ocular rupture associated with lens dislocation to the
advertisement

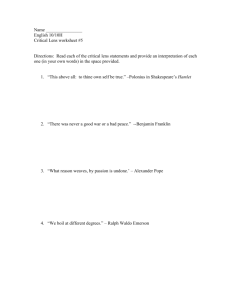
SHORT COMMUNICATION ARCH SOC ESP OFTALMOL 2007; 82: 641-644 OCULAR RUPTURE ASSOCIATED WITH LENS DISLOCATION TO THE SUBCONJUNCTIVAL SPACE ESTALLIDO OCULAR CON LUXACIÓN DE CRISTALINO AL ESPACIO SUBCONJUNTIVAL SANTOS-BUESO E1, SAENZ-FRANCÉS F2, DÍAZ-VALLE D1, TROYANO J2, LÓPEZ-ABAD C1, BENÍTEZ-DEL-CASTILLO JM1, GARCÍA-SÁNCHEZ J1 ABSTRACT RESUMEN Case report: We present the case of a patient who suffered from rupture of her left eye due to moderate blunt trauma. The lens, which was dislocated to the nasal and superior subconjunctival space, was extracted and the wound explored and repaired; when the process had stabilized secondary vitrectomy and suture of an IOL to the sulcus were performed, achieving a final visual acuity of 0.3. Discussion: Eye trauma is common and eye rupture may occur in those patients who have undergone ocular surgery or suffer from a debilitating condition of the eye. None of these predisposing factors existed in our case. Despite the seriousness of the problem, appropriate treatment achieved good visual function (Arch Soc Esp Oftalmol 2007; 82: 641-644). Caso clínico: Se describe el caso de una paciente que sufre estallido del globo ocular izquierdo secundario a un traumatismo de moderada intensidad. Se produjo luxación del cristalino al espacio subconjuntival nasal superior. El cristalino fue extraído y al producirse la estabilidad del cuadro se realizó vitrectomía y sutura de lente intraocular a sulcus, alcanzando una agudeza visual de 0,3. Discusión: Los traumatismos oculares son muy frecuentes y el estallido ocular suele producirse en aquellos casos que presentan patología debilitante del globo ocular o antecedentes de cirugías previas, hechos que no se presentaban en nuestro caso. A pesar de la gravedad del cuadro, la paciente alcanzó una buena función visual final. Key words: Trauma, dislocation, lens, subconjunctival space. Palabras clave: Traumatismo, luxación, cristalino, espacio subconjuntival. Received: 13/9/06. Accepted: 20/9/07. Ocular surface and inflammation unit. San Carlos Clinical Hospital. Madrid. Spain. 1 Ph.D. in Medicine. 2 Graduate in Medicine. Awarded the best 2006 communication in the Madrid Ophthalmological Society. Correspondence: Enrique Santos Bueso Servicio de Oftalmología. Hospital Clínico San Carlos Avda. Prof. Martín Lagos, s/n 28040 Madrid Spain E-mail: esbueso@hotmail.com SANTOS-BUESO E, et al. INTRODUCTION Ocular rupture with lens dislocation is a rare condition resulting from high-power traumas such as car accidents or aggressions. The eye globe tends to behave as a sphere difficult to comprehend when involved in a traumatic impact, which absorbs the energy transmitted by decreasing the anteroposterior diameter and expanding the equatorial plane. Although impacts are absorbed by the eye globe, rupture may occur where the impact took place (direct rupture) or at a certain distance (indirect rupture) (1,2). Impact tends to occur in the inferior temporal sector of the eye globe, since it is left unprotected by the orbit´s bone structure. Energy is projected towards the superior nasal region; the globe collides with the trochlea and the orbital wall. Ocular ruptures usually take place in this sector (2-4). conjunctiva with intense and generalized chemosis, full and transparent cornea and 100 percent hyphema hindering assessment of the remaining ocular structures (fig. 1). Left eye hypotony recorded 5 mm Hg intraocular pressure. The imaging tests performed (computed tomography and magnetic resonance) revealed the existence of an upper nasal paralimbic lacerated wound approximately 10 mm long and the presence of a full lens prolapsed into the subconjunctival space (figs. 2 and 3). Conjunctival chemosis evolved fast into a generalized hyposphagma, thus revealing the existence CASE REPORT A 74-year-old female patient arrived in the emergency room after having suffered a casual, mild and traumatic contusion in the left eye at home, after crashing against the nightstand. Her personal history included slight ametropia without optical correction and diabetes mellitus type 2 treated with oral antidiabetics. No other significant personal or family history were found. Her visual acuity (VA) was 0.6 in the right eye and LE light perception not improving with stenopeic spectacles. Slit lamp examination revealed hematoma and edema in the left upper eyelid, full Fig. 1: Traumatic contusion in the left eye with hematoma and edema in the right upper eyelid. 