Assessing the characteristics of patients with
oral lichen planus
NW Burkhart, EJ Burker, EJ Burkes and L Wolfe
JADA 1996;127(5):648-642
10.14219/jada.archive.1996.0277
The following resources related to this article are available online at
jada.ada.org (this information is current as of January 22, 2014):
http://jada.ada.org/content/127/5/648
This article appears in the following subject collections:
Infection Control http://jada.ada.org/cgi/collection/infection_control
Information about obtaining reprints of this article or about permission to reproduce
this article in whole or in part can be found at: http://www.ada.org/990.aspx
Copyright © 2014 American Dental Association. All rights reserved. Reproduction or republication strictly
prohibited without prior written permission of the American Dental Association. The sponsor and its products
are not endorsed by the ADA.
Downloaded from jada.ada.org on January 22, 2014
Updated information and services including high-resolution figures, can be found
in the online version of this article at:
Ilk
ASSESSING THE CHARACTERISTICS OF PATIENTS
PLANUS
NANCY W. BURKHART, B.S.D.H., M.ED., ED.D.; EILEEN J. BURKER, PH.D.; E. JEFFERSON BURKES,
D.D.S., M.S.; LAURIE WOLFE, B.S.
Qrasmus Wilson, in 1869, was
the first to describe patients
who had lichen planus.1 He described the 50 patients in his
study as being in their 40s and
50s, with the majority being female. They also have been characterized as anxious, highstrung, overconscientious and
sensitive, with a tendency to
worry excessively and with periods of undue emotional stress.24
Still other studies have reported high percentages of academic, professional and intellectually oriented people among
those who have this condition.5
Although stress is commonly
considered a factor in the development and progression of oral
lichen planus, very little documentation has been presented
to substantiate this widely held
assumption. Recent studies
using instruments to assess the
mental states of these patients
have resulted in conflicting reports.6'7
However, the prevailing clinical impression is that patients
seeking dental treatment for
lichen planus lesions may be experiencing stressful situations
648 JADA, Vol. 127, May 1996
The authors assessed the medlcal history, lifestyles and health
habits of 146 patients wlth oral
lichen planus as confirmed by
biopsy. The results support a relationship between stress and
the development of oral lichen
planus. Fifty-one percent of the
subjects reported that they had
experienced stressful events at
the time of the lichen planus
onset. Practitioners may want to
consider the benefits of stress
management and bereavement
counseling in managing patients
with oral lichen planus.
in their lives. Therefore, we
designed a study to survey the
lifestyle, health habits and
demographics of a group of men
and women diagnosed with oral
lichen planus to determine if
such stressful events could be
documented.
Our sample consisted of pa-
tients whose lichen planus was
confirmed by biopsy. We documented common characteristics
of this patient population in regard to medical problems, blood
types, medications, allergies,
symptoms of their lichen planus,
health habits and demographics. Additional questions focused on life events and major
stressors that occurred at the
time of the onset of lichen
planus.
REVIEW OF THE
LITERATURE
Lichen planus. Lichen planus
is an inflammatory keratotic
disease that can affect the skin,
the oral mucosa or both. The results from studies indicate that
as many as 44 percent of subjects have reported both external and internal lesions.8'9
These lesions may be active or
in remission at any given time,
and the severity and discomfort
may vary.
According to most research
studies, the average patient
with lichen planus is of middle
age, with men and women affected in equal numbers.10 Some
Downloaded from jada.ada.org on January 22, 2014
WITH ORAL LICHEN
CLINICAL PDACTICE
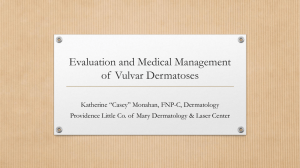
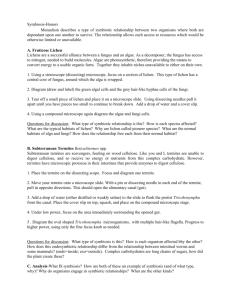
Figure 1. Black woman with reticular and erosive lesions showing ulceration in the buccal mucosa.
