Nucleated red blood cells in polycythemic infants
Dror Mandel, MD, Yoav Littner, MD, Francis B. Mimouni, MD, and Shaul Dollberg, MD
Tel Aviv, Israel
OBJECTIVE: This study was undertaken to evaluate whether the absolute nucleated red blood cell (RBC)
count is elevated in term, appropriate-for-gestational-age (AGA) polycythemic infants.
STUDY DESIGN: We compared absolute nucleated RBC counts taken during the first 12 hours of life in
term, AGA infants with neonatal polycythemia (n = 29), and in control, nonpolycythemic infants (n = 37). We
excluded infants of women with diabetes, hypertension, and alcohol, tobacco, or drug abuse, and those with
fetal heart rate abnormalities or low Apgar scores, hemolysis, blood loss, or chromosomal anomalies.
RESULTS: There were no differences between groups in birth weight, gestational age, or other demographic
or perinatal factors. The hematocrit, RBC count, and absolute nucleated RBC counts were significantly
higher and the platelet counts significantly lower in the polycythemic group. Regression analysis that included Apgar scores and gestational age showed a significant correlation of absolute nucleated RBC count
with the polycythemia status only (P = .017).
CONCLUSION: At birth, term AGA polycythemic infants have increased indices of active erythropoiesis. We
speculate that this finding is suggestive of subtle fetal hypoxemia. (Am J Obstet Gynecol 2003;188:193-5.)
Key words: Exchange transfusion, term infant, fetal hypoxia
Neonatal polycythemia, defined as a neonatal venous
hematocrit of 65% or greater, occurs in a sizable proportion of newborn infants. Its management is highly controversial because most randomized clinical trials have
shown little1 or no impact of dilutional exchange transfusion on neurodevelopmental outcome. Nevertheless, a
major textbook of neonatology recommends to perform
a partial dilutional exchange transfusion in all symptomatic or hypoglycemic polycythemic infants and in
asymptomatic infants with a venous hematocrit of 70% or
greater.2 The mechanisms by which the infants becomes
polycythemic are probably multiple. Neonatal dehydration can cause hemoconcentration (hypovolemic polycythemia), a situation not very likely to occur within the
first 24 hours of life. At the other end of the spectrum, hypervolemic polycythemia may follow an acute blood
transfusion to the fetus originating from the placenta
(placental-fetal transfusion), a twin fetus (twin-to-twin
transfusion), or the mother (maternal-fetal transfusion).
Finally, normovolemic polycythemia may occur in situations when erythropoiesis is enhanced by chronic fetal
hypoxia, such as happens in fetuses of diabetic mothers,3
From the Department of Neonatology, Lis Maternity Hospital, Tel Aviv
Sourasky Medical Center and the Tel Aviv University Sackler Faculty of
Medicine.
Received for publication December 31, 2001; revised March 18, 2002;
accepted July 18, 2002.
Reprint requests: Shaul Dollberg, MD, Department of Neonatology, Lis
Maternity Hospital, Tel Aviv-Sourasky Medical Center, 6 Weizman St,
Tel Aviv, 64239, Israel. E-mail: dolberg@post.tau.ac.il
© 2003, Mosby, Inc. All rights reserved.
0002-9378/2003 $30.00 + 0
doi:10.1067/mob.2003.113
or in fetal growth restriction.4 The aim of this study was to
examine hematologic indices of potential intrauterine
hypoxia, including circulating nucleated red blood cells
(RBCs), lymphocytes, and platelets5 in polycythemic and
nonpolycythemic, appropriate-for-gestational-age (AGA)
infants of nonsmoking, nondiabetic mothers. We hypothesized that higher absolute nucleated RBC and lymphocyte counts, and lower platelets would be found in
polycythemic, compared with control infants, as a consequence of subtle fetal hypoxemia.