642 Fig. 2: Computed tomography revealing full globe and lens prolapsed into the subconjunctival space. Fig. 3: Nuclear magnetic resonance confirms eye globe integrity and the presence of the prolapsed lens. ARCH SOC ESP OFTALMOL 2007; 82: 641-644 Traumatic dislocation of the lens of a superior nasal subconjunctival mass (fig. 4) corresponding to the prolapsed lens. The patient underwent a 360º peritomy, extraction of the prolapsed lens, scleral wound suture and treatment with reinforced intravenous and topical antibiotherapy. One month after surgery, the patient exhibited VA of hand movement improving to 0.1 with + 14.00 diopter correction. The slit lamp revealed a transparent cornea, superior nasal corectopia with loss of iris tissue and adhered remnants (fig. 5). The eye fundus could not be observed due to media opacities. Ultrasound B mode showed the retina in place. Twelve months later, surgery combining vitrectomy via pars plana and suture of the intraocular lens to the sulcus (fig. 6) were performed, resulting in spontaneous VA of 0.3 eighteen months later. DISCUSSION Several factors favor ocular rupture with lens dislocation in the event of traumas, even if these are mild in intensity: advanced age results in rigid lenses and sclera, weakening pathologies in the eye globe such as rheumatoid arthritis, scleritis or disorders affecting the connective tissue and, above all, weakness resulting from prior surgeries, mainly large incisions such as lens extracapsular extraction (1-4). These are the main factors altering the ocular structure and responsible for those weak areas in the comprehensible globe sphere suffering from dehiscence caused by trauma. Ocular rupture tends to occur in the superior nasal sector due to the projection of energy caused by the impact in the temporal region, where impacts Fig. 4: Generalized hyposphagma and superior nasal subconjunctival mass corresponding to the prolapsed lens. ARCH SOC ESP OFTALMOL 2007; 82: 641-644 643 SANTOS-BUESO E, et al. Fig. 5: Immediate postoperative period: aphakia and superior nasal corectopia with adhered remnants and loss of iris tissue. occur more frequently (5). Energy is projected towards the superior, posterior and nasal sectors; the globe collides with the trochlea and orbital wall (2-5). Rupture usually occurs at 2.5 mm and is concentric to the limbus, where tense and deep scleral fibers are transformed into a delicate lamella of pectineous ligament (3). The case described herein is rare, since ocular rupture occurs as a result of mild trauma. Furthermore, the patient had not undergone any prior eye surgery nor did she reveal any pathologies weakening the eye globe. This type of lesions tend to result in suprachoroidal expulsive hemorrhages with massive output of ocular content, a condition not observed in the patient. Staff in the Emergency Unit should seek to preserve the integrity of the eye globe and prevent infections. Subsequently, the adequacy of surgery should be assessed in order to recover as mach visual functions as possible. REFERENCES Fig. 6: Intraocular lens sutured to the sulcus. 644 1. Kramar PO, Brandt DE. Subconjuntival dislocation of the lens. Arch Ophthalmol 1976; 94: 110-111. 2. Andonegui J, Ferro J. Subconjuntival cataract after trauma. Photo Essay. Arch Ophthalmol 2002; 120: 1102. 3. Sony P, Khokhar S, Panda A. Traumatic lenticele. Clin Experiment Ophthalmol 2005; 33: 76-77. 4. Sathish S, Chakrabarti A, Prajna V. Traumatic subconjuntival dislocation of the crystalline lens and its surgical management. Ophthalmic Surg Lasers 1999; 30: 684-686. 5. Yurkadul NS, Ugurlu S, Yilmaz A, Maden A. Traumatic subconjuntival crystalline lens dislocation. J Cataract Refract Surg 2003; 29: 2407-2410. ARCH SOC ESP OFTALMOL 2007; 82: 641-644