Propofol exerts its anti-inflammatory effect in Alveolar type II
advertisement

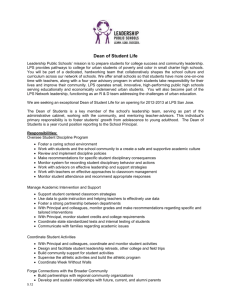
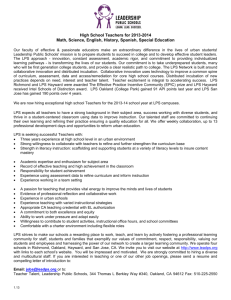
1 Propofol exerts its anti-inflammatory effect in Alveolar type II epithelial cells through downregulation of CD14 and TLR4 expression Ling Ma, Weimin Chen, Xiuying Wu, Lingxin Meng, Yuji Fujino Authors: Ling Ma, M.D.1, Xiuying Wu, M.D, Ph.D2, Weimin Chen, M.D, Ph.D3, Yuji Fujino, M.D, Ph.D 4 1. Lecturer, Department of Anesthesiology, Shengjing Hospital of China Medical University, Shenyang, China 2. Associate Professor, Department of Anesthesiology, Shengjing Hospital of China Medical University, Shenyang, China 3. Professor, Department of Anesthesiology, Shengjing Hospital of China Medical University, Shenyang, China 4. Associate Professor, Department of Anesthesiology and Intensive Care Medicine, Osaka University Medical School, Osaka, Japan Corresponding author: Weimin Chen. Mailing address: Department of Anesthesiology, No.36 Sanhao Street, Heping District, Shenyang, 110004, China. Phone: +86-13386861177 Email: chenwm@sj-hospital.org Running title: propofol and alveolar type II epithelial cell 2 Summary Background: We investigated whether LPS induced inflammation in ATII is through CD14 and TLR4 and the effect of different dosage of propofol on the inflammation in primary cultured rat alveolar epithelial type II (ATII) cells. Methods: The cultured ATII cells were randomly assigned to one of the following five groups: Group C: AT II cells in untreated group (control) was cultured in the absence of propofol and LPS; Group LPS: treated with 1μg. -1ml LPS; Group P1: treated with 1μ.ml-1 LPS and 25μM propofol; Group P2: treated with 1μg.ml-1 LPS and 50μM propofol; Group P3: treated with 1μg.ml-1 LPS and 100μM propofol. ATII cells in untreated and propofol control groups were cultured at 37°C for 3 h. CD14 and TLR4 mRNA were detected using real-time PCR. Western blot were used to detect CD14 and TLR4 protein expression. CD14 and TLR4 expression on the AT II cells were imaged using immunofluorescence. TNF-α using ELISA kit. Results: LPS stimulation resulted in an increased CD14 and TLR4 expression and increased TNF-α production in AT II cells. Propofol, at concentrations 50 µM, significantly (P < 0.05) and dose-dependently decreased CD14 and TLR4 mRNA expression and protein expression in AT II cells. This was accompanied by decreases in TNF-α production (P < 0.05). Conclusion: These results suggest that propofol, at clinical relevant concentrations, can reduce inflammatory response in LPS-induced AT II cells injury through downregulation of CD14 and TLR4 expression. Key words: propofol; alveolar type II epithelial cell; CD14; Toll like receptor-4 3 Introduction: The lung represents a site for the invasion of various bacteria or bacterial products. Along with alveolar macrophages, pulmonary epithelial cells are the first cells to be challenged by pathogenic microorganisms. rat alveolar epithelial type II (ATII) cells synthesize and secrete surfactant, control the volume and composition of fluid in the alveolar space, and proliferate and differentiate into alveolar type I epithelial cells after lung injury to maintain the integrity of the alveolar lining 1,2. Recently, there have been publications reporting the involvement of ATII in modulating the development of inflammatory reactions within the alveolus3. ATII secrete chemokines in response to inflammatory stimuli in vitro, suggesting a potential physiologic role in acute inflammatory lung injury 4, 5. Lipopolysaccharide (LPS) triggers a physical association between cluster of differentiation 14 (CD14) and Toll like receptor 4 (TLR4) 6, 7. Inflammatory response to endotoxin is largely mediated through CD14 and TLR4 8, 9. The activation of CD14 and TLR4 leads to proinflammatory cascade including the expression of proinflammatory mediators, such as TNF-α. CD14 and TLR4 have been found on ATII 10,11and could thus play an important role in the innate immune response at the alveolar surface area. Little is known about the interaction of generally used intravenous anesthetic propofol (2, 6-diisopropylphenol) with AT II. Our goal