neurocognitive subtypes in patients with schizophrenia and their
advertisement

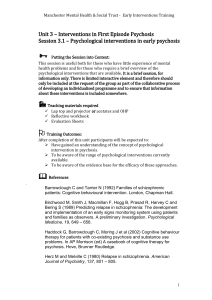
NEUROCOGNITIVE SUBTYPES IN PATIENTS WITH SCHIZOPHRENIA AND THEIR ASSOCIATED ! CLINICAL FEATURES! ! J. Ospina-Duque1, A. Rangel2, C. Muñoz3, M. Ocampo4, C. Quintero3, M. Escobar3, S. Botero3, C. Marín4, L. Jaramillo5, R. Sánchez5, J. Rodríguez5, D. Aguirre6, C. Palacio1 and J. García2.! ! (1)Research Group in Psychiatry GIPSI, University of Antioquia, Medellín, Colombia. (2)Department of Psychiatry, School of Medicine, University of Antioquia, Medellín, Colombia. (3)Department of Psychiatry Biology and Basic Science, University of Antioquia. (4)Universidad Pontificia Bolivariana. (5)Universidad Nacional de Colombia. (6)University of Antioquia. ! ! Background ! : The vast majority of patients with schizophrenia have cognitive deficits. As neuropsychological variables are more suitable for empirical research (e.a. as endophenotypes) several groups have proposed the neurocognitive subtyping of schizophrenia [1]. Once identified, these neurocognitive subtypes would permit to examine their relationships with clinical and non-clinical variables, in order to improve diagnostic accuracy, prognosis and treatment [2].! Objective: To identify empirically-based neurocognitive subtypes in patients with chronic schizophrenia and determine their association with clinical characteristics.! Methods: This is a cross-sectional study that is part of a larger research on neuropsychological endophenotypes in schizophrenia. The sample consists of 253 subjects with schizophrenia. Inclusion criteria were: age 18 to 65 years old, diagnosis of schizophrenia according to DSM-IV-TR [3] and clinical stability during the last month. Patients with hospitalization in the last month and some characteristics that could impede realization of tests or alter their results, such as illiteracy, visual or hearing disabilities, use of benzodiazepines in the past month, use of psychoactive substances (except nicotine) in the past six months, electro convulsive therapy in the past six months, significant traumatic brain injury (loss of consciousness for more than 15 minutes or neurological squeals) or neurological diseases such as epilepsy, dementia, mental retardation or other neurodegenerative disorders were excluded. ! Patients were assessed using neuropsychological tests for sustained attention, executive function, facial emotion recognition, verbal learning and working memory. In order to identify the neurocognitive subtypes of schizophrenia, a latent class analysis was performed using Latent Gold 4.5 statistical program. Once neurocognitive subtypes were identified their association with clinical characteristics was examined.! Results: We identified four neurocognitive subtypes: (a) Global Cognitive Deficit; (b) Memory and Executive Function Deficit; (c) Memory and Facial Emotion Recognition Deficit; and (d) A group Without Cognitive Deficit. Patients with the subtypes ‘Memory and Executive Function Deficit’ and ‘Global Cognitive Deficit’ had a higher frequency of male sex, unemployment, severe impairment, and good adherence to treatment than the patients with the subtype ‘Without Cognitive Deficit’. Patients with the ‘Global Cognitive Deficit’ subtype had a lower frequency of past major depressive episodes (OR 0.39; 95%CI: 0.16 to 0.97) and suicide attempts. The patients with ‘Memory and Facial Recognition Deficit’ had a higher probability of severe impairment (OR 5.52; 95%CI: 1.89 to 16.14) and of being unemployed (OR 2.43; 95%CI: 1.06 to 5.55), but also a lower probability of past depressive episodes (OR 0.21; 95%CI: 0.07 to 0.66). Patients without cognitive impairment had a history of increased affective symptomatology.! Association between demographic and clinical features ! with neurocognitive subtypes! Conclusion: Our results suggest the existence of a spectrum of cognitive impairment in subjects with schizophrenia, which is divided into four neurocognitive subtypes according to the degree and type of commitment, which in turn are related to factors of functional impairment, severity and affective symptomatology. ! ! Using neuropsychological characteristics can provide valuable information for improving classification, course assessment and treatment of schizophrenia [3].! References:! 1. Szendi I, Racsmány M, Cimmer C, Csifcsák G, Kovács ZA, Szekeres G, et al., 2010. Two subgroups of schizophrenia identified by systematic cognitive neuropsychiatric mapping. European Archives of Psychiatry and Clinical Neuroscience;260(3):257–66.! 2. Hill SK, Ragland JD, Gur RC, Gur RE., 2002. Neuropsychological profiles delineate distinct profiles of schizophrenia, an interaction between memory and executive function, and uneven distribution of clinical subtypes. Journal of Clinical and Experimental Neuropsychology;24(6):765–80.! 