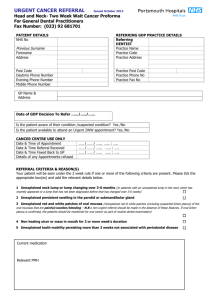
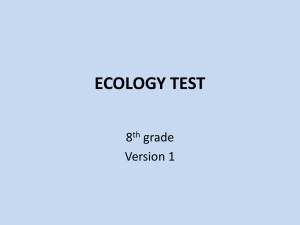
Figure 2. White woman with erosive lesion on the gingiva.
result of the actual disease.'8
Stress, too, has been implicated.
Irvine and colleagues reported
that patients believed stress to
be a major factor in the development of lichen planus. They
suggested that stress is not
easily qualified or quantified,
thus making the assessment of
stress and its importance in the
disorder difficult to analyze.'9
Management. The relation-
ship of lichen planus to squamous cell carcinoma is controversial. Patients with lichen
planus may have a higher-thannormal rate of oral malignancy.10 Because of the malignancy
controversy, considerable care
should be taken to make sure
that a diagnosis of lichen
planus is correct, and to assign
an appropriate treatment plan
that takes into consideration
JADA, Vol. 127, May 1996 651
Downloaded from jada.ada.org on January 22, 2014
studies report a slightly higher
female population.11 The disorder has been found in people of
all races, but a very high percentage of the affected people
are white.'2'13
Clinical diagnosis of lichen
planus. Andreasen (1968) divided oral lichen planus into six
clinical forms. The classification
included reticular (Figure 1),
papular, plaquelike, atrophic,
erosive (Figure 2) and bullous
types.9 Most of the lichen
planus lesions appear on the
buccal mucosa, followed by the
tongue, gingiva, lips, floor of the
mouth and palate.
The differentiation of the
type of lichen planus is important because lichen planus can
have a clinical appearance similar to that of carcinoma, as well
as to that of other oral lesions.14
The clinician must be knowledgeable about the various
forms of lichen planus to provide a differential diagnosis and
to provide the proper patient
management. An assessment
regarding the frequency of and
need for biopsies is important,
as are consultations with experts in the field.'5
Etiology. The etiology of
lichen planus is unknown; however, some evidence supports a
cell-mediated immune response
factor.'6 Other factors such as
reactions to drugs, flavoring
agents, local irritants, dental
materials and oral microorganisms have been implicated.'5
Lichen planus also has been associated with a number of medical disorders such as diabetes
and hypertension.17 Some researchers believe that lesions in
patients with diabetes and hypertension may actually be a
lichenoid reaction and may be
caused by medications used to
treat the disease, rather than a
-CLINICAL PRACIICE
TABLE I
652 JADA, Vol. 127, May 1996
oids is indicated in the erosive
forms to keep the disease in the
least erosive state.10'15
Stress, grief and disease.
Mason22 differentiated between
the arousal of the sympathetic
adrenal-medullary system by
the fight-flight response (based
on work by Selye)23 and the pituitary adrenocortical response.
It has been documented that
if the sympathetic adrenalmedullary system is activated
excessively, persistently and too
often, illness and disease may
occur. The release of catecholamines, epinephrine and
norepinephrine by the adrenal
medulla and/or sympathetic
nerve endings is believed to induce many of the pathogenic
states associated with psychological stress: increased blood
disease.31'32
Life events that produce
chronic stress have been shown
to have a wide range of effects
on the body.33 Recently a major
emphasis has been placed on
the patient's ability to cope with
the chronic stress of daily life.34
Adverse life events have also
been documented as occurring
before the onset of functional
abdominal pain, alopecia areata, headaches, cancer, heart disease, low back pain and psoria-
Downloaded from jada.ada.org on January 22, 2014
the condition's severity and
clinical appearance and the patient's specific needs. When the
diagnosis of lichen planus is
made, the practitioner should
monitor the patient at recall appointments and provide the patient with appropriate educational materials.21
Moncarz and colleagues20
suggested that practitioners
monitor lichen planus patients
at three- to six-month intervals
and attempt to resolve the condition as quickly as possible.