is to investigate whether LPS induced inflammation in ATII is through CD14 and TLR4 and the effect of different dosage of propofol on the inflammation. Methods and Materials Isolation of alveolar epithelial cell and primary culture ATII were isolated from male SPF degree Wistar rats (180-250g), following the protocol according to the method of Richard et al 12. Briefly, after intraperitoneal sodium pentobarbital (60 mg.kg-1) and heparin (400U.kg-1), the thoracic cavity was opened and the inferior vena cava was cut. The lungs were perfused via the right atrium with sterile saline and inflated simultaneously with air. After removal from the thoracic cavity, they were washed 6 times with normal saline and digested enzymatically with typsin. The lungs were then minced in fetal bovine serum (FBS) and DNase I (Roche), and the resulting suspension was filtered through 150μm and 30 μm mesh once. The cell mixture was purified by centrifugation on a discontinuous Percoll gradient (density 1.089 and 1.04, 400 g, 20 min). The interface was collected and after rewashing the cells were seeded onto 6-well culture dishes at a 4 density of 1×106 cells/dish in Dulbecco's modified Eagle medium (DMEM) with 10% inactivated FBS, penicillin (100U.ml-1), streptomycin (100 μg.ml-1) at 37℃ in the humidified atmosphere of 95% air/5% CO2 and cultured for 18-20 hours. Characterization of type II pneumocyte Alkaline Phosphatase Histochemical Staining Alkaline phosphatase staining served to identify ATII cells in primary cultured cells grown on glass coverslips. Briefly, the cells were fixed for 15 min at room temperature in 4% paraformaldehyde solution, rinsed for 1 min in distilled water, and air-dried. Fixed cells were incubated with BCIP/NBT stain (Sigma Chemical, St Louis, Mo) for 10 min at room temperature. The samples were then rinsed with distilled water for 1 min and air-dried. The cells were counterstained with 0.1% neutral red solution (Sigma) for 1 min at room temperature, rinsed for 1 min, air-dried, and photographed under light microscopy. Blue staining identified cells with high alkaline phosphatase activity, whereas other cells, such as macrophages, were counterstained in red. Transmission electron microscopy Cells were fixed in 2.5% glutaraldehyde, washed three times in 0.1M phosphate buffered saline (PBS) and serially dehydrated in acetone and embedded in Epon 812. Ultrathin sections (70 nm) were examined with a transmission electron microscope (JEM-1200EX, JEOL, Tokyo, Japan). Experimental design The cultured ATII cells were randomly assigned to one of the following five groups: Group C: AT II cells in untreated group (control) was cultured for 3 h in the absence of propofol (AstraZeneca, Basiglio, Italy) and LPS (E. Coli O55: B5, Sigma); Group LPS: treated with 1μg. -1ml LPS for 3 h; Group P1: treated with 1μ.ml-1 LPS and 25μM propofol for 3 h; Group P2: treated with 1μg.ml-1 LPS and 50μM propofol for 3 h; Group P3: treated with 1μg.ml-1 LPS and 100μM propofol for 3 h. Real Time PCR Total RNA was extracted by TRIzol reagent (Invitrogen, Carlsbad, CA). Real time PCRs were conducted with SYBR PrimeScriptTM RT-PCR kit (Cat. no. DRR063S, TaKaRa Biotechnology, Dalian, China) according to the manufacturer’s instructions. Briefly, total RNA (500 ng) was reverse-transcribed into cDNA using 0.5μl PrimeScript RT Enzyme Mix I, 0.5μl Random 6 mers. Quantitative real time PCR was done using an ABI PRISM® 7500 Real-Time PCR System (PE Applied Biosystems, Foster City, CA). The reactions were carried out on 5 multiple 8-well stripes. GAPDH was amplified on the same plates and used to normalize the data. The reaction volume was 25μl containing 12.5μl of the SYBR Premix EX Taq, 0.5μl of ROX reference Dye II, 2.5μl each of 2μM forward and reverse primers,5μl of RNase free water, and 2μl of the cDNA samples. Real-time PCRs were performed in triplicate for each sample and at least 3 different sets of cell preparations were used. The thermal cycling conditions used were: 95℃ for 10 s followed by 40 cycles at 95℃ for 5 s, 60℃ for 34 s. PCR products were heated to 95℃ for 15s, annealed at 60℃ for 1 min and then heated from 60℃ to 95℃ for 15 s to obtain melting