Distortion Product Otoacoustic Emissions
advertisement

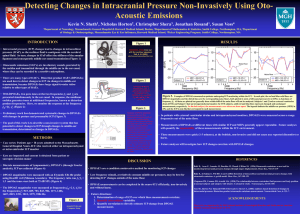
Distortion Product Otoacoustic Emissions: Comparison of Sequential versus Simultaneous Presentation of Primary-Tone Pairs Randall C. Beattie* Abstract This Grason-Stadler GSI-60 system for measuring distortion product otoacoustic emissions (DPOAEs) allows the examiner to present one set of primary-tone pairs at a time (i.e., sequential presentation), or to present as many as four sets of primary-tone pairs at a time (i.e., simultaneous presentation). The Sequential and Simultaneous protocols were used to compare administration times, DPOAEs, and noise floors (NFs) on normal-hearing subjects at three frequencies (f2 = 1000, 2000, and 4000 Hz) and eight intensities (L1 = 40–75 dB SPL in 5 dB steps; L2 = 30–65 dB SPL). The Simultaneous protocol was completed in less than half the time (mean = 2 minutes, 21 seconds) required for the Sequential protocol (mean = 5 minutes, 13 seconds). When stimulus intensity (L1) was <60 dB SPL, the Sequential and Simultaneous protocols yielded similar DPOAEs and NFs. However, at the higher L1 intensities, the NFs for the Simultaneous protocol were larger than those for the Sequential protocol. The higher Simultaneous NFs reflect the greater system distortion/noise generated by the GSI-60 instrumentation. Reliability was assessed using the standard error of measurement of the difference between two scores. The data revealed no significant differences between protocols, and suggest that differences between two DPOAEs are statistically significant if they exceed ~7 dB (95% confidence interval). Key Words: Distortion product otoacoustic emissions, Grason-Stadler GSI60, input-output functions, sequential presentation of primary-tone pairs, simultaneous presentation of primary-tone pairs, test-retest reliability Abbreviations: ANSI = American National Standards Institute; DPOAE = distortion product otoacoustic emissions; f1 = lower value in Hertz of two paired primary tones; f2 = higher value in Hertz of two paired primary tones; FFT = fast Fourier transform; L1 = sound pressure level in decibels of the f1 frequency; L2 = sound pressure level in decibels of the f2 frequency; NF = noise floor; SPL = sound pressure level in decibels; RMS = root mean squared Sumario Este sistema Grason-Stadler (GSI-60) para la medición de emisiones otoacústicas por productos de distorsión (DPOAE) permite al examinador la presentación de un juego de pares de tonos primarios al mismo tiempo (p.e., presentación secuencial), o presentar hasta cuatro juegos de pares de tonos primarios a la vez (p.e., presentación simultánea). Se utilizaron los protocolos Secuencial y Simultáneo para comparar los tiempos de administración, las DPOAE y los pisos de ruido (NF) en sujetos normo-oyentes, en tres frecuencias (f2 = 1000, 2000 y 4000 Hz) y ocho intensidades (L1 = 40-75 dB en pasos de 5 dB; L2 = 30-65 dB SPL). El protocolo Simultáneo se completó en menos de la mitad del tiempo (media = 2 minutos, 21 segundos) requerido por el protocolo Secuencial (media = 5 minutos, 13 segundos). Cuando la intensidad del estí- * Department of Communicative Disorders, California State University, Long Beach Reprint requests: Randall C. Beattie, Department of Communicative Disorders, California State University, Long Beach, 1250 Bellflower Blvd., Long Beach, CA 90840; Phone: 562-985-5281; E-mail: BeattieR@csulb.edu 471 Journal of the American Academy of Audiology/Volume 14, Number 9, 2003 mulo (L1) fue £60 dB SPL, los protocolos Secuencial y Simultáneo rindieron DPOAE y NF similares. Sin embargo, en las intensidades L1 más altas, los NF para el protocolo Simultáneo fueron mayores que aquellas para el protocolo Secuencial. Los NF Simultáneos más altos reflejan la mayor distorsión/ruido del sistema, generado por la instrumentación del GSI-60. La confiabilidad fue evaluada utilizando el error estándar de medición de la diferencia entre los dos puntajes. Los datos revelaron que no había diferencias significativas entre los protocolos, y sugieren que las diferencias entre dos DPOAE son estadísticamente significativas si exceden ~7 dB (intervalo de confianza del 95%). Palabras Clave: Emisiones otoacústicas por productos de distorsión; GrasonStadler GSI-60; funciones input/output; presentación secuencial de pares de tonos primarios; presentación simultánea de pares de tonos primarios; confiabilidad test/retest. Abreviaturas: ANSI = Instituto Nacional Americano de Normal; DPOAE = emisiones otoacústicas por productos de distorsión; F1 = valor inferior en Hertz de dos tonos primarios pareados; f2 = valor superior en Hertz de dos tonos primarios pareados; FFT = transformación rápida de Fourier; L1 = nivel de presión sonora en decibeles de la frecuencia f1; L2 = nivel de presión sonora en decibeles de la frecuencia f2; NF = piso de ruido; SPL = nivel de presión sonora en decibeles; RMS = media de la raíz cuadrada. D istortion product otoacoustic emissions (DPOAEs) result from the simultaneous presentation of two tones of frequencies f1 and f2, where f2 is higher in frequency than f1 (Kemp, 1979). DPOAEs are thought to be generated by the outer hair cells and may correspond to the region where the f1 and f2 forward traveling waves maximally overlap (Brown and Kemp, 1984; Kemp, 1986; Brown, 1987; LonsburyMartin and Martin, 1990; Probst et al, 1991; Sun et al, 1996). In human ears the difference-intermodulation distortion product at the frequency 2f1-f2 (cubic difference tone) is the most prominent DPOAE. Cochlear emissions have been employed to screen newborns, evaluate difficult-to-test patients, identify middle-ear pathology, and to monitor the status of Meniere’s disease, noise-induced hearing loss, and ototoxicity (Kemp et al, 1986; Lafreniere et al, 1991; Lonsbury-Martin et al, 1993; Probst et al, 1993; Hunter et al, 1994; Kimberly et al, 1997; Mulheran and Degg, 1997; Yardley et al, 1998; Hall, 2000). DPOAEs are typically obtained by presenting pairs of primary tones sequentially at different frequencies. However, to reduce test time, one manufacturer (Grason-Stadler, Madison, WI) produces a DPOAE system in which more than one pair of primary tones 472 can be presented simultaneously. This system (GSI-60) allows the examiner to present one set of primary-tone pairs at a time (i.e., sequential presentation), or to present as many as four sets of primary-tone pairs at a time (i.e., simultaneous