Most authorities believe that
lichen planus, and any such
chronic oral lesions, especially
call for correct diagnosis and
close monitoring. Erosive lesions should be biopsied more
frequently and assessed for dysplasia. The use of corticoster-
pressure, cardiac arrhythmias
and sudden death.2425
Stress and stress-related illnesses have been studied extensively in the last 20 years. The
results clearly indicate that
stress, especially chronic stress,
has profound effects on the
body. The well-known Framingham, Mass., heart study identified the type A personality and
associated it with a doubling of
the risk of coronary heart disease in men and women.26 Ani
mals subjected to repeated
stress showed significant decreases in the total number of
mononuclear cells, especially T
cells, in the spleen and blood.27
Chronic stress can cause a reduction in mitogenesis, alterations in lymphocytes, reductions
in the ratio of T-helper cells to
T-suppressor cells and an elevation in the number of natural
killer cells.28
In addition to acute and
chronic stress, the physical effects of unresolved grief have
gained attention in recent
years. Results from studies
have indicated a strong correlation between long-term, unresolved grief, high stress levels
and an increase in both cancer
and heart disease.2930 It is believed that the resulting change
in immunological functioning
may make people vulnerable to
CLINICAL PRACTICE
sis.35'36 However, as mentioned
earlier, the relationship of
stress to the development of
oral lichen planus has been
documented only sparsely.1-3'6'7
TABLE 2
METHODS
sent follow-up postcards to the
subjects who had not responded
after a two-month period.
RESULTS
Of the 299 patients with lichen
planus confirmed by biopsy,
146 subjects-101 (69 percent)
women and 45 (31 percent)
men-completed the questionnaire. Ninety-seven percent of
subjects were white, two per-
I When asked what
they thought caused
their lichen planus,
more subjects
attributed it to stress
than to any other
factor.
cent were black and 1 percent
was classified as "other." The
mean age was 57.8 with a range
of 17 to 86 years. Seventy-seven
percent of the women reported that they had undergone menopause. Subjects had
a mean educational level of 14.3
years, with years of education
ranging from seven to 32. The
majority (77 percent) of subjects
were married.
The majority of subjects (64
percent) reported having at
least some English heritage.
The next most frequently mentioned ethnicity was Irish (25
percent), followed by German
(22 percent). Only 4 percent of
subjects were Italian, followed
by 2 percent who were from
India and 0.7 percent who were
Asian.
Ninety-six of the 146 subjects
reported knowing their blood
type. The majority of subjects
had either blood type A (45 percent) or 0 (43 percent), followed
by type B (10 percent) and AB
(2 percent).
Fifty-eight percent of the
subjects said that they received
regular medical care from a
physician. The most common
medical conditions reported by
subjects are presented in Table 1.
(Subjects selected as many medical conditions as applied to
them.) In addition to medical
conditions, subjects also reported whether they were allergic to six common allergens.
JADA, Vol. 127, May 1996 655
Downloaded from jada.ada.org on January 22, 2014
Our subjects were drawn from a
series of 299 patients in the
southeastern United States
whose dentists performed biopsies on their tissue samples because of oral lesions. When the
biopsies were interpreted by
two oral pathologists at a major
teaching hospital in the Southeast, the patients were diagnosed with oral lichen planus.
We excluded patients from the
study if their biopsy did not
meet the accepted histopathologic criteria as described by
Shafer and colleagues."7
We searched for a diagnosis
of oral lichen planus in the
records of all patients who had
undergone biopsy between 1992
and 1994. We contacted the referring dentists of patients who
had had a biopsy and were diagnosed as having oral lichen
planus and asked for their permission to recruit their patients
for the present study. After the
dentist consented, we mailed a
questionnaire packet to the subject. This packet contained a
letter explaining the study, an
informed-consent form, and a
basic information questionnaire
that addressed demographic
variables such as age, marital
status and educational background, as well as information
on the subject's symptoms of
lichen planus. The packet also
contained standardized instruments to assess coping skills,
life stressors, locus of control
and level of optimism vs. pessimism. Each subject received a
stamped, addressed envelope to
use in returning the packet. We
-CL
[NICA[ POACIICE
The most commonly reported allergens were pollen (25 percent), food (10 percent), animal
dander (9 percent), trees (8 percent) and food flavoring agents
(3 percent).
Some questions pertained to
health behaviors. Thirteen percent of subjects reported that
they smoked cigarettes. Twelve
percent of subjects said that
they drank alcohol frequently,
43 percent said they drank occasionally and 45 percent said
that they did not drink at all.