curve. Dissociation curve analysis was performed for each gene to ensure the specificity of PCR products. Serial dilutions (10-fold) of one of the samples were used to generate the standard curve for each PCR. All sense and antisense primers were supplied by Sangon (Shanghai, China). The oligonucleotides primers used for real-time PCR were: rat CD14: forward ATTCCCGACCCTCCAAGT; reverse CCAGCAGTATCCCGCAGT; rat TLR4: forward GAGGACTGGGTGAGAAACGA; reverse GAAACTGCCATGTCTGAGCA; rat GAPDH: forward ATGTTCCAGTATGACTCCACTCACG; reverse GAAGACACCAGTAGACTCCACGACA. Immunoblotting Cells were lysed using a commercially available kit (KGP250; Nanjing Keygen Biotech Co. Ltd., Nanjing, China). Protein concentration was determined using the EasyQuant protein assay kit (Cat. no. DQ 101, TransGen Biotech Co. Ltd., Beijing, China) and boiled for 5 min at 100℃. Each vessel homogenate was diluted with PBS to obtain the same protein concentration. Then 20 μg of protein per lane was separated on a 10% SDS-polyacrylamide gels and transferred to a nitrocellulose membrane (Bio-Rad, Hercules, CA). The transfers were blocked overnight with 5% dry skim milk power. The membranes were incubated with anti-CD14 (sc-9150), anti-TLR4 (sc-16240) or anti-β-actin (sc-47778; all Santa Cruz Biotechnology, CA) antibodies at 1:200 dilutions for 2 h at 37℃. After being washed in PBS 3 times, the membranes were incubated with 1:2000 horseradish peroxidase-conjugated anti-rabbit, -goat, or -mouse IgGs (Pierce, Rockford, IL) for 1 h at room temperature. The blots were washed again. The individual target proteins were developed with chemiluminescent reagent (Cat. no. DW101, EasyECL Western Blot kit; TransGen Biotech Co. Ltd., Beijing, China) using the enhanced chemiluminescence detection system. The relative band density was determined on an imaging system (Scion Image for Windows; Scion Corporation, Federick, MD). The results described were obtained in at least three independent experiments. Gel loadings were normalized with β-actin antibody. Immunocytochemistry Detection of CD14 and TLR4 6 ATII were plated onto 18 × 18 mm glass coverslips and treated with LPS for 3 h in the presence/absence of propofol as described in experimental design. Afterwards, the coverslips were fixed with 4 % paraformaldehyde for 30min at room temperature and washed 3 times in PBS. Cells were incubated with blocking solution (5% BSA) at room temperature for 15 min and incubated overnight at 4℃ with 1: 160 dilution of anti-CD14 antibody (sc-9150) and with 1: 160 dilution of anti- TLR4 antibody (sc-16240). Slides were then washed 3 times with PBS and incubated with 1:200 Rhodamine (TRITC)-Conjugated AffiniPure Goat Anti-Rabbit IgG (H+L) (Cat. no. ZF-0316, Beijing Zhongshan Golden Bridge Biotechnology Co., Ltd., China) and 1:200 Fluorescein (FITC)-conjugated AffiniPure Rabbit Anti-Goat IgG (H+L) (Cat. no. ZF-0313, Beijing Zhongshan Golden Bridge Biotechnology Co., Ltd., China). TNF-α nzyme-linked immunosorbent assay Cell culture supernatants were collected and stored at -70℃ until analysis. The levels of TNF-α were determined in duplicate using rat TNF-α kit (R&D Systems Inc, Minneapolis, MN) following the manufacturer’s instructions. The results are presented as the mean ±SD of three replicates from one representative experiment; this experiment was repeated three times. Statistical analysis The data were normally distributed as determined by the Levene’s test. ANOVA followed by a post hoc Tukey’s test was used for multiple-group comparisons. Values are expressed as means±SD. The significance level was set at P<0.05. SPSS 13.0 software (SPSS Inc. Chicago, IL) was used for all statistical work. Results Identification of ATII cells The cell mix, obtained by the discontinuous Percoll gradient centrifugation method, contained 82±5% of ATII which were stained blue with alkaline phosphatase histochemical staining. (Fig.1A). Transmission electron microscopy showed typical lamella bodies in ATII. (Fig. 1B) 7 Fig1. Alkaline phosphatase histochemical staining shows ATII in blue by phase-contrast objective (1A). 