presentation). The GSI-60 instruction (Grason-Stadler, 1996) manual states that the Simultaneous protocol is advantageous because DPOAE data can be obtained in less time than the Sequential protocol. A shortened test may be advantageous because it allows (1) completion of testing before a difficult-to-test patient becomes uncooperative, (2) testing more patients within a given time period, and/or (3) a reduction in the cost of testing so that the procedure is affordable to more patients. Only limited data are available comparing the Sequential and Simultaneous protocols. Kim et al (1997) tested normal-hearing and hearing-impaired subjects at a single condition (L1 = 65 and L2 = 50 dB SPL) and found that the two protocols yielded similar mean DPOAE and NF amplitudes. These investigators measured recording times for six frequencies and found that the Sequential and Simultaneous protocols required typically 40–80 seconds and 11–25 seconds, respectively. That is, the Simultaneous protocol was completed in approximately Sequential versus Simultaneous/Beattie one-third to one-half the time as the Sequential protocol. Kim et al (1997) also evaluated test-retest reliability on three normal-hearing subjects and found that the standard deviation of the test-retest differences was less than 4 dB for both the Sequential and Simultaneous protocols. Some investigators suggest that it may be useful to obtain DPOAEs at more than one intensity (Stover and Norton, 1993; Hall, 2000). For example, monitoring input-output functions may be useful to identify changes in hearing following the administration of ototoxic drugs or exposure to loud noises. Input-output functions can be examined for (1) DPOAE amplitudes over a range of intensities, (2) DPOAE threshold, (3) slope of the function, and/or (4) shape of the function (Nelson and Kimberly, 1992; Lasky et al, 1994; Nelson and Zhou, 1996; Stover et al, 1996). Obtaining input-output functions also may provide a measure of loudness growth that may be useful when selecting amplification characteristics such as compression ratio (Dorn et al, 2001). When input-output functions are generated, as compared to testing at a single intensity, the potential time savings should be even greater for the Simultaneous protocol as compared to the Sequential protocol. Reliability is an essential aspect of any clinical procedure because it provides a measure of the degree of confidence that can be placed in an individual DPOAE or between DPOAEs. These decisions require that clinicians know how much of a difference in the DPOAE is necessary before they can be reasonably certain that the DPOAE change is due to an alteration in the auditory system and is not simply due to measurement error. These questions require the establishment of reliability values that estimate the degree of confidence that can be placed in an individual DPOAE or in differences between DPOAEs. In view of the limited research comparing the Sequential and Simultaneous protocols, the present study was designed to gather additional data comparing these protocols when testing over a wide range of intensities. Normal-hearing subjects were tested and retested at eight intensities (L1 = 40–75 dB SPL in 5 dB steps; L2 = 30–65 dB SPL) and at three frequencies (f2 = 1000, 2000, and 4000 Hz). The comparability of the two protocols was assessed by measuring (1) test administration times for obtaining DPOAEs at eight intensities for each of the three frequencies, (2) DPOAE amplitudes and noise floor (NF) amplitudes in the vicinity of the DPOAEs, and (3) test-retest reliability. METHOD Subjects One ear was randomly selected from 62 normal-hearing women ranging in age from 19 to 26 years (mean = 23). The subjects reported no ear infections, and a negative history of long-term noise exposure, ototoxic drugs, and hereditary hearing loss. They passed a pure-tone screening test for the octave frequencies from 500 Hz to 4000 Hz at 15 dB HL (ANSI, 1996), had normal otoscopic findings, and had normal tympanograms using a 226 Hz probe tone (static admittance ranged from 0.3 to 1.4 mmhos and the pressure peak was 0 ± 50 daPa). Additionally, no spontaneous OAEs were present within 100 Hz of the cubic difference tone (2f1-f2) for the three pairs of primary tones in which f2 = 1000, 2000, and 4000 Hz. Instrumentation Testing was conducted with a commercially available system for measuring spontaneous OAEs and DPOAEs (GrasonStadler GSI-60; Application Software Version 4.7). The probe system employed a measurement microphone and two separate speakers for presenting each of the primaries. The primaries were delivered via tubing that was coupled to the ear canal with a probe tip and rubber eartips supplied by the manufacturer. The microphone directed the output to an associated analysis board/computer that averaged ear canal responses. A sampling rate of 16 kHz was used. The data were continuously recorded into a series of 32 msec segments (frames) that were subjected to spectral analyses using a Fast Fourier Transform yielding 512 bins of data; each bin of data was 31.25 Hz wide. Test Stimuli Three pairs of frequencies in which f2 was set at 1000, 2000, and 4000 Hz were presented at an f2:f1 ratio of about 1.20 (Harris et al, 1989; Gaskill and Brown, 1990; 473 Journal of the American Academy of Audiology/Volume 14, Number 9, 2003 Lonsbury-Martin et al, 1993; Nielsen et al,1993; Rasmussen et al, 1993; Brown et al, 1994; Whitehead et al, 1995). This investigation presents data as a function of the f2 frequency. The associated distortion product frequencies (2f1-f2) were 686, 1312, and 2686 Hz. The L1 primary tone varied in 5 dB decrements from 75 to 40 dB SPL. The L2 primary tone was 10 dB less than L1 because several studies suggest that this relative level yields DPOAEs that approach maximal values (Gaskill and Brown, 1990; Hauser and Probst, 1991; Whitehead et al, 1995; Beattie and Jones, 1998). The primary tones were presented in 5 dB decrements from L1 = 75 dB SPL and L2 = 65 dB SPL to L1 = 40 dB SPL and L2 = 30 dB SPL. Data Acquisition Criteria Testing at a given frequency was terminated when a signal-to-noise ratio of 10 dB was attained. However, a minimum of 200 frames and a maximum of 1,000 frames were averaged. Moreover, a frame was rejected if it exceeded the 30 dB SPL rejection criterion or if L1 or L2 differed by more than 2 dB from the target values. These test acceptance criteria and