Pediatric Nutrition Surveillance System Report
advertisement

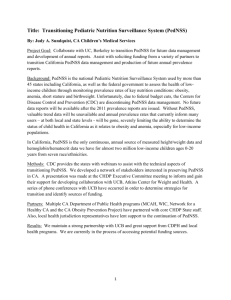
Health Status: Minnesota Children Enrolled in WIC 1997 to 2006 Data presented in this report were gleaned from the Minnesota WIC Program through the Pediatric Nutrition Surveillance System (PedNSS). Table of Contents Pediatric Nutrition Surveillance System ......................................3 Demographic Characteristics .......................................................3 Pediatric Health Indicators Low Birthweight .................................................................4 High Birthweight ................................................................5 Short Stature ......................................................................6 Underweight .......................................................................7 Overweight and Risk of Overweight ...................................8 Anemia ..............................................................................11 Breastfeeding ...................................................................12 Infant and child health advances and concerns .........................16 Pediatric Recommendations ......................................................16 References .................................................................................17 PedNSS Summary Report ~ Page 2 Pediatric Nutrition Surveillance System The Pediatric Nutrition Surveillance System (PedNSS) is a child-based public health surveillance system that monitors the nutritional status of low-income children in federally funded maternal and child health programs. In Minnesota, PedNSS includes only data from children enrolled in the Special Supplemental Food Program for Women Infants and Children (WIC). Virtually all Minnesota WIC records are included in the surveillance system. The national PedNSS includes data from other federally funded programs in addition to WIC, but is the comparable national group. Data reported here includes: birthweight, short stature, underweight, overweight, anemia, and breastfeeding. Data are collected at the clinic level, aggregated to the state level, and submitted to the Centers for Disease Control and Prevention (CDC) for analysis. The goal of PedNSS is to collect, analyze, and disseminate surveillance data to guide public health policy and action. PedNSS information is used to set priorities and plan, implement, and evaluate nutrition programs. This report summarizes 2006 data and highlights trends from 1997 through 2006 for Minnesota. Demographic Characteristics During 2006, the Minnesota WIC Program served an average monthly caseload of 129,066 participants. Among the children served during 2006, 48% were non-Hispanic white children, 19% Hispanic children, 16% non-Hispanic black children, 7% Asian or Pacific Islander children, 3% American Indian or Alaska Native children, and 6% were children of multiple or unspecified races and ethnicities. During 2000, the average monthly caseload was 90,093 participants. Among the children served during 2000, 59% were non-Hispanic white children, 13% Hispanic children, 15% non-Hispanic black children, 9% Asian or Pacific Islander children, and 4% were American Indian or Alaska Native children (Figure 1). Figure 1 Racial and ethnic distribution among among Minnesota Minnesota WIC children children aged aged <5 <5 years years for for 2000 2000 and and 2006 2006 Percentage 0 Minnesota 2006 10 20 30 40 50 60 70 80 90 100 White, not Hispanic Black, not Hispanic Hispanic American Indian Asian Multiple Minnesota 2000 2006 MN PedNSS Table 1C PedNSS Summary Report ~ Page 3 Pediatric Health Indicators Low Birthweight The single most important factor affecting neonatal mortality, and a significant determinant of postneonatal mortality, is low birthweight (< 2,500 grams). Lowbirthweight infants who survive are at increased risk for a variety of health problems, including neurodevelopmental disabilities and respiratory disorders. In Minnesota during 2006, 7.4% of WIC infants were born at a low birthweight, compared with 9.4% of infants in the National Pediatric Nutrition Surveillance system during 2005. One of the Healthy People 2010 objectives (16-10a) calls for a reduction in the incidence of low birthweight to no more than 5% of all live births.2 While the prevalence of low birthweight among Minnesota WIC infants is lower than that of the National PedNSS population, prevalence is still above the goal established for 2010. Furthermore, prevalence of low birthweight has not consistently declined over time, as shown in Figure 2 below. Variations were also observed among each of the racial and ethnic groups. Of particular concern is the higher rate of low birthweight among Black infants compared to all other racial and ethnic