Continuing Education: Shoulder Stability Anatomy & Kinesiology:
advertisement

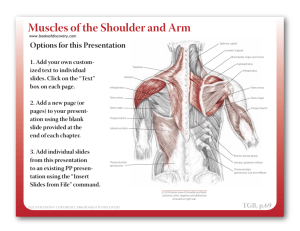
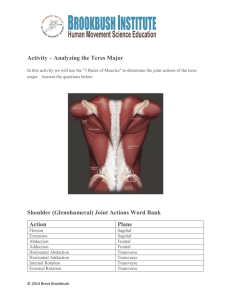
Continuing Education: Shoulder Stability Anatomy & Kinesiology: The GHJ consists of the articulation of three bones: the scapula, clavicle and humerus. The scapula has three protrusions: the coracoid, acromion and glenoid 1. These protrusions as well as the scapula itself serve as attachment sites for the ligaments and muscles that move and stabilise the GHJ 1. The ligaments of the GHJ, the superior, inferior and mid glenohumeral ligaments stabilise the GHJ while the coracoacromial, and acromioclavicuar ligaments attach to the acromion, coracoid and/or clavicle and provide stability to the scapula 2 . 1. Sternoclavicular Joint Synovial joint that articulates with 1st rib and sternal notch. • Elevation (4–60°) • Depression (5–15°) • Protraction/retraction (15°) from resting position • Rotation (30–50° posteriorly about horizontal axis) 2. Acromioclavicular Joint Formed by articulation of acromion process of scapula with acriomial end of clavicle • Upward/downward rotation • Medial (winging)/ lateral rotation) • Anterior/posterior tilting (tipping) 3. Scapulothoracic Joint Functional, not “true” joint, where the scapula articulates with convex rib cage. Motions of Scapula • Elevation/depression • Abduction/adduction • Medial/lateral rotation • Upward/downward rotation 4. Glenohumeral Joint Synovial joint where the head of humerus articulates with glenoid fossa of scapula • Flexion/extension • Abduction/adduction • Internal rotation/external rotation • Horizontal flexion/horizontal extension There are three sets of muscles influencing stability and movement of the GHJ, the periscapula muscles, rotator cuff, and other muscles that move the GHJ. The periscapula muscles (rhomboids, trapezius, levator scapula, pectoralis minor, and serratus anterior) control the positioning of the scapula 3,4. The rotator cuff (supraspinatus, infraspinatus, subscapularis and teres minor) in combination with the long head of biceps brachii (LHBB), surround the humeral head and provide stability and some movement at the GHJ 1. Through their origin on the scapula they are also influenced by the function of the periscapula muscles 4 . As individual muscles, the rotator cuff assists in various movements of the GHJ 5. Supraspinatus assists in abduction, infraspinatus and teres minor perform external rotation, and subscapularis performs internal rotation. LHBB originate on the GHJ and insert on the radius, assisting flexion of the GHJ 5. Other muscles contributing to strength and movement of the joint are deltoids, pectoralis major, latissimus dorsi, triceps brachii, biceps brachii, coracobracialis, and teres major 1,6-8. Movement Glenohumeral Prime movers Anterior deltoid Coracobrachialis Latissimus dorsi Teres major Extension Infraspinatus Posterior deltoid Deltoid (mid) Abduction Supraspinatus Pectoralis major Adduction Latissimus dorsi Infraspinatus External rotation Teres minor Subscapularis Pectoralis major Internal rotation Latissimus dorsi Teres major Infraspinatus Horizontal Teres Minor Extension Posterior Deltoid Coracobrachialis Pectoralis major Horizontal Biceps – short head Flexion Anterior Deltoid Flexion Secondary movers Pectoralis major (clavicular head) Teres minor Triceps Anterior/posterior deltoid Serratus anterior Teres major Posterior deltoid Anterior deltoid Scapular Rhomboid major/minor Trapezius Protraction Serratus anterior Trapezius (upper and lower) Upward rotation Serratus anterior (upper and lower) Downward Rhomboids (major/minor) rotation Pectoralis minor Trapezius Levator scapulae Elevation Rhomboids Latissimus dorsi Depression Pectoralis minor Retraction Pectoralis minor Latissimus dorsi Scapulohumeral rhythm: • First – – • – – • – – degrees of shoulder elevation involves a "setting phase": The movement is largely glenohumeral. Scapulothoracic movement is small and inconsistent. degrees of shoulder elevation: The glenohumeral and scapulothoracic joints move simultaneously. Ratio : of glenohumeral to scapulothoracic movement. degrees of shoulder elevation: The glenohumeral and scapulothoracic joints move simultaneously. Ratio : of glenohumeral to scapulothoracic movement. You can observe scapulohumeral rhythm by palpating the scapula's position as a person elevates the shoulder. Helpful scapular landmarks for palpation are the base of the spine and the inferior angle. Scapulohumeral rhythm serves at least two purposes: 1. The muscles do not shorten as much as they would without the scapula's upward rotation, and so can sustain their force production through a larger portion of the range of motion. 2. Because of the difference in size between the glenoid fossa and the humeral head, subacromial impingement can occur unless relative movement between the humerus and scapula is limited. Simultaneous movement of the humerus and scapula during shoulder elevation limits relative (arthrokinematic) movement between the two bones. Important Force Couples: Rotator Cuff - Deltoid Traps – Serratus Ant Integrated RC – Deltoid and Scapular Force Couples References: 1. 2. 3. 4. 5. 6. 7. 8. Browning, D. G. & Desai, M. M. Rotator cuff injuries and treatment. Prim Care 31, 807-29 (2004). Bigliani, L. U., Kelkar, R., Flatow, E. L., Pollock, R. G. & Mow, V. C. Glenohumeral stability: Biomechanical properties of passive and active stabilizers. Clinical Orthopaedics and Related Research 330, 13 - 30 (1996). Kibler, W. B. The role of the scapula in athletic shoulder function. Am J Sports Med 26, 325-37 (1998). Paine, R. M. & Voight, M. The role of the scapula. J Orthop Sports Phys Ther 18, 386-91 (1993). Sinnatamby, C. S. Last's Anatomy: Regional and Applied (Churchill Livingstone, 1999). Krabak, B. J., Sugar, R. & McFarland, E. G. Practical nonoperative management of rotator cuff injuries. Clin J Sport Med 13, 102-5 (2003). Bohmer, A. S., Staff, P. H. & Brox, J. I. Supervised exercises in relation to rotator cuff disease (impingement syndrome stages II and III): A treatment regimen and its rationale. Physiotherapy Theory and Practice 14, 93 - 105 (1998). Morrison, D. S., Greenbaum, B. S. & Einhorn, A. Shoulder impingement. Orthop Clin North Am 31, 285-93 (2000).