Material and methods
We prospectively studied singleton appropriately
grown (by Lubchenco intrauterine growth charts6) term
infants (38-41 weeks’ gestation by the last menstrual period, confirmed by early ultrasound), who were born vaginally at the Lis Maternity Hospital, Tel Aviv Sourasky
Medical Center between January 1, 1998, and March 31,
1999. All infants had early (<20 seconds) cord clamping
by delivery room protocol.
In our institution, all infants undergo a routine complete blood count with a differential count obtained from
a heel stick within the first 12 hours of life for the screening of polycythemia and neonatal anemia. The protocol
requires that a spun venous hematocrit be obtained
whenever the capillary hematocrit from the heel stick is
greater than or equal to 70%. Polycythemia is then defined whenever the venous hematocrit is equal to or
greater than 65%. A preliminary (unpublished) study in
our institution showed that when the capillary hematocrit
from the heel stick is between 65% and 70%, the venous
hematocrit is never above 65%. We selected only infants
193
194 Mandel et al
January 2003
Am J Obstet Gynecol
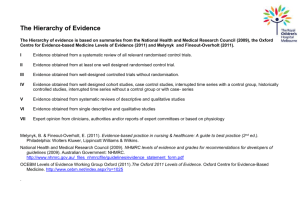
Table. Demographic and capillary heelstick blood characteristics*
Control infants
(n = 37)
Birth weight (g)
Gestational age (wk)
Sex (male/female)
Maternal age (y)
Gravidity
Parity
Epidural analgesia during labor
1-min Apgar score
5-min Apgar score
Hematocrit
RBCs (109/L)
WBCs (corrected) (109/L)
Platelets (109/L)
Absolute lymphocyte count (109/L)
Absolute nucleated RBCs (106/L)
Polycythemic infants
(n = 29)
3294 ± 442
39.3 ± 1.3
20:17
29.0 ± 5.8
2.3 ± 1.6
1.8 ± 1.0
34 (92)
9 (8-10)
10 (9-10)
60.0 ± 6.6
5.6 ± 0.7
20.3 ± 8.1
271 ± 72
6.3 ± 2.3
178 (0-588)
3104 ± 389
38.9 ± 1.5
16:13
30.6 ± 4.5
2.6 ± 2.4
2.2 ± 1.9
28 (99)
9 (8-10)
10 (9-10)
74.6 ± 3.5
7.4 ± 3.3
24.5 ± 8.3
210 ± 67
5.3 ± 2.2
330 (0-3439)
P value
NS
NS
NS
NS
NS
NS
NS
NS
NS
<.001
.008
NS
.002
NS
.02
*All data expressed as mean ± 1 SD or number (%), except the nonnormally distributed Apgar scores and absolute nucleated RBCs,
which are expressed as median (range). NS, Not significant.
with polycythemia (venous hematocrit greater than or
equal to 65%) significant enough to require partial dilutional exchange transfusion because of clinical symptoms, hypoglycemia, or because of hematocrit was greater
than 70%.2 We excluded from the study infants born to
women with gestational or insulin-dependent diabetes7;
pregnancy-induced hypertension8; abruptio placentae or
placenta previa9; any maternal heart, kidney, other lung,
or other chronic condition; drug, tobacco, or alcohol
abuse10; perinatal infections (eg, fever, leukocytosis, clinical signs of chorioamnionitis)11; any abnormality in electronic intrapartum monitoring9; or infants with low
Apgar scores (below 8 at 1 or 5 minutes).12 We also excluded infants with perinatal blood loss, hemolysis (blood
group incompatibility with positive Coombs test or hematocrit below 45%)13 or chromosomal anomalies.14
Controls were selected in the following manner: Each
time D. M. or Y. L. were on call, they screened all nonpolycythemic infants born during their call time and verified all inclusion and exclusion criteria. Each time one
infant met the entry criteria, he or she was selected to be
included in the control group. We aimed to obtain approximately 30 infants in each group, to enable the assumption of normal distribution of means.
