, Coleman RD; Temporomandibular joint; relation of the retrodiscal zone to Meckel's cartilage and lateral pterygoid muselé. J Dent Res 1970; 49;626630 OgUtcen-Toller M; The morphogenesis of the human di.scomalleolar and sphenomandibular ligaments, J Cranioma.xiltofac Surg 1995; 23;42-46, Clemente CD; Gray's anatomv. Philadelphia; Lea & Febiger. 1985, Dr. Jussara Peixoto Ennes is an adjunct professor in human anatomy at the University of Mato Grosso do Sut ( UFMS), Brazil. She received her D.D.S. degree in 1985 from the School of Dentistry in UFMS. Brazil, a Master's degree in odontology ft otn the School of Dentistry of the University of Sao Paulo (USP). Brazil in 1999, atid a Doctorate in oral pathology from the School of Dentistry of Bauru in USP, Brazil in 2002. Dr. Ennes's specialties include: etidodontics (University of Sao Paulo — USP, 1988) and Morpho-physiology (UFMS, 1994). Her teaching experience iticludes: human attatomy, neuroanatomy, dental anatomy, and her particular area of interest is in odontogenesis research, including craniofacial anatomy and dental anomalies. Dr. José Roberto Zorzatto is an associate professor in biostatistics at the Institute of Cotnputation at the University of Mato Grosso do Sut (UFMS). Brazil. He graduated in mathematics at the University Julio de Mesquita Filho, Sao Paulo, in 1978. He received his Master's degree in statistics from the University of Campinas (Unicatnp), SP, Brazil anda Ph.D. degree in electrical engineering at Unicatnp. The main focus of his scientific work is on biostatistics atid experiment platining. He did his thesis on Probability Models for tropical forests. OCTOBER 2011, VOL, 29, NO. 4 Copyright of CRANIO: The Journal of Craniomandibular Practice is the property of Chroma Incorporated and its content may not be copied or emailed to multiple sites or posted to a listserv without the copyright holder's express written permission. However, users may print, download, or email articles for individual use.