groups in Minnesota WIC. This difference has persisted for many years. Figure 2 Trends in prevalence of low birthweight* among children enrolled in WIC in Minnesota 1997 1997 to to 2006 2006 by by race and and ethnicity ethnicity Percentage 15 10 5 0 1997 1998 1999 2000 2001 2002 2003 2004 2005 2006 Year White * Black Hispanic < 2500 grams, among infants born during the reporting period. Year 2010 target: reduce low birthweight to 5% of live births. American Indian Asian Total 2006 MN PedNSS Table 18C PedNSS Summary Report ~ Page 4 High Birthweight High birthweight (> 4,000 grams) also puts infants at increased risk. Infants born at high birthweight are at increased risk for birth injuries, such as shoulder dystocia, and death. Of infants participating in Minnesota WIC in 2006, 9.1% were born at a high birthweight, compared with 6.6% in the National PedNSS population (2005). High birthweight is one of the health indicators in which Minnesota WIC infants fare less well than their national peers. The prevalence of high birthweight has decreased somewhat among Minnesota WIC infants in the ten years from 1997 (10.4%) to 2006 (9.1%). As with low birthweight, the risk of high birthweight is greater among some racial and ethnic groups than others. For example, the rates of high birthweight are higher among Native American children than among other children enrolled in WIC in Minnesota. This difference has persisted over time (Figure 3). Because high birthweight may be indicative of gestational diabetes, it is important to monitor high birthweight. Gestational diabetes is associated with future health problems for the child, in particular obesity and diabetes. Figure 3 Trends in prevalence of high birthweight*among children enrolled in WIC in Minnesota 1997 1997 to to 2006 2006 by by race race and and ethnicity ethnicity Percentage 20 15 10 5 0 1997 1998 1999 2000 2001 2002 2003 2004 2005 2006 Year White * Black Hispanic > 4000 grams, among infants born during the reporting period. American Indian Asian Total 2006 MN PedNSS Table 18C PedNSS Summary Report ~ Page 5 Short Stature Short stature (low length or height, for age) may reflect the long-term health and nutritional status of a child or a population. Although short stature can be associated with parent’s short stature, or with low birthweight, it can also result from growth retardation due to chronic malnutrition caused by inadequate food intake, recurrent illness, or both. In the Minnesota WIC population during 2006, 5.1% of children birth to age 5 were of short stature, compared with 2.3% of U.S. children (unpublished data, Dr. Zuguo Mei, CDC, 2003). However, the prevalence of short stature in Minnesota’s WIC population is about what would be expected at a population level (5%), and nearly meets the Healthy People 2010 objective (19-4) to reduce to 5%2 growth retardation among low-income children less than 5 years of age. The prevalence of short stature among all MN WIC children has declined over the past 10 years from 5.7% (1997) to 5.1% (2006). While there has been a slight decrease in short stature among most racial and ethnic groups, among Asian or Pacific Islander children the decrease had been dramatic until 2004 when the prevalence in this group increased markedly (Figure 4). This corresponds to an influx of new Asian immigrants when the last of the refugee camps in Laos were closed. Figure 4 Trends in prevalence of short stature*among children enrolled in WIC in Minnesota among among children children aged aged <5 <5 years, years, by by race race and and ethnicity ethnicity 1997 to 2006 Percentage 15 10 5 0 1997 1998 1999 2000 2001 2002 2003 2004 2005 2006 Year White * Black Hispanic American Indian Asian Total < 5th percentile length or height-for-age, CDC Growth Charts, 2000. Year 2010 target: reduce growth retardation (short stature) among low-income children under age five years to 5%. 2006 MN PedNSS Table 18C * Short Stature is defined using the 2000 CDC growth chart percentiles of less than the 5th percentile length-for age for children younger than 2 years of age and less than the 5th percentile height-for-age for children 2 years of age or older. PedNSS Summary Report ~ Page 6 Underweight Data on underweight* children from birth to age 5 indicate that acute malnutrition (inadequate calories) is not a public health problem in the Minnesota WIC population. The prevalence of 3.0% among MN WIC children in 2006 is below the expected prevalence of 5%. The prevalence of underweight for U.S. children in this age group is 4.8% (unpublished data, Dr. Zuguo Mei, CDC, 2003). The prevalence of underweight for all Minnesota WIC children decreased from 4.2% in 1997 to 3.0% in 2006 (Figure 5). The highest prevalence of underweight during 2006 was among Black children at 4.2%. Additionally, during 2006, 5.2% of Black infants were underweight, which might be associated with the higher rate of low birthweight in this group, and may also contribute to the overall higher rate of underweight among Black children. Figure 5 Trends in prevalence of underweight* among children enrolled in WIC in Minnesota among among children children aged aged <5 <5 years, years, by by race race and and ethnicity ethnicity 1997 1997 to to 2006 2006 Percentage 10 5 0 1997 1998 1999 2000 2001 2002 2003 2004 2005 2006 Year White * Black Hispanic American Indian < 5th percentile weight-for-length or BMI-for-age, CDC Growth Charts, 2000. 