Venous blood samples for complete blood cell counts
were collected from the infants within 12 hours of birth
and analyzed according to laboratory routine with an
STK-S counter (Coulter Corporation, Hialeah, Fla). Differential cell counts were performed manually and nucleated RBC counts were counted per 100 white blood
cells (WBCs). We showed previously that leukocyte
counts and absolute nucleated RBC numbers are not independent and traditional expression of nucleated RBCs
as their number per 100 WBCs might introduce a significant bias.3 Therefore, we expressed the number of nucleated RBCs as an absolute number rather than per 100
leukocytes, and the WBC count was expressed as corrected for the presence of nucleated RBCs.
Data are reported as mean ± SD or, for nonnormally
distributed variables as median (range). Statistical analysis included two-tailed Student t test for normally distributed variables and Kruskal-Wallis test, or Spearman
ranked correlation for nonnormally distributed variables
(such as absolute nucleated RBCs and Apgar scores) and
backward stepwise regression analysis. P < .05 was considered significant.
Our local Institutional Review Board approved the
study. Because all patients in our institution are screened
routinely for polycythemia with a complete blood count
before the age of 12 hours, the requirement for informed
consent was waived.
Results
During the study interval, there were 7576 singleton
AGA infants born at our center who met our entry criteria. Of these, 29 (0.38%) were born with polycythemia requiring partial dilutional exchange transfusion for the
above indications. There were no differences between
groups in birth weight, gestational age, maternal age,
gravidity, parity, maternal analgesia during labor, 1- and 5minute Apgar scores, and infant sex (Table). The hematologic parameters shown in the table are extracted from
the heel stick capillary blood sample obtained after birth.
As expected, the hematocrit and RBC count were significantly higher in the polycythemia group than in the control group (Table I). The absolute nucleated RBC count
was significantly higher and the platelet count significantly lower in the polycythemia group than in the
control group (Table I). There were no significant differences in lymphocyte counts or WBC counts between the
two groups. Spearman ranked correlation showed a significant relationship between absolute nucleated RBCs
Mandel et al 195
Volume 188, Number 1
Am J Obstet Gynecol
and hematocrit (r2 = 10.9%, P = .007). In backward stepwise regression analysis, taking into account polycythemia, gestational age, and the 1- or 5-minute Apgar
scores as independent variables and the absolute nucleated RBC count as the dependent variable, only polycythemia was a predictor of increased absolute nucleated
RBC count (P = .017).
Comment
We found that neonatal polycythemia is associated with
an increase in nucleated RBC counts and a decrease in
platelet counts in term AGA infants, using Lubchenco’s
curves. In our study, we excluded small-for-gestationalage infants, an important confounding variable.4 We excluded infants with other factors associated with
potentially increased absolute nucleated RBC counts, including preterm labor with histologic placental signs of
chorioamnionitis,11 hemolysis,13 chromosomal anomalies,14 maternal diabetes,7,15 and neurologic insults.16,17
We believe that our study unequivocally shows that as a
group, polycythemic infants have increased absolute nucleated RBC counts.
The mechanism by which polycythemia is associated
with increased circulating neonatal absolute nucleated
RBC counts is unknown. A likely explanation is relative
fetal hypoxia.7,18 The lymphocyte count, also believed to
be an indicator of fetal hypoxia17,19 was not elevated, but
it might be an index of acute, rather than chronic, hypoxia.7 It is worth noticing that we could not find any explanation in the literature of the pathophysiology of the
hypoxia-induced lymphocyte elevation. Nevertheless, the
platelet count was decreased in polycythemic infants,
which is consistent with the theory of shifting of the
pluripotent bone marrow stem cell toward erythropoiesis
at the expense of thrombopoiesis; in theory, another explanation would be that there is increased platelet destruction or sequestration in polycythemia, but this
phenomenon has not been studied in this disease state.
In addition, the absolute nucleated RBC count correlated
with the hematocrit.