The majority of subjects said
that they exercised either three
656 JADA, Vol. 127, May 1996
days per week (54 percent) or
one day per week (21 percent).
Only 25 percent of subjects said
that they did not exercise at all.
Forty percent of subjects indicated that they had seen a periodontist at some point in their
lives, and 21 percent had undergone periodontal surgery.
Twenty-nine percent of subjects
had been told by a dentist that
they grind their teeth. Thirtyseven percent of subjects indicated that they had major dental work completed before being
diagnosed with lichen planus.
Eight percent of subjects re-
DISCUSSION
The major findings of our study
were these:
- the demographic characteristics of this patient population
are consistent with those identified in previous research;
- the patients believed that
stress caused their lichen
planus;
- increased life stressors at
the time of lichen planus onset
were reported by 51.4 percent of
the patients, with the major
stressors reported as family-related stress, work-related stress
Downloaded from jada.ada.org on January 22, 2014
ported that they had been trying
a new toothpaste or mouth rinse
when the lichen planus was diagnosed.
Table 2 presents information
on the duration, frequency and
severity of the lichen planus
symptoms that the subjects
experienced. Despite the frequency and severity of the
mouth discomfort, and the medical conditions noted in Table
1, the majority of the subjects
(90 percent) rated themselves
as being in good health.
When asked what they
thought caused their lichen
planus, more subjects (37.4 percent) attributed it to stress than
to any other factor. Toothpaste
was reported as a cause by 4.8
percent, medicine by 4.1 percent
and foods by 3.4 percent; the remaining patients (50.3 percent)
reported that they did not know
the cause. When subjects were
asked to report any major lifestyle change that occurred at
the time the lichen planus first
appeared, many subjects wrote
about considerable life stress,
including loss (of a job, of loved
ones through death or divorce),
health stressors, work stress
and relationship difficulties
(Table 3).
TABLE 3
CLINICAL
and German descent (22 percent). In a number of cases, the
subjects indicated descent from
a mixture of ethnic groups. Our
study was limited to participants in a small area of the
Southeast in which certain ethnic groups are more common;
therefore, these results may not
be representative of the general
population. The small percentages of other ethnic groups (4
percent) is also seen in previous
studies, which have found small
percentages of blacks, Asians,
Indians and others with oral
lichen planus.""' Certain ethnic
I
Future research
should be directed
toward the question
of unresolved grief
and lichen planus patients' ability to deal
effectively with traumatic lffe events.
groups may be more susceptible
to specific diseases. A person in
one of these groups may be of a
specific blood type that may predispose him or her to certain disorders, such as lichen planus.
Blood type. We included the
subjects' blood type in the medical history because other researchers have reported an
association between certain diseases and disorders and particular blood types.37 ThomopoulouDoukoudakis and colleagues
found that the majority of
lichen planus patients in their
study were of the group 0 blood
type.38 Most of the subjects in
our study who knew their blood
type had either blood type A (45
percent) or type 0 (43 percent).
The distribution of the blood
groups in the general population is 45 percent type 0, 40
percent type A, 9 percent type B
and 3 percent type AB.39 Many
patients did not know their
blood type; therefore, the results from the reported 96 subjects cannot be generalized to
all oral lichen planus patients.
Since certain disorders may be
associated with various blood
types, future research should
address the possible connection
between oral lichen planus and
a specific blood group.
Overall health. The reported health and lifestyle
habits of the subjects in our
study could be considered within a normal range or below average in regard to their smoking and alcohol consumption
and above average in their exercise habits. Only 13 percent indicated that they smoked at the
time of the study. Recent statistics show that 32.0 percent of
men and 26.9 percent of women
who have had 12 years of education are smokers.40 The percentages of smokers for the
southeastern United States in
1989 were 30.4 percent for men
and 26.1 percent for women.41
Given these statistics, it appears that we had a below-average number of smokers among
our subjects. These data indicate that the patients in our
study may be more concerned
about their health and that
they may have been counseled
by practitioners about oral risk
factors. This hypothesis is further supported by data that
showed that only 12 percent of
the subjects reported consuming alcohol on a frequent basis.
Forty-five percent did not consume alcohol at all.