test rejection criteria were selected because they are consistent with the values that are employed in clinical settings with this instrumentation (GrasonStadler, 1996; Kim et al, 1997; Painter, 1997, 2000). Testing was completed in a minimum of 6.4 seconds if all criteria were met, or in a maximum of 32 seconds even if all the test acceptance criteria were not met. Noise Floor Measurements The root mean squared (RMS) noise calculation averaged two bins of data (62.5 Hz) on either side of the DPOAE bin. For each sweep, the average noise value from these four bins was compared to the rejection criterion (30 dB SPL) for either acceptance or rejection of the sweep. If the noise level in the four bins was less than 30 dB SPL, the sweep was accepted and the complex FFT values were averaged in an accumulator. The noise floor levels were computed from two bins on either side of the 2f1-f2 frequency for the Sequential protocol, where f2 = 1000, 2000, or 4000 Hz. For the Simultaneous protocol, however, the GSI system uses the noise floor corresponding to the first set of primary-tone 474 pairs per group when applying the data acquisition criteria for frame rejection, test rejection, and test acceptance. Because the frequency pairs were always presented from low to high frequency for the Simultaneous protocol, the noise floor was measured around 2f1-f2 where f1 = 843 Hz and f2 = 1000 Hz. Procedures The GSI DPOAE system allows the examiner under the “Custom DP Stimulus” menu to select a Sequential or Simultaneous presentation of test stimuli. In the Sequential mode, a single pair of frequencies are presented, one at a time, in as many as 16 combinations of frequency and intensity. Growth functions were collected for each f2 frequency in the following order: 1000, 2000, and 4000 Hz. In the Simultaneous mode, the GSI system allows a maximum of four pairs of frequencies to be presented simultaneously, followed by up to three additional groups of four pairs (i.e., a total of 16 conditions). Initially, three pairs of frequencies were presented simultaneously at L1 = 75 dB SPL and L2 = 65 dB SPL. The three pairs of frequencies were then presented in 5 dB decrements down to L1 = 40 dB SPL and L2 = 30 dB SPL. The subjects were placed in a reclining chair situated in a sound-treated room (Industrial Acoustics Corporation, Series 400). They were instructed to remain quiet and very still during testing (Hall, 2000, 197). All subjects were tested with both the Sequential and Simultaneous protocols. The order of testing for the two protocols was randomized for each subject. The subjects were tested three times in each condition (T1, T2, and T3), with a 10–20 minute break that involved removal and reinsertion of the probe tip (Hall, 2000) between T1 and T2 and between T2 and T3. Data Analysis and Statistical Tests When comparing the Sequential and Simultaneous protocols, the median of the three measurements on each subject was used when calculating administration times, DPOAEs, and NFs. To evaluate the statistical significance of administration times between the Sequential and Simultaneous protocols, paired t-tests were performed using the Statistical Package for the Social Sciences Sequential versus Simultaneous/Beattie (SPSS for Windows 11.01S). Using this statistical package, a two-way analysis-ofvariance (ANOVA) for repeated measures was performed on each frequency to assess the statistical significance of eight levels of the factor “intensity” and two levels of the factor “protocol.” Tukey’s post hoc test was used to identify significant differences between means (Linton and Gallo, 1975; Bruning and Kintz, 1987). Several authors state that the standard error of measurement (SEM) is the most useful statistic for assessing test-test reliability (Guilford and Fruchter, 1973; Anastasi, 1976; Lemke and Wiersma, 1976; Ghiselli et al, 1981; Demorest, 1984; Demorest and Walden, 1984; American Psychological Association, 1985; Brown, 1989). This statistic may be used to estimate the true DPOAE from a single measurement and may be particularly useful for screening applications to assess whether an individual score deviates significantly from the norm or from a predetermined cut-off score. The SEM can be computed from the following formula: SEM = SD √1 - r where the SD is the combined standard deviation of test and retest DPOAEs and r is the Pearson product-moment correlation coefficient. The SEM allows construction of a confidence interval that contains the t r ue D PO AE. Th e pr obabi lit y is approximately 68 percent that the true DPOAE will fall within one standard error of the observed DPOAE; there is a 95 percent probability that the true DPOAE will be within two standard errors of the obtained DPOAE; and there is a 99 percent probability that the true DPOAE will lie within 2.58 standard errors of the obtained DPOAE. To assess w h eth er tw o DPOA E measurements are statistically significant, the standard error of measurement of the difference between two values (SEM∆) can be employed (Anastasi, 1976; Demorest and Walden, 1984; Mehrens and Lehmann, 1984; Brown, 1989). The two measurements may represent DPOAEs before and after noise exposure or drug administration, DPOAEs from the right ear versus the left ear, or DPOAEs from two individuals. The SEM∆ can be computed from the following formula: SEM∆ = SEM √2 where the SEM is the standard error of m ea surem ent of t he t est a nd ret est DPOAEs, and the square root of two is 1.414. Demorest and Walden state that the SEM and the SEM∆ are “the only way to ensure that measurement error is explicitly taken into account in score interpretation” (1984, 234). RESULTS Administration Time When each of the three f2 stimuli (1000, 2000, and 4000 Hz) were presented sequentially at eight levels (L1 = 40–75 dB SPL), the mean administration time for all subjects for data collection was 313 seconds (5 minutes, 13 seconds). Test times ranged from 194 to 640 seconds, with a standard deviation of 110 seconds. When the three f2 stimuli were presented simultaneously at each of the eight L1 levels, the mean administration time was 141 seconds (2 minutes, 21 seconds), the standard deviation was 63 seconds, and test times ranged from 64 to 253 seconds. The 172-second mean difference between the two protocols was statistically significant using the t-test (p < .01, t = 15.3). It is evident that the Simultaneous protocol was completed in less than half