We suggest that increased erythropoiesis contributes to
the pathophysiology of neonatal polycythemia in term,
AGA infants. Future studies comparing the neurologic
and developmental outcomes of polycythemic infants
who did or did not undergo a partial exchange transfusion should take into account the hematologic indices of
intrauterine hypoxia (ie, absolute nucleated RBC counts
as potential predictors of outcome).
REFERENCES
1. Werner EJ. Neonatal polycythemia and hyperviscosity. Clin Perinatol 1995;22:693-710.
2. Luchtman-Jones L, Schwartz AL, Wilson DB. Hematologic problems in the fetus and neonate. In: Fanaroff AA, Martin RJ, editors. Neonatal perinatal medicine. St. Louis: Mosby; 2002. p.
1204-5.
3. Green DW, Khouri J, Mimouni FB. Neonatal hematocrit and maternal glycemic control in insulin-dependent diabetes. J Pediatr
1992;120:302-5.
4. Snijders RJM, Abbas A, Melby O, Ireland RM, Nicolaides KH.
Fetal plasma erythropoietin concentration in severe growth retardation. Am J Obstet Gynecol 1993:168:615-9.
5. Hermansen MC. Nucleated red blood cells in the fetus and newborn [review]. Arch Dis Child Fetal Neonatal Ed 2001;84:F211-5.
6. Lubchenco LO, Hansman C, Dressler M, Boyd E. Intrauterine
growth as estimated from live-born birth weight data at 24 to 42
weeks gestation. Pediatrics 1963;32:793-9.
7. Green DW, Mimouni F. Nucleated erythrocytes in healthy infants and in infants of diabetic mothers. J Pediatr 1990;116:12931.
8. Sinha HB, Mukherjee AK, Bala D. Cord blood haemoglobin (including foetal haemoglobin), and nucleated red cells in normal
and toxaemic pregnancies. Ind Pediatr 1972;9:5490-3.
9. Korst LM, Phelan JP, Ahn MO, Martin GI. Nucleated red blood
cells: an update on the marker for fetal asphyxia. Am J Obstet
Gynecol 1996;175:843-6.
10. Halmesmaki E, Teramo KA, Widness JA, Clemons GK, Ylikorkala
O. Maternal alcohol abuse is associated with elevated fetal erythropoietin levels. Obstet Gynecol 1990;76:219-22.
11. Leikin E, Garry D, Visintainer P, Verma U, Tejani N. Correlation
of neonatal nucleated red blood cell counts in preterm infants
with histologic chorioamnionitis. Am J Obstet Gynecol 1997;
177:27-30.
12. Hanlon-Lundberg KM, Kirby RS. Nucleated red blood cells as a
marker of acidemia in term neonates. Am J Obstet Gynecol
1999;181:196-201.
13. Thomas RM, Canning CE, Cotes PM, Linch DC, Rodeck CH,
Rossiter CE, et al. Erythropoietin and cord blood haemoglobin
in the regulation of human fetal erythropoiesis. Br J Obstet Gynaecol 1983;90:795-800.
14. Oski FA, Naiman JL. Hematologic problems in the newborn.
2nd ed. Philadelphia: WB Saunders; 1972. p. 15-7.
15. Mimouni F, Miodovnik M, Siddiqi TA, Butler JB, Holroyde J,
Tsang RC. Neonatal polycythemia in infants of insulin-dependent diabetic mothers. Obstet Gynecol 1986;68:370-2.
16. Green DW, Hendon B, Mimouni F. Nucleated erythrocytes and
intraventricular hemorrhage in preterm neonates. Pediatrics
1995;96:475-8.
17. Naeye RL, Localio R. Determining the time before birth when ischemia and hypoxemia initiated cerebral palsy. Obstet Gynecol
1995;86:713-9.
18. Hermansen MC. Nucleated red blood cells in the fetus and newborn. Arch Dis Child Fetal Neonatal Ed 2001;84:F211-5.
19. Phelan JP, Korst LM, Ahn MO, Martin GI. Neonatal nucleated
red blood cell and lymphocyte counts in fetal brain injury. Obstet Gynecol 1998;91:485-9.