3. Jablensky A., 2006. Subtyping schizophrenia: implications for genetic research. Molecular Psychiatry.;11(9):815–36.! ! !Copyright © 2014 ! J. Ospina-Duque et al. e-mail: investigacionpsiquiatriaudea@gmail.com! ! P.1.j.009 Neurocognitive subtypes in patients with schizophrenia and their associated clinical features J. Ospina-Duque 1, A. Rangel 2, J. Garcia2, C. Palacio 1, E.T. Al 3 1Research Group on Psychiatry. School of Medicine University of Antioquiaa Department of Psychiatrya Medellina Colombia 2School of Medicine University of Antioquiaa Department of Psychiatrya Medellina Colombia 3Universidad de Antioquia Universidad Pontificia Bolivariana y Universidad Nacionala Departments of Psychiatry Biology and Basic Sciencea Medellina Colombia Background: The vast majority of patients with schizophrenia have cognitive deficits. As neuropsychological variables are more suitable for empirical research (e.a. as endophenotypes) several groups have proposed the neurocognitive subtyping of schizophrenia [1]. Once identified, these neurocognitive subtypes would permit to examine their relationships with clinical and non-clinical variables, in order to improve diagnostic accuracy, prognosis and treatment [2]. Objective: To identify empirically-based neurocognitive subtypes in patients with chronic schizophrenia and determine its association with clinical characteristics. Methods: This is a cross-sectional study that is part of a larger research on neuropsychological endophenotypes in schizophrenia. The sample consists of 253 subjects with schizophrenia. Inclusion criteria were: age 18 to 65 years old, diagnosis of schizophrenia according to DSM-IV-TR [3] and clinical stability during the last month. Patients with hospitalization in the last month and some characteristics that could impede realization of tests or alter their results, such as illiteracy, visual or hearing disabilities, use of benzodiazepines in the past month, use of psychoactive substances (except nicotine) in the past six months, electro convulsive therapy in the past six months, significant traumatic brain injury (loss of consciousness for more than 15 minutes or neurological squeals) or neurological diseases such as epilepsy, dementia, mental retardation or other neurodegenerative disorders were excluded. Patients were assessed using neuropsychological tests for sustained attention, executive function, facial emotion recognition, verbal learning and working memory. In order to identify the neurocognitive subtypes of schizophrenia, a latent class analysis was performed using Latent Gold 4.5 statistical program. Once neurocognitive subtypes were identified their association with clinical characteristics was examined. Results: We identified four neurocognitive subtypes: (a) Global Cognitive Deficit; (b) Memory and Executive Function Deficit; (c) Memory and Facial Emotion Recognition Deficit; and (d) A group Without Cognitive Deficit. Patients with the subtypes ‘Memory and Executive Function Deficit’ and ‘Global Cognitive Deficit’ had a higher frequency of male sex, unemployment, severe impairment, and good adherence to treatment than the patients with the subtype ‘Without Cognitive Deficit’. Patients with the ‘Global Cognitive Deficit’ subtype had a lower frequency of past major depressive episodes (OR 0.39; 95aCI: 0.16 to 0.97) and suicide attempts. The patients with ‘Memory and Facial Recognition Deficit’ had a higher probability of severe impairment (OR 5.52; 95aCI: 1.89 to 16.14) and of being unemployed (OR 2.43; 95aCI: 1.06 to 5.55), but also a lower probability of past depressive episodes (OR 0.21; 95aCI: 0.07 to 0.66). Patients without cognitive impairment had a history of increased affective symptomatology. Conclusion: Our results suggest the existence of a spectrum of cognitive impairment in subjects with schizophrenia, which is divided into four neurocognitive subtypes according to the degree and type of commitment, which in turn are related to factors of functional impairment, severity and affective symptomatology. Using neuropsychological characteristics can provide valuable information for improving classification, course assessment and treatment of schizophrenia [3]. 1. Szendi I, Racsmány M, Cimmer C, Csifcsák G, Kovács ZA, Szekeres G, et al., 2010. Two subgroups of schizophrenia identified by systematic cognitive neuropsychiatric mapping. European Archives of Psychiatry and Clinical Neuroscience;260(3):257–66. 2. Hill SK, Ragland JD, Gur RC, Gur RE., 2002. Neuropsychological profiles delineate distinct profiles of schizophrenia, an interaction between memory and executive function, and uneven distribution of clinical subtypes. Journal of Clinical and Experimental Neuropsychology;24(6):765–80. 3. Jablensky A., 2006. Subtyping schizophrenia: implications for genetic research. Molecular Psychiatry.;11(9):815–36. Citation: Eur Neuropsychopharmacol. 2014;24aSuppl 2):S324 Keywords Schizophrenia: clinical Biological markers Neurophysiology: clinical