the time required for the Sequential protocol. DPOAE and NF Amplitudes Table 1 presents mean DPOAEs and NFs in dB SPL and standard deviations for the Sequential and Simultaneous protocols for three frequencies at L1 = 40–75 dB SPL. The mean data also are shown in Figure 1 for 1000 Hz (top panel), 2000 Hz (middle panel), and 4000 Hz (bottom panel). The 1000 Hz DPOAE data show similar mean SPLs (<0.5 dB) for both the Sequential and Simultaneous protocols at L1 = 40–60 dB SPL. However, somewhat higher DPOAEs were observed for the Simultaneous protocol at L1 = 65–75 dB SPL. The ANOVA revealed a statistically significant interaction (p < .01) 475 Journal of the American Academy of Audiology/Volume 14, Number 9, 2003 Table 1 Mean Distortion Product Otoacoustic Emissions (DPOAEs) and Noise Floors (NFs) in dB SPL and Standard Deviations for the Sequential and Simultaneous Protocols for f2 = 1000, 2000, and 4000 Hz at L1 = 40–75 dB SPL f2 Frequency Protocol Sequential Mean DPOAE SD Mean NF SD L1 in dB SPL 55 60 40 45 50 -3.0 0.5 2.6 4.9 6.8 4.6 5.9 -12.3 -12.1 -12.8 65 70 75 6.7 6.4 6.1 5.6 6.4 6.5 7.4 6.4 5.7 -10.8 -11.9 -11.7 -10.2 -11.6 8.0 4.4 6.1 6.2 5.8 6.3 6.9 6.9 -3.4 0.1 2.8 4.7 6.8 8.1 9.1 10.6 6.4 5.9 5.8 6.3 6.2 5.8 5.1 5.7 -12.3 -10.1 -9.8 -9.2 -7.0 -3.1 2.8 1000 Hz Simultaneous Mean DPOAE SD Mean NF SD Sequential Mean DPOAE SD Mean NF SD -12.8 6.5 5.8 7.1 5.2 4.6 3.7 3.0 3.9 -9.1 -7.5 -4.1 -0.3 3.1 5.5 7.1 8.9 8.0 8.0 7.1 6.7 6.0 7.2 7.2 6.6 -18.0 -19.0 -17.6 -17.6 -17.0 -16.6 -14.2 -17.6 6.4 7.6 4.9 5.3 5.4 5.6 6.5 5.8 -9.2 -6.7 -4.6 -0.5 2.2 5.4 6.9 6.6 10.1 8.0 7.1 7.3 7.5 6.1 5.5 6.0 -18.0 -17.1 -16.4 -14.5 -14.8 -10.0 -4.5 2000 Hz Simultaneous Mean DPOAE SD Mean NF SD Sequential Mean DPOAE SD Mean NF SD -18.5 7.7 6.8 7.2 6.3 8.7 4.6 5.8 4.5 -10.3 -7.4 -2.9 0.9 4.2 6.9 7.0 5.2 5.6 6.7 6.9 6.4 5.5 5.1 6.0 7.0 -22.0 -21.2 -21.0 -20.7 -20.4 -20.3 -20.5 -22.9 5.0 4.8 5.1 5.5 5.7 6.0 7.9 5.3 -10.3 -6.8 -2.9 0.3 4.1 6.4 6.9 6.4 7.1 6.4 6.7 6.2 5.8 5.2 5.3 6.9 -22.9 -22.9 -21.1 -20.2 -15.1 -6.8 -0.2 5.5 4.7 3.3 3.4 8.3 4000 Hz Simultaneous Mean DPOAE SD Mean NF SD between the intensity and protocol factors. Tukey’s post hoc test showed statistically significant differences (p < .01) between the Sequential and Simultaneous protocols at L1 = 70 and 75 dB SPL. The Simultaneous protocol yielded means that were 3 dB higher than the Sequential protocol at L1 = 70 dB SPL and 5 dB higher at L1 = 75 dB SPL. Significant differences between protocols 476 -21.6 9.3 5.3 5.7 were not observed at the lower L1 intensities. Standard deviations were similar across intensities and were about 6 dB for both protocols. The top panel in Figure 1 shows that the NFs associated the Sequential and Simultaneous protocols differed by less than 3 dB for L1 = 40–60 dB SPL; these differences were not statistically significant (p > .01) using the Tukey test. However, the Sequential versus Simultaneous/Beattie Figure 1 Mean DPOAEs in dB SPL are presented for the Sequential protocol (closed circles, solid line) and the Simultaneous protocol (stars, dotted line) for f2 = 1000 Hz (top panel), 2000 Hz (middle panel), and 4000 Hz (bottom panel) at L1 = 40–75 dB SPL. The associated mean NFs in dB SPL also are shown for the Sequential protocol (triangles, dashed line) and the Simultaneous protocol (closed squares, dotteddashed line). Simultaneous NFs were higher than the Sequential NFs at L1 = 65–75 dB SPL (p < .01). The figure shows that the Simultaneous minus Sequential differences increased from 4.7 dB at L1 = 65 dB SPL to 14.4 dB at L1 = 75 dB SPL. The 2000 Hz data in Figure 1 shows that the DPOAEs for the Sequential and Simultaneous protocols differed by less than 1 dB for L1 = 40–70 dB SPL. At L1 = 75 dB SPL, however, the Sequential protocol yielded a DPOAE that was higher (8.9 dB SPL) than the Simultaneous DPOAE (6.6 dB SPL). The two-way ANOVA yielded a statistically significant interaction between the protocol and intensity factors, and the Tukey test revealed that the Sequential DPOAE was significantly higher (p < .01) than the Simultaneous DPOAE at L1 = 75 dB SPL. The DPOAEs for the two protocols did not differ significantly (p > .01) at the other intensities. For L1 = 40–65 dB SPL, the middle panel in Figure1 shows that the Sequential and Simultaneous NFs associated with 2000 Hz differed by <3.1 dB. These differences were not statistically significant using the Tukey test. The noise floor was significantly higher (p < .01) for the Simultaneous protocol than with the Sequential protocol for L1 = 70–75 dB SPL. These differences were 6.6 dB at 70 dB SPL and 9.7 dB at 75 dB SPL. The bottom panel in Figure 1 shows that the Sequential and Simultaneous DPOAEs for 4000 Hz were similar (<1.2 dB) as L1 increased from 40 to 75 dB SPL. The effects of protocol and the interaction between protocol and intensity were not statistically significant (p < .01) when tested with a twoway ANOVA for repeated measures. The 4000 Hz NF data in the bottom panel of Figure 1 illustrate similar values (<2 dB) for the Sequential and Simultaneous protocols for L1 = 40–60 dB SPL. However, the Tukey test indicated that the NFs associated with the Simultaneous protocol were higher (p < .01) than the Sequential protocol at L1 = 65, 70, and 75 dB SPL. These differences increased from approximately 5 dB at L1 = 65 dB SPL to 20 dB at L1 = 75 dB SPL. Reliability Table 2 presents SEM values for the Sequential and Simultaneous protocols at three frequencies (f1 = 1000, 2000, and 4000 477 Journal of the American Academy of Audiology/Volume 14, Number 9, 2003 Table 2 L1 in dB SPL Standard Errors of Measurement for the Sequential (Seq) and Simultaneous (Simul) Protocols 1000 Hz Seq Simul Com 2000 Hz Seq Simul Com Seq 4000 Hz Simul Com Combined 1000–4000 Hz Seq Simul Com 75 4.2 2.3 3.3 1.5 1.5 1.5 2.5 2.7 2.6 2.7 2.2 2.5 70 2.9 2.3 2.6 2.3 2.5 2.4 1.7 1.2 1.5 2.3 2.0 2.2 65 2.6 2.9 2.7 2.2 2.0 2.1 1.4 1.5 1.5 2.1 2.1 2.1 60 2.8 2.5 2.7 2.1 2.9 2.5 1.9 1.7 1.8 2.3 2.4 2.3 55 2.5 3.2 2.8 2.2 2.7 2.5 2.6 2.2 2.4 2.4 2.7 2.5 50 2.3 2.3 2.3 2.5 3.3 2.9 2.8 3.3 1.1 2.5 3.0 2.8 45 3.1 4.1 3.6 3.0 3.2 3.1 2.5 1.9 2.2 2.9 3.1 3.0 40 4.2 4.8 4.5 4.3 5.2 4.7 3.2 3.7 3.5 3.9 4.6 4.3 Combined 40–75 3.1 3.1 3.1 2.5 2.9 2.7 2.3 2.3 2.3 2.6 2.8 2.7 Combined 45–75 2.9 2.8 2.9 2.4 2.6 2.5 2.2 2.1 2.1 2.5 2.5 2.5 Note: The first column presents L1 intensities in dB SPL. The next nine columns present data for the three f2 frequencies. The