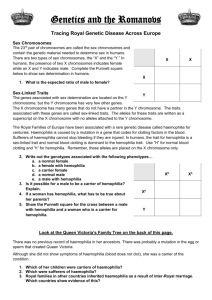
Canadian Social Worker and Nurse Perspectives on the Haemophilia Experiences, Results and Opportunities (HERO) Study Results From Canada Introduction The Haemophilia Experiences, Results and Opportunities (HERO) initiative aimed to increase the understanding of psychosocial issues impacting people with haemophilia by collaborating with an International Advisory Board that included healthcare providers (HCPs), patients, and caregivers. Ten countries participated between June 2011 and February 2012 (Figure 1). 2. A. Iorio McMaster University Hamilton, ON, Canada HERO results: sex life Social Workers Haemophilia Nurses Key Key insights insights and and unmet unmet needs needs Proposed Proposedsolutions solutions Of the 29 Canadian adults with haemophilia who responded on employment, 15 (52%) were employed full-time, employed part-time, or self-employed. – Overall, 4 patients (14%) reported long-term disability. Of the 39 Canadian parents of children with haemophilia who responded on employment, 35 (90%) were employed full-time, employed part-time, or were self-employed. HERO results: pain HCPs need training on how to engage and take cues from patients and parents. HCPs need to discuss sex life more, and there is a need for professional support on how to approach the topic (eg, a timeline for parents, brochure). USA UK Spain Italy Germany Sex life Possibility to approach the topic more appropriately with patients (eg, give the parent a brochure with timeline for talking to kids). Handouts to start conversations. Educational seminars on strategies for HCP seminars. Website with patient testimonials. – Create business cards linking to the website. Youth group discussions through local haemophilia chapters. Information nights through local haemophilia chapters. HCPs should ask about sex life at every opportunity. There is still discrimination at work and school; this has a negative impact on patients and parents. Social workers question whether patients are underperforming (eg, salary) in relation to education. Social workers wonder whether they are doing a good enough job educating about the future and advice for transition (eg, should they recommend desk jobs?). Capture the facts (what’s possible or not with respect to jobs). Vocational support programs need to start early. Prophylaxis research (is there a link between adherence and good job choices?). Clarify Haemophilia Treatment Centre role in advocacy. Develop a literature review about pain assessment tools for haemophilia. Teach parents how to assess pain (develop tools for this). Develop an application for assessing and managing haemophilia-specific pain. Offer pain intervention (pain teams specialist clinic). Develop distraction tool kits. Teach ways to cope (eg, pharmacologic, alternative, relaxation methods). To describe social worker and haemophilia nurse perspectives on the Canadian HERO results. Methods Surveys were developed for adults with haemophilia (≥18 years) or parents of children (<18 years) with haemophilia either currently receiving factor replacement or with spontaneous joint bleeding in the past 12 months. Advisory board meetings with Canadian social workers and nurses were held to discuss the HERO results in January and April 2013, respectively. Results Overall, 30 adults and 41 parents from Canada responded to the HERO survey. – Adults with haemophilia from Canada reported a median age of 38 years. – Parents of children with haemophilia reported a median age of 37 years. Independently, both social workers and nurses identified the same key psychosocial issues. – These included issues with sex life, employment, and pain (Figure 2). Employment Social workers wonder what the impact is on parent’s (both mother and father) career. Explore vocational issues and increase Haemophilia Treatment Centre awareness of the issues. Social workers wonder how they can do a better job before patients start work (eg, disclosure, their rights). In Canada, there is a higher percentage of patients reporting suffering from pain compared to the US and total HERO population. – Social workers wonder whether pain recognition is “better” in Canada compared to other countries? There is a lack of chronic pain care/service. Pain There is a lack of acute pain treatment in children. There needs to be an increase in sensitivity to pain issues. Presented at NHF’s 65th Annual Meeting; Anaheim, California; October 3-5, 2013. Overall, 9/30 (30%) adults with haemophilia reported that in the past 4 weeks, pain had interfered with their daily life extremely or quite a lot; 8/30 (27%) reported moderate interference, 13/30 (43%) reported a little or no interference. – Of 27 adults, 9 (33%) reported pain all the time and 13 (48%) reported pain all the time that gets worse when they have a bleed; 3 (11%) reported pain only when a bleed occurs and 2 (7%) did not know when pain occurs. Items that the nurses identified they would do differently after seeing the HERO results Objective Of the 18 Canadian adults with haemophilia who responded about their sex life, 9 (50%) reported that haemophilia had affected the quality of their sex life. HERO results: employment France China Canada Argentina Kiddies Health Care Inc. Toronto, ON, Canada Figure 2 Top 3 psychosocial issues independently identified by Canadian social workers and haemophilia nurses were sex life, employment, and pain Figure 1 HERO participants Algeria 1. A. M. Stain Add more items to a clinic checklist, such as asking patients with haemophilia if they see a family physician and the last time they saw the physician or nurse. Take a closer look at obesity in patients with haemophilia and assess whether a dietician is needed. – In addition, explore the possibility of creating a patient discussion group to discuss healthy eating practices. Work more closely with the haemophilia social worker. Work collaboratively with the Canadian Hemophilia Society to develop topics of interest for patients and families. Conclusions HERO provided key insights into psychosocial issues facing Canadian adults with haemophilia and Canadian parents of children with haemophilia. At independent advisory board meetings, both social workers and nurses identified the same key psychosocial issues impacting patients and parents. Nurses and social workers provided strategies that could help improve the lives of both patients and parents. Nurses and social workers may approach challenges differently. But when they work to their strengths, they better understand the key issues and work together as a team to provide comprehensive care to patients and their caregivers.