5% of children are expected to fall below the 5th percentile. Asian Total 2006 MN PedNSS Table 18C * Underweight is defined using the 2000 CDC growth chart percentiles of less than the 5th percentile weight-for-length for children younger than 2 years of age and less than the 5th percentile BMI -for-age for children 2 years of age or older. † To calculate BMI (body mass index): Weight (kg) ÷ Stature (cm) ÷ Stature (cm) x 10,000 or Weight (lb) ÷ Stature (in) ÷ Stature (in) x 703. PedNSS Summary Report ~ Page 7 Overweight and Risk of Overweight The prevalence of overweight* in children and adolescents has reached epidemic proportions in recent years. In Minnesota WIC children in 2006, the prevalence of overweight among children birth to age 5 was 12.1%. Overweight in children younger than age 2 does not pose the same risk as it does for children aged 2 and older, because only a weak association has been found between the weight status of children less than two years of age and adult obesity.3 Expert committees have recommended distinguishing between two levels of risk in children aged 2 years or older: overweight is defined as a BMI-for-age >95th percentile, and at risk of overweight as a BMI-for-age between the 85th and 95th percentiles.4-6 With the exception of white children, the prevalence of overweight by racial and ethnic groups in the Minnesota WIC population is comparable to or greater than the prevalence in these groups nationwide. American Indian children in the Minnesota WIC Program have higher rates of overweight than American Indian children in the national sample (Figure 6). Figure 6 Prevalence of overweight* among children enrolled in WIC in Minnesota 2006 among among children children aged 2 to 5 years, by race race and and ethnicity ethnicity compared to to National National PedNSS 30 Percentage 25 20 15 10 5 Expected rate 5% 0 White Black Hispanic American Indian MN WIC 2006 * Asian Multiple Total National PedNSS 2005 > 95th percentile weight-for-length or BMI-for-age, CDC Growth Charts, 2000. 5% of children are expected to fall above the 95th percentile. 2006 MN PedNSS Table 8C * Overweight is defined using the 2000 CDC growth chart percentiles of greater than or equal to the 95th percentile BMI-for-age for children 2 years of age or older. PedNSS Summary Report ~ Page 8 In the Minnesota WIC population, the prevalence of overweight in children aged 2 to 5 years increased slightly but steadily between 1990 (8.3%) and 2004 (13.8%) (Figure 7). However, beginning in 2005 the prevalence began to decline slightly: in 2005 13.3%, and in 2006 13.1%, of Minnesota WIC children had BMI values ≥ 95th percentile for age and gender. While the change is relatively small and the time period may be too short to constitute a “trend”, this is a positive development, and has been observed in other states. National PedNSS data for overweight children aged 2 to 5 years, has shown a leveling off during this time frame. Overweight in children is a concern for all race ethnic groups in Minnesota WIC, but is of particular concern among American Indian children, in which 25.0% were overweight in 2006. The prevalence of overweight in American Indian children has been consistently higher than in other groups, and the recent decrease in prevalence among other groups has not been observed among American Indian children. Figure 7 Trends in prevalence of at risk of overweight Percentage among among children children aged aged 22 to to <5 <5 years, years, by by race race and and ethnicity 30 25 20 15 10 5 0 1997 1998 1999 2000 2001 2002 2003 2004 2005 2006 Year White * Black Hispanic American Indian > 85th-<95th percentile BMI-for-age, CDC Growth Charts, 2000. 