last three columns present data combined (Com) across the f2 frequencies. The bottom two rows present data that were combined across protocols, frequencies, and intensities for all eight intensities (L1 = 40–75 dB SPL) and for the seven higher intensities (L1 = 45–75 dB SPL). Hz) and eight intensities (L1 = 40–75 dB SPL). The table also presents the data combined across protocols, frequencies, and intensities. These SEM values represent the mean of three measurements (T1 vs. T2, T1 vs. T3, and T2 vs. T3). Examination of the SEM values in Table 2 reveals three major observations. First, with one exception (1000 Hz at 75 dB SPL), the standard errors were similar (<1 dB) for the Sequential and Simultaneous protocols at all intensities and frequencies. When the protocol data were combined across all frequencies and intensities, SEM values were 2.6 dB for the Sequential protocol and 2.8 dB for the Simultaneous protocol. Second, the SEM values tended to decrease slightly as frequency increased. That is, when the SEM values were combined across protocols and intensities, the standard errors were 3.1 dB at 1000 Hz, 2.7 dB at 2000 Hz, and 2.3 dB at 4000 Hz. When the data were combined across all conditions, the SEM was 2.7 dB. Third, somewhat larger standard errors were observed at L1 = 40 dB SPL than at the higher intensities. That is, when combined across protocols and frequencies, the standard errors were 4.3 dB at L1 = 40 dB SPL and 2.5 dB for L1 = 45–75 dB SPL. Using the 2.5 dB standard error value as representative of the 478 Sequential and Simultaneous protocols across frequency and for L1 = 45–75 dB SPL, the test-retest data suggest that there is a 95 percent probability that an individual’s true DPOAE will fall within 5 dB (two standard errors) of the obtained DPOAE. The SEM ∆ was employed to assess whether two DPOAE measurements are statistically significant. Using the combined standard error of measurement for the L1 = 45–75 dB SPL (2.5 dB), the SEM∆ is 3.5 dB (2.5 dB X 1.414 = 3.5 dB). The SEM∆ can be multiplied by 1.64 (90 percent confidence interval), 1.96 (95 percent confidence interval), or 2.58 (99 percent confidence interval) to determine if two DPOAEs are statistically significant at the selected confidence level. Using the 95 percent confidence interval (.05 level), the difference between two DPOAEs is statistically significant if it exceeds 6.9 dB (3.5 dB X 1.96 = 6.9 dB). DISCUSSION Administration Time The Simultaneous protocol was completed in less than half the time (two Sequential versus Simultaneous/Beattie minutes, 21 seconds) required for the Sequential protocol (five minutes, 13 seconds). These data are consistent with those reported by Kim et al (1997), who stated that the Simultaneous protocol was completed in onethird to one-half the time as compared to the Sequential protocol. The times presented in the current report represent the durations required to test three frequencies at eight intensities each (one trial only). Obtaining two sets of data to assess reliability, which some investigators advocate (Hall, 2000; Beattie et al, 2003), would approximately double the test times. The Simultaneous protocol may be particularly useful when the examiner requires data at numerous frequencies and/or intensities. In addition to research applications, this testing may include noise or drug monitoring in which input-output functions are generated. The Simultaneous protocol also may be preferred when evaluating difficult-to-test patients who are unable or unwilling to remain still for the required time period using the Sequential protocol. DPOAE and NF Amplitudes The results showed that when stimulus intensity (L1) was <60 dB SPL, the differences between the DPOAEs and NFs derived from the Sequential and Simultaneous protocols were similar and statistically nonsignificant at f2 = 1000, 2000, and 4000 Hz. However, at the higher L1 intensities, the NFs for the Simultaneous protocol were larger than those for the Sequential protocol, and this difference systematically increased as L1 increased from 60 to 75 dB SPL. The largest differences were observed for NFs associated with 4000 Hz, where the Simultaneous NFs were approximately 5, 13, and 20 dB larger than the Sequential NFs at the respective L1 intensities of 65, 70, and 75 dB SPL. At the highest intensity (L1 = 75 dB SPL), the Simultaneous DPOAEs also were slightly greater (3–5 dB) than the Sequential DPOAEs at 1000 and 2000 Hz. For the Simultaneous NFs, signal averaging continued at all frequencies (f2 = 1000, 2000, and 4000 Hz) until the preset signal-to-noise ratio (+10 dB) of the first frequency tested (i.e., f2 = 1000 Hz) was achieved or until the 32-second time limit at a particular intensity was reached. That is, the GSI-60 Simultaneous protocol monitors the noise floor status for the first set of primary-tone pairs per group, which was f1 = 843 Hz and f2 = 1000 Hz. Because more noise typically is measured around the DPOAE associated with1000 Hz than for 2000 or 4000 Hz (see Figure 1), signal averaging at 2000 and 4000 Hz for the Simultaneous protocol may continue somewhat longer and result in lower NFs than for the Sequential protocol. To the contrary, however, the Simultaneous protocol yielded NFs that were higher than the NFs for the Sequential protocol at L1 = 65–75 dB SPL. A likely explanation is that the Simultaneous protocol produced higher system distortion and/or system noise because of the interaction of the six primary tones (three sets of two tones). That is, the interaction of the six primary tones generated system harmonic and/or intermodulation distortion products that fell within the NF bins. Recall that each bin is 31.25 Hz wide and that the NF values represent the RMS average of two bins (62.5 Hz wide) on either side of the DPOAE frequency bin. If system distortion products or system noise are present in any of the four bins around the DPOAE bin, the overall (RMS) NF value will be elevated. To estimate system noise, the probe tip was sealed in a 2cc coupler, and NFs were measured for the Simultaneous and Sequential protocols. The NF values in dB SPL are presented in Table 3 for each test frequency and intensity. The Sequential NF values are similar to those reported by Dorn et al (2001). For the L1 intensities below 60 dB SPL, the NFs for the two protocols were similar and varied <4 dB. The table also shows that the Simultaneous protocol yielded higher NFs than the