200×. ATII cells are characterized by lamellar body (LB) inclusions in the cytoplasm by transmission electron micrographs (1B), magnification: 4000×. CD14 and TLR4 mRNA changes with different concentration of propofol LPS at the concentration of 1μg/ml significantly increased the CD14 mRNA (P<0.05) and TLR4 mRNA (P<0.05) in ATII. To determine whether propofol suppressed the LPS induced CD14 and TLR4 mRNA expression in cultured ATII, various concentrations of propofol (25, 50, and 100μM) were used in this study. Propofol at the concentrations of 50 and 100μM (p<0.05) dose-dependently suppressed both CD14 and TLR4 mRNA expression of the LPS-treated AT II cells (Fig. 2). Fig. 2 Relative expression of CD14 and TLR4 mRNA. (A) CD14 mRNA expression increased significantly in the LPS group and P1 group compared with control. CD14 mRNA expression is suppressed significantly in the P2 group and P3 group compared with LPS group. (B) TLR4 mRNA expression increased significantly in the LPS group and P1 group compared with control. TLR4 mRNA expression is suppressed significantly in the P2 group and P3 group compared with LPS group. C = control; LPS = ATII cells subjected to 1μg/ml LPS; P1 = ATII cells subjected to 1μg/ml LPS and 25μM propofol; P2 = ATII cells subjected to 1μg/ml LPS and 50μM propofol; P3 = ATII cells subjected to 1μg/ml LPS and 100μM propofol. *compare with the control, P<0.05; # compare with LPS group, P<0.05 8 CD14 and TLR4 protein changes with different concentrations of propofol As quantified by scanning the chemiluminescence's bands from four different experiments. The CD 14 and TLR4 protein expression was increased after LPS stimulation for 3 hours (P<0.001 and P=0.002, respectively), and the increase was lower in the propofol and LPS cointubation compared with LPS alone. CD14 protein expressions were lower in P1, P2 and P3 groups compared with LPS group with P<0.001. TLR4 protein expressions were lower in P2 and P3 groups compared with LPS group with P=0.003 and P<0.001, respectively. Figure 3. Fig. 3. Representative immunoblot of CD14 and TLR4 protein in ATII cells (Fig 3A and 3B). LPS increased both CD14 and TLR4 protein expression while propofol at concentration of 25, 50 and 100μM could decrease CD14 protein expression (Fig 3C) and propofol at concentration of 50 and 100μM could decrease TLR4 protein expression (Fig 3D) compared with LPS alone. C = control; LPS = ATII cells subjected to 1μg/ml LPS; P1 = ATII cells subjected to 1μg/ml LPS and 25μM propofol; P2 = ATII cells subjected to 1μg/ml LPS and 50μM propofol; P3 = ATII cells subjected to 1μg/ml LPS and 100μM propofol. *compare with the control, P<0.05; # compare with LPS, P<0.05 9 Distribution of CD14 and TLR4 in ATII with immunofluorescence To confirm the TLR4 expression on the cell surface, we performed the phase contrast imaging that revealed the location of TLR4 expression on the external membrane of AT II cells. (Figure 4). We further investigated the effect of LPS and propofol on CD14 and TLR4 distribution using confocal microscope. As shown in Fig. 5, distribution of CD14 on the cell surface is consistent with TLR4 and we observed CD14 and TLR4 increase in ATII in response to LPS (1μg/ml) treatment. After stimulation with propofol at 25μM, 50μM and 100μM, CD14 and TLR4 expression in ATII decreased in a dose-dependent manner. Fig. 4. Phase-contrast micrograph shows the AT II cells (Fig 4A) and TLR4 expressions were shown by immunofluorescence micrographs (Fig 4B). The majority of cells in cultures were positively stained with an antibody to TLR4 protein on the external surface (Fig 4C). 10 11 Fig 5 Representative photomicrographs of ATII cells subjected to immunofluorescence analysis. Cells were fixed, permeabilized, and stained with antibodies to CD14 (shown in red) and TLR4 (shown in green). There were increases in CD14 and TLR4 expressions in LPS group. CD14 and TLR4 expressions were lower in P1, P2 and P3 groups compared with LPS group. C = control; LPS = ATII cells subjected to 1μg/ml LPS; P1 = ATII cells subjected to 1μg/ml LPS and 25μM propofol; P2 = ATII cells subjected to 1μg/ml LPS and 50μM propofol; P3 = ATII cells subjected to 1μg/ml LPS and 100μM propofol. Scale bars=37.5μm. Effect of propofol on TNF-α in LPS incubated ATII cells TNF-α levels