10% of children are expected to fall between these percentiles. Asian Total 2006 MN PedNSS Table 18C * Overweight is defined using the 2000 CDC growth chart percentiles of greater than or equal to the 95th percentile weight-for-length for children less than 2 years of age and greater than the 95th percentile BMI-for-age for children 2 years of age or older. Similarly, in the Minnesota WIC population of children aged 2 to 5 years, the prevalence of risk of overweight (85th to 95th percentile) increased from 15.5% in 1997 to 16.5% in 2006. Among American Indian children, the prevalence of risk of overweight was 23.9%, in 2006. As is true with overweight, the prevalence of risk of overweight has been higher among American Indian children than in all other groups. PedNSS Summary Report ~ Page 9 Similar to the National PedNSS data, prevalence of overweight increases with increasing age among children participating in Minnesota WIC (Figure 8). Children at 4 years of age are more likely to be overweight than younger children. Because the association between childhood overweight and adult overweight increases with children’s age, this trend is particularly troublesome. Figure 8 Prevalence of overweight and risk of overweight* among children enrolled in WIC in Minnesota 2006 among among children children aged aged 22 to <5 years, years, by by age Percentage 40 30 20 10 0 2 3 4 Total-State Total-Nation Age (years) Overweight * Risk of overweight Overweight: > 95th percentile BMI-for-age; at risk of overweight: > 85th-<95th percentile BMI-for-age, CDC Growth Charts, 2000. 15% of children are expected to fall above the 85th percentile (5% above the 95th percentile and 10% between the 85th and 95th percentiles). 2006 MN PedNSS Table 8C The “picture” of childhood overweight seen in both Minnesota and National PedNSS data, is similar to that of all U.S. children aged 2 to 5 years. In previous editions of this report, the rate of overweight was much greater among Minnesota children enrolled in WIC than among all children in the U.S. However, more recently, the prevalence of overweight in children enrolled in Minnesota WIC (13.1%) is less than that (13.9%) for all U.S. children aged 2 to 5 years (from NHANES 2003 – 2004).7 PedNSS Summary Report ~ Page 10 Anemia Anemia (low hemoglobin/hematocrit) is an indicator of iron deficiency, the most common nutrient deficiency worldwide. Iron deficiency in children is associated with developmental delays and behavioral disturbances. In 2006, the prevalence of anemia among children in the Minnesota WIC program was 11.6%, compared with 2.8% for all U.S. children the same age (unpublished data, Dr. Zuguo Mei, CDC, 2003). The highest prevalence of anemia in both Minnesota WIC and National PedNSS population is in children younger than 2 years of age. In the National PedNSS population as a whole, the prevalence of anemia decreased from 1996 to 2005. More recently, the prevalence of anemia has increased. A similar trend has been observed in the Minnesota WIC population. As with other health indicators, the prevalence of anemia varies between racial and ethnic groups. Compared with other racial/ethnic groups, Black children enrolled in the Minnesota WIC program have the highest rate of anemia (Figure 8). Among Black or African American children in Minnesota WIC, 19.8% are anemic compared to 8.4% of the White non-Hispanic children. Figure 8 Trends in prevalence of anemia* among children enrolled in WIC in Minnesota 1997 to 2006 among children aged <5 years, by race and ethnicity Percentage 25 20 15 10 5 0 1997 1998 1999 2000 2001 2002 2003 2004 2005 2006 Year White * Black Hispanic American Indian Hb or Hct < 5th percentile, CDC MMWR vol. 47 (No. RR-3), 1998. Asian Total 2006 MN PedNSS Table 18C * Anemia is defined using the CDC MMWR Vol. 47 (No. RR3), 1998 as hemoglobin or hematocrit measures less then the 5th percentile. Children aged 1 to 2 years are considered anemic if their hemoglobin (Hb) concentration is less than 11.0 g/dL or their hematocrit (Hct) level is less than 33.0%; children aged 2 to 5 years are considered anemic if their Hb concentration is less than 11.1 g/dL or their Hct level is less than 33.3%. 8 PedNSS Summary Report ~ Page 11 Breastfeeding The benefits of breastfeeding -- nutritional, immunologic, allergenic, economic, and psychologic -- are well known and widely recognized. As such, the Healthy People 2010 objective (16-19a-c) is to increase the proportion of children who were breastfed in the early postpartum period (referred to as “ever breastfed”) to 75%; to increase the proportion of children still breastfeeding at 6 months to 50%; and to increase the proportion of infants breastfed at 1 year to 25%. In Minnesota in 2006, 71% of WIC infants initiated breastfeeding. Of the infants who initiated breastfeeding, 32.6% were breastfed for at least 6 months; and 19.2% were breastfed for at least 12 months. National data from other sources indicate that, 70.1% of U.S. infants initiated breastfeeding; 33.2% were still breastfeeding at 6 months, and 19.7% at 12 months.9 Breastfeeding initiation in Minnesota WIC infants is similar to rates nationally, and close to the 2010 goal. In 2006, the rates of initiation among Hispanic and non-Hispanic Black infants in Minnesota WIC met or exceeded the 2010 goals (Figure 9). Figure 9 Percentage of infants ever breastfed* among infants enrolled in WIC in Minnesota 2006 Percentage by by race race and and ethnicity ethnicity 100 90 80 70 60 50 40 30 20 10 0 Year 2010 target** White Black Hispanic American Indian State Asian Multiple Total Nation * Among infants born during the reporting period. ** Increase the proportion of mothers who breastfeed their babies in the early postpartum period to 75%. 