Sequential protocol at the highest L1 intensities. At L1 = 75 dB SPL, these NF differences were 27 dB at 1000 Hz, 23 dB at 2000 Hz, and 35 dB at 4000 Hz. Moreover, at L1 = 65–75 dB SPL for the Simultaneous protocol, the system distortion/noise measurements are similar to the NF values obtained under test conditions. For 2000 Hz at L1 = 75 dB SPL, for example, note that the system noise was -6 dB SPL (Table 3) and the mean NF was -4.5 dB (Table 1). Because the Simultaneous NFs were greater than the Sequential NFs only at the higher intensities (L1 > 65 dB SPL) where greater system distortion was 479 Journal of the American Academy of Audiology/Volume 14, Number 9, 2003 Table 3 f2 Frequency System Noise/Distortion (2cc Coupler Measurements) for the Sequential and Simultaneous Protocols at Three Frequencies and Eight L1 Intensities Protocol L1 in dB SPL 55 60 40 45 50 65 70 75 Sequential -28 -24 -31 -22 -26 -22 -28 -22 Simultaneous -26 -25 -27 -24 -13 -7 -2 5 Sequential -29 -34 -28 -29 -31 -28 -25 -29 Simultaneous -28 -30 -29 -30 -29 -24 -16 -6 Sequential -28 -32 -33 -31 -34 -33 -35 -32 Simultaneous -29 -30 -30 -29 -27 -16 -7 3 1000 Hz 2000 Hz 4000 Hz Note: System noise floor values are in dB SPL and represent RMS values for two bins of data on either side of the cubic difference tone. measured, we conclude that the higher Simultaneous NFs reflect the greater system distortion/noise generated by the interaction of the six primary tones. Larger DPOAEs were observed at the higher intensities for the Simultaneous protocol than for the Sequential protocol. These larger DPOAEs also may reflect the system distortions discussed above because the DPOAE values represent both the DPOAE and noise (biologic, environmental, instrument) within the 31.25 Hz wide bin of interest (Beattie and Ireland, 2000). Thus, instrument noise in the form of distortion products within the DPOAE bin may elevate the DPOAE. Another explanation for the higher Simultaneous DPOAEs was suggested by Kim et al (1997), who state that presenting several pairs of tones simultaneously is likely to result in complicated interactions among the distortion products that may be enhanced or suppressed. Although many investigators suggest L1 screening levels of ~60 dB SPL, high-level testing may be used when testing hearingimpaired subjects or when generating inputoutput functions (Gorga et al, 1996; Hall, 2000; Robinette and Glattke, 2002). The present study suggests that caution should be used when moderate to high level (L1 > 65 dB SPL) primary tones are presented using the Simultaneous protocol. That is, using the GSI-60 instrumentation, the NFs for the Sequential and Simultaneous protocols are not equivalent when data are collected at moderate to high levels. These findings should be replicated with other instrumentation 480 (speakers) that may exhibit different degrees of system noise/distortion. Moreover, different findings would be expected if the bin width is varied or if different bins are used to calculate the NF (e.g., those without high levels of distortion). Reliability Test-retest reliability was assessed in which the retest followed a 10–20 minute break that included probe tip removal and replacement. The short time interval minimizes the likelihood of changes in hearing, environmental or subject noise, procedures, or equipment (Franklin et al, 1992; Prieve et al, 1993; Roede et al, 1993; Marshall and Heller, 1996; Zhao and Stephens, 1999). DPOAE amplitude and noise level differences on the test and retest may be due to changes in probe placement, changes in middle-ear status (e.g., swallowing or coughing may alter middle-ear pressure), and/or variable subject noise. Zhao and Stephens (1999) state that changing the position of the probe tip may affect (1) the level of background noise in the ear canal, particularly at the low frequencies, (2) acoustic leakage, and (3) the interaction of the ear canal resonances and the acoustic stimuli. Beattie et al (2003) reported no test-retest reliability differences between the very shortterm measurements (retest following probe removal and a 10–20 minute break) and short-term measurements (5–10 days between test and retest). These authors concluded that probe removal and Sequential versus Simultaneous/Beattie replacement was the major factor that contributed to the increased variability (0.5 dB to 1.0 dB) between the immediate testretest measurements and the very shortterm and short-term measurements. Roede et al (1993) state that middle-ear changes in fluid or air pressure will have more effect on the low-frequency DPOAEs than on the higher frequencies. The standard errors were similar for the Sequential and Simultaneous protocols. When combined across all frequencies and intensities, the SEM values were 2.6 dB for the Sequential protocol and 2.8 dB for the Simultaneous protocol. When the data were combined across all conditions, the combined SEM was 2.5 dB. These protocol findings are consistent with those of Kim et al (1997), who reported no differences in reliability between the Sequential and Simultaneous procedures. We also found that the standard errors tended to decrease slightly as frequency increased from 1000 Hz (2.9 dB) to 4000 Hz (2.1 dB). Larger standard errors may be observed at the lower frequencies as compared to the higher frequencies because the former is associated with more variable immittance and more variable noise (Roede et al, 1993; Zhao and Stephens, 1999). However, Beattie et al (2003) found similar standard errors of about 2.5 dB for 1000–4000 Hz. When combined across protocols and frequencies, somewhat larger standard errors were observed for L1 = 40 dB SPL (SEM = 4.3 dB) than for L1 = 45–75 dB SPL (SEM = 2.5 dB). The improved reliability at the higher intensities may be the result of reduced variability in the background noise because of a greater signal-to-noise ratio. That is, at the higher intensities, DPOAEs may have been sufficiently high in comparison to the background noise so that the noise had little effect on the signal in the DPOAE bin. The DPOAE bin contains both the relatively stable DPOAE and relatively variable noise. Kimberly et al (1997) suggest that if the noise is approximately 12 dB below the DPOAE, the noise will have little effect on the DPOAE. In contrast to the foregoing explanation, however, Table 2 shows that the Simultaneous protocol at L1 = 75 dB SPL (1000 and 4000 Hz) yielded SEMs of ~2.3 