Stress as a cause. Although
most of the subjects did not
know what had caused the
JADA, Vol. 127, May 1996 659
Downloaded from jada.ada.org on January 22, 2014
and death-related stress.
Our study has certain limitations. First, the subjects were
patients who consented to be
part of the study. Volunteers
have specific characteristics in
comparison with non-volunteers. Second, each referring
dentist was contacted and
asked to consent to his or her
patient's being part of the
study. Some patients were
screened by the dentists and
dismissed for varying reasons
such as age or debilitating illness. Finally, the study sampled only a select geographic
area of the Southeast.
Age and education. Our
subjects were slightly older
(mean age = 57.8 years) than
subjects described in previous
research.10'11 We had a larger
number of women (69 percent)
than men in our study compared with previous studies."1"2
The data from the present
study also denote a professional
population with a mean educational level of 14.3 years (range,
seven to 32 years). In our study,
37 percent of subjects had a
high school diploma, 43 percent
had one to four years of college
education and 20 percent had
postgraduate college degrees. A
higher level of education among
patients with lichen planus is
consistent with findings reported in other studies.1'4 People who
have a higher level of education
may seek treatment for disease
more readily than people who
have less education and are in
lower socioeconomic strata;
therefore, our population may
not truly represent a cross section of the general population.
Ethnic descent. The results
of our study show a large percentage of the population to be
of English descent (64 percent)
followed by Irish (25 percent)
PRACIICE
NICAL PRACTICE-
660 JADA, Vol. 127, May 1996
usually described as chronic situations that had continued for
extended periods of time. Workrelated stress also may be interpersonal stress, and the person
may be exposed to chronic
stress by spending a major part
of the day in the stressful work
environment.
Many of the medical conditions noted by the subjects appeared to be conditions that
have been described as somewhat stress related, such as
hypertension, stomach problems, headaches, diverticulitis
and allergies. Hypertension and
arthritis were noted by 27 percent and 24 percent, respectively, of this patient population as
chronic health problems.
CONCLUSIONS
We used a survey technique to
assess the health history, lifestyles and health habits of patients who have oral lichen
planus. The research was intended to be descriptive and
was conducted to gather data on
the general characteristics of
this patient population.
These patients were of a high
professional and educational
level. A high
percentage of
subjects were
of Northern
European descent. Blood
type A appeared most
Dr. Burkhart Is an
a#astant
frequently, fol- f aqlunct
Departprofesor,
lowed by blood ment
of Dental
type 0.
University
EcoloWy,
A majority
of North Carolina
of Dentistry,
of the subjects School
CB#7460, Brauer
in our study in- Hall, Chapel Hill,
dicated that
N.C. 27599-7450.
also Is a
postthey had major She
doctoral fellow In
stressors at the oral pathology.
time of the
onset of lichen
Address
reprint requests to Dr.
Burkhart.
planus and also for periods of
time before the original diagnosis. The stress was most often
related to work, relationship
problems and various forms of
loss.
The data collected support a
relationship between stress and
oral lichen planus. A major stressor for the subjects was death of
loved ones. Future research
should be directed toward the
question of unresolved grief and
lichen planus patients' ability to
deal effectively with traumatic
life events, as well as the effects
of multiple traumatic events on
their immune system. Future
research should also address
the coping style, the effects of
stress management and the
general personality profile of
lichen planus patients. These
factors are relevant in patient
management.
The major findings of this
study clearly indicate that patients perceive a relationship
between stressful life events
and the onset and progression
of lichen planus. Subjects appeared to be cognizant of health
risk factors and seemed concerned about their own health.
The practitioner may want to
consider the benefits of stress
management and bereavement
counseling in managing the
treatment of patients with
lichen planus, and to consider
referring specific patients to the
appropriate sources. o
Dr. Burker is an assistant professor,
Departments of Medical Allied Health Professions and Psychiatry, University of North
Carolina School of Medicine, Chapel Hill.
Dr. Burkes is a professor, Oral Pathology
Section, University of North Carolina School
of Dentistry, Chapel Hill.
Ms. Wolfe is a research assistant and graduate student, Department of Medical Allied
Health Professions, University of North
Carolina School of Medicine, Chapel Hill.