2006 MN PedNSS Table 9C PedNSS Summary Report ~ Page 12 Among Minnesota WIC children, the prevalence of initiating breastfeeding has increased from 57.6% in 1997 to 72.9% in 2006. Increasing rates of breastfeeding initiation are evident among all racial and ethnic groups (Figure 10). Figure 10 Trends in the percentage of MN WIC infants ever breastfed* 2006 Percentage by by race race and and ethnicity ethnicity 100 90 80 70 60 50 40 30 20 10 0 2010 Target = 75% 1997 1998 1999 2000 2001 2002 2003 2004 2005 2006 Year White American Indian 2010 Goal Black Asian Hispanic Total * Reported by mother at postpartum visit. Year 2010 target: increase the proportion of mothers who breastfeed their babies in the early postpartum period to 75%. 2006 MN PNSS Table 23C PedNSS Summary Report ~ Page 13 During 2006, none of the groups in Minnesota WIC met the 2010 target of 50% infants still breastfeeding at six months. However, Hispanic and non-Hispanic White and nonHispanic Black children participating in the Minnesota WIC Program are more likely to breastfeed until six months than their national counterparts (Figure 11). Figure 11 Percentage of MN WIC infants breastfed at least 6 months* 2006 by race race and and ethnicity 70 Percentage 60 Year 2010 target** 50 40 30 20 10 0 White Black Hispanic American Indian State Asian Multiple Total Nation * Among infants who turned six months of age during the reporting period. ** Year 2010 target: increase the proportion of mothers who breastfeed their babies at six months to 50%. 2006 MN PedNSS Table 9C PedNSS Summary Report ~ Page 14 Rates of long-term breastfeeding are better among Minnesota WIC infants than among the national PedNSS sample. In the Minnesota WIC population, both Hispanic and nonHispanic Black children met the 2010 goal that 25% of infants who initiated breastfeeding would continue breastfeeding until at least 12 months of age (Figure 12). Figure 12 Percentage of MN WIC infants breastfed at least 12 months* 2006 by race race and and ethnicity 70 Percentage 60 50 40 Year 2010 target** 30 20 10 0 White Black Hispanic American Indian State Asian Multiple Total Nation * Among infants who turned twelve months of age during the reporting period. ** Increase the proportion of mothers who breastfeed their babies at one year to 25%. 2006 MN PedNSS Table 9C It is interesting to note that while nationally Black infants in the PedNSS were the least likely to breastfeed, in the Minnesota WIC population they are second most likely to breastfeed. This positive pattern persists through the six and twelve month mileposts (Figures 9, 10 and 11). The higher rates of initiating breastfeeding and the longer duration among Black women in the Minnesota WIC population may reflect recent changes in Minnesota demographics, with an increasing proportion MN Black women being immigrants from Africa. Based on Minnesota birth certificate information, 47% of the women identified as African American on the birth certificate, were “foreign born” in 2005, while only 14% were “foreign born” in 1995. PedNSS Summary Report ~ Page 15 Infant and Child Health Advances and Concerns Low-Birth-weight: No clear trend toward improvement can be seen among infants enrolled in the WIC program in Minnesota. In 2006 none of the racial or ethnic groups met the 2010 goal of < 5% of infants born at low-birth-weight. Additionally, low-birthweight continues to be disproportionally high among non-Hispanic Black or African American WIC enrollees (9.7%) compared to all Minnesota WIC infants (7.4%). High-Birth-weight: There are higher rates of high-birth-weight among Minnesota WIC participants than among the National PedNSS population. Only Asian children in Minnesota are below the expected rate of 5%. American Indian children have much higher rates of high-birth-weight (15.8% in 2006) putting them at higher risk for birth injuries and death. Overweight: Overweight is a major public health problem in Minnesota, as it is nationally. Some good news was seen in data for 2005 and 2006, reflecting a stabilization of the rates of overweight among the Minnesota WIC population. Until 2005 there had been small but consistent increases each year beginning in 1987, when 8.1% of children were overweight. In 2004 the rate was 13.8%; in 2005 13.3%, and in 2006 it was 