in the control group was 271±35 pg/ml. 1μg/ml LPS increased TNF-α level to 600±222 pg/ml with P=0.003 compared with control. Propofol at concentration of 25μM, 50μM and 50μM decreased the TNF-α levels to 374±197 pg/ml, 325±79 pg/ml and 232±44 pg/ml in ATII cells with P values of 0.07, 0.017 and 0.001 compared with LPS group, respectively. (Figure 6) Fig 6. The concentrations of TNF-α were measured by ELISA. LPS incubation increased TNF-α concentration. Propofol at the concentration of 25, 50 and 100μM decreased the TNF-α concentration dose-dependently. C = control; LPS = ATII cells subjected to 1μg/ml LPS; P1 = ATII cells subjected to 1μg/ml LPS and 25μM propofol; P2 = ATII cells subjected to 1μg/ml LPS and 50μM propofol; P3 = ATII cells subjected to 1μg/ml LPS and 100μM propofol. *compare with the control, P<0.05; # compare with LPS, P<0.05. Results are representative of three independent experiments. Discussion In this study, we demonstrated propofol at the concentration of 50 μM and 100 μM decreased CD14 and TLR4 in primary cultured adult rat AT II cells at the mRNA and protein levels as well as decrease TNF-α secretion. The CD14 and TLR4 expression are key early event in the generation of an innate immune response mediated 12 LPS-signaling pathway and may play a key role in the regulation of alternative splicing of NF-κB in the lungs after injury9, 13. LPS upregulates the CD14 and TLR4-dependent cytokine production in various cell types through mechanisms involving p38 MAPK, ERK1/2, or JNK14, 15 An upregulated TLR-4 expression is known to play a pivotal role in the development of sepsis-related organ injuries16. In our study, stimulation of ATII with LPS for 3 hours triggered significant upregulation of CD14 and TLR4 gene expression, hence TNF-α expression, which is consistent with the previous reports. Pretreatment with 100μM propofol in hepatocytes was reported to alleviate sepsis-related systemic inflammatory response by downregulation of TLR4 expression and partial suppression on the phosphorylation of ERK1/2 and IκB-α as well as the NF-κB nuclear translocation 17. Propofol at a concentration of 157 μM reportedly increased LPS-stimulated TNF-α production in human whole blood 18, it was shown to inhibit nitric oxide and TNF-α release from alveolar macrophages in an endotoxin-induced lung injury model 19 and to suppress nitric oxide and iNOS expression in LPS-stimulated macrophages at 25–100 μM 20. However, there is no study about the immunorgulation of propofol on the primaried cultured ATII cells. To our knowledge, this is the first study to report the effects of propofol on inflammatory responses of primary cultures of rat alveolar type II cells stimulated with LPS. We found that propofol dose-dependently reduced LPS-stimulated increase of CD14 and TLR4 in ATII cells. Propofol was also found to inhibit LPS-induced TNF-α production in ATII cells. Significant effects on ATII cells were observed at a propofol concentration of 50μM and 100μM. This study raised the possibility that propofol might modulate some of the inflammatory processes in these pathological conditions, which is consistent with our previous in vivo study that propofol attenuates the LPS induced acute lung injury through TLR4 downregulation. Clinically relevant blood concentration of propofol is 3-11 μg/ml (approximately 17-62 μM) for maintenance of satisfactory anesthesia 21, 22. The blood concentration of bolus injection of propofol can reach 56 μM 23. Therefore we considered 25–100μM as the range of clinically relevant concentrations achievable during propofol anaesthesia. Our results suggest that propofol may modulate some of the inflammatory responses of ATII cells stimulated by LPS in vitro at the high range of clinically achievable concentrations. In conclusion, we found that propofol at the concentration of 50 and 100μM inhibited some of the inflammatory responses of alveolar type II cells treated with LPS with decreasing TNF-α levels. Propofol, in large concentrations 13 (more than 50μM), may be a good choice of anesthetics to reduce inflammatory responses when using in patients with acute lung injury and related respiratory diseases. Acknowledgements This work was supported financially by the Hospital Foundation of Shengjing Hospital of China Medical University, China. 