The investigators welcome any inquiries or
Downloaded from jada.ada.org on January 22, 2014
lichen planus, more than 37
percent believed that their
lichen planus was caused by
stress. The subjects who reported life stressors that had occurred at the time of diagnosis
(n = 112) wrote about three
main categories of causes of
stress: death and illness, work,
and interpersonal or family
matters. The majority of the
subjects reported that several
stressful events had occurred
before the onset of the lichen
planus.
Death and illness. The death
factor usually involved the care
of sick relatives over long periods of time and the relatives'
subsequent death. Additionally,
a number of subjects reported
the death of a child. Since death
and unresolved grief are major
stressors, and the death of one's
child is considered to be one of
the most overwhelming on the
list of stressful events,42 these
subjects may have experienced
extreme amounts of what are
considered highly stressful life
events.
A few subjects also reported
unusual experiences such as
having discovered a dead body;
in two cases, in fact, the subjects had discovered mutilated
bodies. Since the questionnaire
asked the subject only about life
events that may have been
stressful during the period of
time when the lichen planus
initially occurred, it is not
known what impact traumatic
events that occurred long before
the onset of lichen planus may
have had on the present state of
the patient's health.
Interpersonal and work problems. Frequently, subjects
wrote about relationship problems with their spouses, children or co-workers. These types
of relationship problems were
-CLINICAL PRACTII
information that will benefit research on
lichen planus. Interested readers should contact Dr. Burkhart, coordinator, The Lichen
Planus Study, at the address on page 660.
662 JADA, Vol. 127, May 1996
sons with cancer referred for psychotherapy.
Psychiatr Clin North Am 1987;10(3):467-86.
30. Cottington EM, Matthews KA, Talbott
E, Kuller LH. Environmental events preceding sudden death in women. Psychosom Med
1980;42(6):567-74.
31. Zisook S, Shuchter S, Schuckit M. Factors in the persistence of unresolved grief
among psychiatric outpatients. Psychosomatics 1985;26(6):497-503.
32. Geller JL. The long-term outcome of unresolved grief: an example. Psychiatr Q 1985;
57(2):142-6.
33. Holmes TH, Masuda M. Life change and
illness susceptibility. In: Dohrenwend BS,
Dohrenwend BP, eds. Stressful life events:
their nature and effects. New York: Wiley;
1974:45-72.
34. Scheier MF, Carver CS. Optimism, coping and health: assessment and implications
of generalized outcome expectancies. Health
Psychol 1985;4(3):219-47.
35. Al'Abadie MS, Kent GG, Gawkrodger
DJ. The relationship between stress and the
onset and exacerbation of psoriasis and other
skin conditions. Br J Dermatol 1994;130(2):
199-203.
36. Jensen J. Life events in neurological patients with headache and low back pain (in
relation to diagnosis and persistence of pain).
Pain 1988;32(1):47-53.
37. Harrison GA, Weiner JS, Tanner JM,
Barnicot NA. Human biology. 2nd ed. London:
Oxford University Press; 1977:250-83.
38. Thomopoulou-Doukoudakis A, Squier
CA, Hill MW. Distribution of ABO blood
group substances in various types of oral
lichen planus. J Oral Pathol 1983;12(1):47-56.
39. Andreoli TE, Carpenter CJ, Plum F,
Smith LH. Cecil essentials of medicine. 9th
ed. Philadelphia: Saunders; 1986:368.
40. Cigarette smoking among adultsUnited States, 1993. MMWR 1994;43(50):
925-9.
41. Smoking tobacco and health-a fact
book. U.S. Department of Health and Human
Services 1989; DHHS publication no. (CDC)
87-8397.
42. Holmes TH, Rahe RH. The Social Readjustment Rating Scale. J Psychosom Res 1967;
11:213-8.
Downloaded from jada.ada.org on January 22, 2014
1. Wilson E. On leichen planus. J Cutan
Med Dis Skin 1869;3:117-32.
2. Thompkins JK Lichen planus-a statistical study of forty-one cases. Arch Dermatol
1955;71:515-9.
3. Cooke BED. The oral manifestations of
lichen planus: 50 cases. Br Dent J 1954;96
(1):1-9.
4. Cawley EP, Kerr DA. Lichen planus. Oral
Surg Oral Med Oral Pathol 1952;5(10):106976.