13.1%. This rate is still well above the expected rate of 5%, and as is true with other health indicators, there are disparities among different race and ethnic groups. In Minnesota during 2006, 25% of American Indian children enrolled in WIC were overweight (≥ 95th percentile BMI for age and gender). This is five times the expected rate of 5%. In the Minnesota WIC population of children, rates of overweight increase with each year of age. This is worrisome since the likelihood of overweight persisting into adulthood increases with children’s age. Anemia: The rates of anemia among Minnesota children enrolled in WIC are above the expected 5% for all race and ethnic groups. Since 2002 there has been a gradual increase in anemia among Minnesota WIC children. Additionally the rate of anemia among Black non-Hispanic or African American children in Minnesota WIC is much higher (19.1%) than that of White not-Hispanic children (8.4%). Breastfeeding: The bright spot in the 2006 PedNSS data for Minnesota is the trend in breastfeeding. Both initiation and duration are improving in Minnesota WIC children. In 2006 initiation rates for Black not-Hispanic or African American and Hispanic children met the 2010 goal that 75% of children be breastfed. Additionally, the breastfeeding duration trends are improving. 35 Pediatric Nutrition Recommendations The Minnesota PedNSS data indicate that national and state public health programs are needed to support the following actions: • Implement innovative strategies to reverse the rising trend of overweight in young children by increasing breastfeeding, increasing physical activity, promoting increased consumption of fruits and vegetables, and decreasing television viewing. • Promote and support breastfeeding through medical care systems, work sites, and communities. PedNSS Summary Report ~ Page 16 • Promote adequate dietary iron intake and the screening of children at risk for iron deficiency. • Prevent low birthweight by providing preconception nutrition care and outreach activities to promote early identification of pregnancy and early entry into comprehensive prenatal care, including the Special Supplemental Nutrition Program for Women, Infants, and Children (WIC) and the Title V Maternal and Child Health Program. References 1. Martin JA, Hamilton BE, Sutton PD, Ventura SJ, Menacker F, Munson ML. Births: final data for 2002. National Vital Statistics Reports 2003; 52(10):1-114. Available at http://www.cdc.gov/nchs/data/nvsr/nvsr52/nvsr52_10.pdf. 2. U.S. Department of Health and Human Services. Healthy People 2010. 2nd edition. Two volumes. Washington, DC: U.S. Government Printing Office; 2000. Available at http://www.healthypeople.gov/Publications/. 3. Whitaker RC, Wright JA, Pepe MS, Seidel KD, Dietz WH. Predicting obesity in young adulthood from childhood and parental obesity. New England Journal of Medicine 1997;337(13):869-873. 4. Bellizzi MC, Dietz WH. Workshop on childhood obesity: summary of the discussion. American Journal of Clinical Nutrition 1999;70(1):173S-175S. 5. Barlow SE, Dietz WH. Obesity evaluation and treatment: expert committee recommendations. Pediatrics (serial online)1998;102(3):e29. 6. Himes JH, Dietz WH. Guidelines for overweight in adolescent preventive services: recommendations from an expert committee. The Expert Committee on Clinical Guidelines for Overweight in Adolescent Preventive Services. American Journal of Clinical Nutrition 1994;59(2):307-316. 7. Ogden CL, Flegal KM, Carroll MD, Johnson CL. Prevalence and trends in overweight among U.S. children and adolescents, 1999-2000. Journal of the American Medical Association2002;288(14):1728-1732. 8. Centers for Disease Control and Prevention. Recommendations to prevent and control iron deficiency in the United States. Morbidity and Mortality Weekly Report Recommendations and Reports 1998;47(RR-3):1-30. 9. Mothers Survey, Ross Products Division, and Abbott Laboratories. Breastfeeding Trends Through 2002. Columbus, OH: Abbott Laboratories; 2003. 10. U.S. Public Health Service. Healthy People 2000: National Health Promotion and Disease Prevention Objectives. Washington, DC: U.S. Department of Health and Human Services, Public Health Service; 1991. Publication No. PHS 91-50212. PedNSS Summary Report ~ Page 17 11. American Academy of Pediatrics Committee on Nutrition. Policy statement. Prevention of pediatric overweight and obesity. Pediatrics (serial online) 2003; 112(2):424-430. 12. United States Department of Agriculture, Economic Research Service. Nutrition and Health Characteristics of Low-Income Populations: Volume II, WIC Program Participants and Nonparticipants. Chapter Five: Health Status, Conditions and Risks. December 2004. Nancy Cole and Mary Kay Fox. Publication No. E-FAN-04-010-2 PedNSS Summary Report ~ Page 18