14 References 1. Evans MJ, Cabral LJ, Stephens RJ, et al. Transformation of alveolar type 2 cells to type 1 cells following exposure to NO2. Exp Mol Pathol 1975; 22:142-50. 2. Crandall ED, Matthay MA. Alveolar epithelial transport. Basic science to clinical medicine. Am J Respir Crit Care Med 2001;163:1021-9. 3. McRitchie DI, Isowa N, Edelson JD, et al. Production of tumour necrosis factor alpha by primary cultured rat alveolar epithelial cells. Cytokine 2000; 12: 644–654. 4. Farivar AS, Woolley SM, Fraga CH, et al. Proinflammatory response of alveolar type II pneumocytes to in vitro hypoxia and reoxygenation. Am J Transplant 2004; 4:346-51. 5. Hahon N, Castranova V. Interferon production in rat type II pneumocytes and alveolar macrophages. Exp Lung Res. 1989;15:429-45. 6. da Silva Correia J, Soldau K, Christen U, et al. Lipopolysaccharide is in close proximity to each of the proteins in its membrane receptor complex. J Biol Chem 2001; 276: 21129-35. 7. Jiang Q, Akashi S, Miyake K, Petty HR. Lipopolysaccharide induces physical proximity between CD14 and toll-like receptor 4 (TLR4) prior to nuclear translocation of NF-kappa B. J Immunol 2000;165:3541-4. 8. Landmann R, Zimmerli W, Sansano S, et al. Increased circulating soluble CD14 is associated with high mortality in Gram-negative septic shock. J Infect Dis 1995; 171:639-44. 9. Togbe D, Schnyder-Candrian S, Schnyder B, et al.TLR4 gene dosage contributes to endotoxin-induced acute respiratory inflammation. J Leukoc Bio 2006; 80:451-7. 10. Wissel H, Schulz C, Koehne P, et al. Chlamydophila pneumoniae induces expression of toll-like receptor 4 and release of TNF-alpha and MIP-2 via an NF-kappaB pathway in rat type II pneumocytes. Respir Res 2005; 6: 51. 11. Armstrong L, Medford AR, Uppington KM, et al. Expression of functional toll-like receptor-2 and -4 on alveolar epithelial cells. Am J Respir Cell Mol Biol 2004; 31: 241-5. 12. Richards RJ, Davies N, Atkins J, Oreffo VI. Isolation, biochemical characterization, and culture of lung type II cells of the rat. Lung, 1987; 165: 143-158. 13. Phan HH, Cho K, Sainz-Lyon KS, Shin S, Greenhalgh DG. CD14-dependent modulation of NF-kappaB 15 alternative splicing in the lung after burn injury. Gene 2006; 371:121-9. 14. Cheng C, Qin Y, Shao X, et al. Induction of TNF-alpha by LPS in Schwann cell is regulated by MAPK activation signals. Cell Mol Neurobiol 2007; 27: 909–921. 15. O'Toole T, Peppelenbosch MP. Phosphatidyl inositol-3-phosphate kinase mediates CD14 dependent signaling. Mol Immunol 2007; 44: 2362–9. 16. Barsness KA, Arcaroli J, Harken AH, et al. Hemorrhage-induced acute lung injury is TLR-4 dependent. Am J Physiol Regul Integr Comp Physiol 2004; 287: R592–9. 17. Jawan B, Kao YH, Goto S, et al. Propofol pretreatment attenuates LPS-induced granulocyte-macrophage colony-stimulating factor production in cultured hepatocytes by suppressing MAPK/ERK activity and NF-kappaB translocation. Toxicol Appl Pharmacol 2008; 229:362-73. 18. Larsen B, Hoff G, Wilhelm W, Buchinger H, Wanner GA, Bauer M. Effect of intravenous anesthetics on spontaneous and endotoxin-stimulated cytokine response in cultured human whole blood. Anesthesiology 1998; 89:1218-27. 19. Chu CH, David Liu D, Hsu YH, Lee KC, Chen HI. Propofol exerts protective effects on the acute lung injury induced by endotoxin in rats. Pulm Pharmacol Ther 2007; 20:503-12. 20. Chen RM, Wu GJ, Tai YT, et al. Propofol reduces nitric oxide biosynthesis in lipopolysaccharide-activated macrophages by downregulating the expression of inducible nitric oxide synthase. Arch Toxicol 2003; 77:418-23. 21. Short TG, Aun CS, Tan P, et al. A prospective evaluation of pharmacokinetic model controlled infusion of propofol in paediatric patients. Br J Anaesth 1994; 72: 302– 6. 22. Gepts E, Camu F, Cockshott ID, Douglas EJ. Disposition of propofol administered as constant rate intravenous infusions in humans. Anesth Analg 1987; 66: 1256–63. 23. Servin F, Desmonts JM, Haberer JP, et al. Pharmacokinetics and protein binding of propofol in patients with cirrhosis. Anesthesiology 1988; 69:887–91.