dB even though the associated signal-to-noise ratios were similar to the L1 = 40 dB SPL conditions. Although comparisons with previous studies must be made with reservations because of differences in experimental design, the present SEM values (~2.5 dB) are identical to those reported by Beattie et al (2003) using similar procedures. Slightly smaller standard errors were reported by Beattie and Bleech (2000) and Franklin et al (1992). The immediate test-retest standard errors reported by Beattie and Bleech (2000) under similar conditions (L1 = L2 = 55 dB SPL) were ~1.7 dB for 1000, 2000, and 4000 Hz. Franklin et al (1992) reported similar reliabilities for measurements taken over four consecutive days and on four successive weeks. For the L1 = L2 = 65 dB SPL condition, they observed standard errors of about 3.1 dB at 1000 Hz, 1.8 dB at 2000 Hz, and 1.3 dB at 4000 Hz (Franklin et al, 1992, table 2, 423). To assess the consistency of DPOAEs, clinicians may obtain two or three sets of measurements. Hall (2000) suggests that, to assess reliability, two or three measurements should be obtained in which the probe tip is removed between measurements. He states: “False-negative screening outcomes can be minimized by insisting on two replicable DPgrams for each ear (DP amplitudes within +1 or 2 dB for each frequency)” (Hall, 2000, 429). Our SEM∆ data suggest, however, that the differences between two DPOAEs must exceed approximately 7 dB at 1000–4000 Hz to be statistically significant at the 0.05 level of confidence. This value agrees with the 6–7 dB values suggested by Beattie and Bleech (2000) and Beattie et al (2003). Test-retest differences that exceed these values, in the absence of any pathologic condition (e.g., ototoxic drugs, noise trauma, or middle-ear infections), are unusual and warrant repeat testing until stable findings are obtained. If repeat measurements verify differences that exceed these values, however, it is likely that the differences represent an actual change in the auditory system and are not the result of measurement error. SUMMARY AND CONCLUSIONS T he Simultaneous protocol was completed in less than half the time required for the Sequential protocol. The Simultaneous protocol may be preferred when evaluating individuals who have difficulty remaining still for any period of time, and may be particularly useful when data are required at numerous frequencies and/or intensities. Using the GSI-60 instrumentation, the NFs for the Sequential and Simultaneous 481 Journal of the American Academy of Audiology/Volume 14, Number 9, 2003 protocols are not equivalent when data are collected at moderate to high levels (L1 ≥ 65 dB SPL). The Simultaneous protocol yielded higher NFs than the Sequential protocol, which is believed to be due to higher system distortion that results from the interaction of the six primary tones. When stimulus intensity (L1) was ≤60 dB SPL, the Sequential and Simultaneous protocols yielded similar DPOAEs and NFs at all tested frequencies. At the highest intensity (L1 = 75 dB SPL), the Simultaneous DPOAEs also were slightly greater (3–5 dB) than Sequential DPOAEs at 1000 Hz and 2000 Hz. Depending on procedural variables such as the minimum number of frames averaged and the specified signal-to-noise ratio, elevated NFs may result in increased DPOAE amplitudes (Beattie and Ireland, 2000). No differences in reliability were observed between the Sequential and Simultaneous protocols when the data were combined across all frequencies and intensities. The SEM values tended to decrease as f2 frequency increased. Using the 2.5 dB standard error value as representative of the Sequential and Simultaneous protocols across frequency and for L1 = 45–75 dB SPL, the test-retest data suggest that there is a 95 percent probability that an individual’s true DPOAE will fall within 5 dB (two standard errors) of the obtained DPOAE. Reliability also was assessed using the SEM∆ (3.5 dB). Using the 95 percent confidence interval, the difference between two DPOAEs is statistically significant if it exceeds ~7 dB. Test-retest differences that exceed these values are unusual and warrant repeat testing until stable findings are obtained. REFERENCES American National Standards Institute. (1996). American National Standard Specifications for Audiometers. ANSI S3.6-1996. New York: American National Standards Institute. American Psychological Association. (1985). Standards for Educational and Psychological Testing. Washington, DC: American Psychological Association. Anastasi A. (1976). Psychological Testing. 4th ed. New York: MacMillan. Beattie RC, Bleech J. (2000). Effects of sample size on the reliability of noise floor and DPOAE. Brit J Audiol 34:305–309. Beattie RC, Ireland A. (2000). Effects of sample size on the noise floor and distortion product otoacoustic emissions. Scand Audiol 29:93–102. Beattie RC, Jones RL. (1998). Effects of relative levels of the primary tones on distortion product otoacoustic emissions in normal-hearing subjects. Audiol 37:187–197. Beattie RC, Kenworthy OT, Luna CA. (2003). Immediate and short-term reliability of distortionproduct otoacoustic emissions. Int J Audiol 42:348–354. Brown AM. (1987). Acoustic distortion from rodent ears: a comparison of responses from rats, guinea pigs, and gerbils. Hear Res 31:25–39. Brown AM, Kemp DT. (1984). Suppressibility of 2F1F2 stimulated acoustic emissions in gerbil and man. Hear Res 13:29–37. Brown AM, Sheppard SL, Russell PT. (1994). Acoustic distortion products (ADP) from the ears of term infants and young adults using low stimulus levels. Brit J Audiol 28:273–280. Brown JR. (1989). The truth about scores children achieve on tests. Lang Speech Hear Services Schools 20:366–371. Bruning JL, Kintz BL. (1987). Computational Handbook of Statistics. 3rd ed. Glenview, IL: Scott, Foresman and Company. Demorest ME. (1984). Psychometric issues in speech recognition testing. ASHA Reports 14:19–22. Demorest ME, Walden BE. (1984). Psychometric principles in the selection, interpretation, and evaluation of communication self-assessment inventories. J Speech Hear Disord 49:226–240. Dorn PA, Konrad-Martin D, Neely ST, Keefe DH, Cyr E, Gorga MP. (2001). Distortion product otoacoustic emission input/output functions in normal-hearing and hearing-impaired human ears. J Acoust Soc Am 110:3119–3131. Franklin DJ, McCoy MJ, Martin GK, LonsburyMartin BL. (1992). Test/retest reliability of distortion-product and transiently evoked otoacoustic emissions. Ear Hear 13:417–429. 