5. Shklar G. Lichen planus as an oral ulcerative disease. Oral Surg Oral Med Oral Pathol
1972;33(3):376-88.
6. Allen CM, Beck FM, Rossie KM, Kaul TJ.
Relation of stress and anxiety to oral lichen
planus. Oral Surg Oral Med Oral Pathol
1986;61(1):44-6.
7. Hampf BG, Malmstrom MJ, Aalberg VA,
Hannala JA, Vikkula J. Psychiatric disturbance in patients with oral lichen planus.
Oral Surg Oral Med Oral Pathol 1987;63(4):
429-32.
8. Lacy MF, Reade PC, Hay KD. Lichen
planus: a theory of pathogenesis. Oral Surg
Oral Med Oral Pathol 1983;56(5):521-6.
9. Andreasen JO. Oral lichen planus-a
clinical evaluation of 115 cases. Oral Surg
Oral Med Oral Pathol 1968;25(1):31-42.
10. Regezi JA, Sciubba J. Oral pathology:
clinical pathological correlations. 2nd ed.
Philadelphia: Saunders; 1993:114-20.
11. Axell T, Rundquist L. Oral lichen
planus-a demographic study. Community
Dent Oral Epidemiol 1987;15:52-6.
12. Brown RS, Bottomley WK, Puente E,
Lavigne GL. A retrospective evaluation of 193
patients with oral lichen planus. J Oral Pathol
Med 1993;22:69-72.
13. Silverman S Jr., Gorsky M, Lozada-Nur
F. A prospective follow-up study of 570 patients with oral lichen planus: persistence, remission, and malignant association. Oral
Surg Oral Med Oral Pathol 1985;60(1):30-4.
14. Hansen LS, Olson JA, Silverman S Jr.
Proliferative verrucous leukoplakia-a long-
term study of thirty patients. Oral Surg Oral
Med Oral Pathol 1985;60(3):285-98.
15. Jungell P. Oral lichen planus-a review.
Int J Oral Maxillofac Surg 1991;20(3):129-35.
16. Sugerman PB, Voltz MJ, Savage NW,
Basford KE, Seymour GJ. Phenotypic and
functional analysis of peripheral blood lymphocytes in oral lichen planus. J Oral Pathol
Med 1992;21(10):445-50.
17. Shafer WG, Hine MK, Levy BM. A textbook of oral pathology. 4th ed. Philadelphia:
Saunders; 1983:808-14.
18. Shiohara TL. The lichenoid tissue reaction: an immunological perspective. Am J Dermatopathol 1988;10(3):252-6.
19. Irvine C, Irvine F, Champion RH. Longterm follow-up of lichen planus. Acta Derm
Venereol 1991;71(3):242-4.
20. Moncarz V, Ulmansky M, Lustmann J.
Lichen planus: exploring its malignant potential. JADA 1993;124(3):102-08.
21. Burkhart NW. Oral lichen planus commonalities: educational and psychological implications. Dissertation Abstracts International: (0317) 1995;56-O1B, publication No.
9517788:0159.
22. Mason JW. A review of psychoendocrine
research on the sympathetic adrenal medullary system. Psychosom Med 1968;30:631-53.
23. Selye H. The physiology and pathology
of exposure to stress. Montreal: Acta Inc.;1950.
24. Markovitz JH, Matthews KA, Kannel
WB, Cobb JL, D'Agostino RB. Psychological
predictors of hypertension in the Framingham study: is there tension in hypertension?
JAMA 1993;270(20):2439-43.
25. Eliot RS, Buell JC. Role of emotions and
stress in the genesis of sudden death. J Am
Coll Cardiol 1985;5(6)(Supplement):95B-98B.
26. Castelli WP. Epidemiology of coronary
heart disease: the Framingham study. Am J
Med 1984;76(2-A):4-12.
27. Batuman OA, Sajewski D, Ottenweller
JE, Pitman DL, Natelson BH. Effects of repeated stress on T cell numbers and function
in rats. Brain Behav Immun 1990;4:105-17.
28. Bachen EA, Manuck SB, Marsland AL,
et al. Lymphocyte subset and cellular immune response to a brief experimental stressor. Psychosom Med 1992;54:673-9.
29. Vachon MLS. Unresolved grief in per-