482 Sequential versus Simultaneous/Beattie Gaskill SA, Brown AM. (1990). The behavior of the acoustic distortion product, 2f1-f2, from the human ear and its relation to auditory sensitivity. J Acoust Soc Am 88:821–839. Ghiselli EE, Campbell JP, Zedeck S. (1981). Measurement Theory for the Behavioral Sciences. San Francisco: W. H. Freeman. Gorga MP, Stover L, Neely ST. (1996). The use of cumulative distributions to determine critical values and levels of confidence for clinical distortion product otoacoustic emission measurements. J Acoust Soc Am 100:968–977. Grason-Stadler. (1996). Grason-Stadler GSI-60 DPOAE—Distortion Product Otoacoustic Emissions System User Manual. Milford, NH: GSI GrasonStadler. Guilford JP, Fruchter B. (1973). Fundamental Statistics in Psychology and Education. 5th ed. New York: McGraw-Hill. Hall JW. (2000). Handbook of Otoacoustic Emissions. San Diego, CA: Singular Publishing Group. Harris FP, Lonsbury-Martin BL, Stagner BB, Coats AC, Martin GK. (1989). Acoustic distortion products in humans: systematic changes in amplitude as a function of f2/f1 ratio. J Acoust Soc Am 85:220–229. Hauser R, Probst R. (1991). The influence of systematic primary-tone level variation L2-L1 on the acoustic distortion product emission 2F1-F2 in normal human ears. J Acoust Soc Am 89:280–286. Hunter MF, Kimm L, Cafarlli DD, Kennedy CR, Thornton AR. (1994). Feasibility of otoacoustic emission detection followed by ABR as universal neonatal screening test for hearing impairment. Brit J Audiol 28:47–51. Kemp DT. (1979). Evidence of mechanical nonlinearity and frequency selective wave amplification in the cochlea. Arch Otolaryngol 224:37–45. Kemp DT. (1986). Otoacoustic emissions, traveling waves and cochlear mechanics. Hear Res 22:95–104. Kemp DT, Bray P, Alexander L, Brown AM. (1986). Acoustic emission cochleography—practical aspects. Scand Audiol Suppl 15:71–96. Kim DO, Sun SM, Jung MD, Leonard G. (1997). A new method of measuring distortion product otoacoustic emissions using multiple tone pairs: study of human adults. Ear Hear 18:277–285. Lemke E, Wiersma W. (1976). Principles of Psychological Measurement. Chicago: Rand McNally. Linton M, Gallo PS. (1975). The Practical Statistician: Simplified Handbook of Statistics. Belmont, CA: Wadsworth Publishing Company. Lonsbury-Martin BL, Martin GK. (1990). The clinical utility of distortion-product otoacoustic emissions. Ear Hear 11:144–154. Lonsbury-Martin B, McCoy M, Whitehead M, Martin G. (1993). Clinical testing of distortion-product otoacoustic emissions. Ear Hear 14:11–22. Marshall L, Heller LM. (1996). Reliability of transient-evoked otoacoustic emissions. Ear Hear 17:237–254. Mehrens WA, Lehmann IJ. (1984). Measurement and Evaluation in Education and Psychology. New York: Holt, Rinehart and Winston. Mulheran M, Degg C. (1997). Comparison of distortion product OAE generation between a patient group requiring frequent gentamicin therapy and control subjects. Brit J Audiol 31:5–9. Nelson DA, Kimberly BP. (1992). Distortion-product emissions and auditory sensitivity in human ears with normal hearing and cochlear hearing loss. J Speech Hear Res 35:1142–1159. Nelson DA, Zhou JZ. (1996). Slopes of distortion-product otoacoustic emission growth curves corrected for noise floor levels. J Acoust Soc Am 99:468–474. Nielsen LH, Popelka GR, Rasmussen AN, Osterhammel PA. (1993). Clinical significance of probe-tone frequency ratio on distortion product otoacoustic emissions. Scand Audiol 22:159–164. Painter J. (1997). Basic instrumentation issues in acquiring distortion product otoacoustic emissions. In: Robinette MS, Glattke TJ, eds. Otoacoustic Emissions. New York: Thieme, 333–346. Painter J. (2000). Grason Stadler Incorporated (GSI). In: Hall JW, ed. Handbook of Otoacoustic Emissions. San Diego, CA: Singular Publishing Group, 291–303. Prieve BA, Gorga MP, Schmidt A, Neely S, Peters J, Schultes L, Jesteadt W. (1993). Analysis of transientevoked emissions in normal-hearing and hearing-impaired ears. J Acoust Soc Am 93:3308–3319. Probst R, Harris FP, Hauser R. (1993). Clinical monitoring using otoacoustic emissions. Brit J Audiol 27:85–90. Kimberly BP, Brown DK, Allen JB. (1997). Distortion product emissions and sensorineural hearing loss. In: Robinette MS, Glattke TJ, eds. Otoacoustic Emissions. New York: Thieme, 181–204. Probst R, Lonsbury-Martin B, Martin G. (1991). A review of otoacoustic emissions. J Acoust Soc Am 89:2053–2055. Lafreniere D, Jung MD, Smurzynski J, Leonard G, Kim DO, Sasek J. (1991). Distortion-product and clickevoked otoacoustic emissions in healthy newborns. Arch Otolaryngol 117:1382–1389. Rasmussen AN, Popelka GR, Osterhammel PA, Nielsen LH. (1993). Clinical significance of relative probe levels on distortion product otoacoustic emissions. Scand Audiol 22:223–229. Lasky RE, Snodgrass E, Hecox K. (1994). Distortionproduct otoacoustic emission input/output functions as a function of frequency in human adults. J Am Acad Audiol 5:183–194. Robinette MS, Glattke TJ. (2002). Otoacoustic Emissions: Clinical Applications. 2nd ed. New York: Thieme. 483 Journal of the American Academy of Audiology/Volume 14, Number 9, 2003 Roede J, Harris FP, Probst R, Xu L. (1993). Repeatability of distortion product otoacoustic emissions in normally hearing humans. Audiol 32:273–281. Stover L, Gorga MP, Neely ST, Montoya D. (1996). Toward optimizing the clinical utility of distortion product otoacoustic emission measurements. J Acoust Soc Am 100:956–967. Stover L, Norton SJ. (1993). The effects of aging on otoacoustic emissions. J Acoust Soc Am 94:2670–2681. Sun X , Kim DO , Jung MD, Randolph KJ. (1996). Distortion product otoacoustic emission test of sensorineural hearing loss in humans: comparison of unequal- and equal-level stimuli. Ann Otol Rhinol Laryngol 105:982–990. Whitehead ML, McCoy MJ, Lonsbury-Martin BL, Martin GK. (1995). Dependence of distortionproduct otoacoustic emissions on primary levels in normal and impaired ears. I. Effects of decreasing L2 below L1. J Acoust Soc Am 97:2346–2358. Yardley MP, Davies CM, Stevens JC. (1998). Use of transient evoked otoacoustic emissions to detect and monitor cochlear damage caused by platinumcontaining drugs. Brit J Audiol 32:306–316. Zhao F, Stephens D. (1999). Test-retest variability of distortion-product otoacoustic emissions in human ears with normal hearing. Scand Audiol 28:171–178. 484