Methods and Materials
advertisement

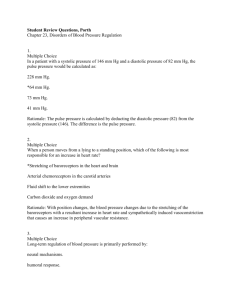
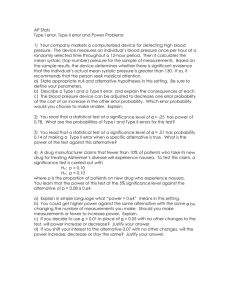
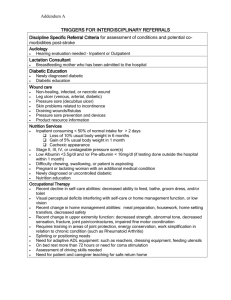
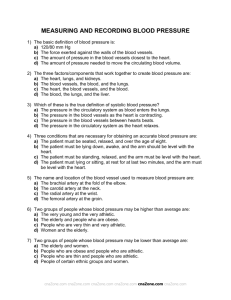
Effects of Magnesium Di-Potassium EDTA suppositories on the symptoms of Diabetes Mellitus Type One Spencer Feldman and Boris Ljahnicki M.D. PhD. April 2004 ABSTRACT: 29 adults both male and female with an average age of 50, diagnosed with Diabetes Mellitus Type 1 with complications of the feet were divided into three Groups. 11 were given 365 mg Magnesium Di-Potassium EDTA suppositories in a cocoa butter base for one month then placebos for an additional month, 12 were given Magnesium Di-Potassium EDTA suppositories for two months, and 6 were given placebos from the beginning. While significant improvements were seen in the first month in all measured parameters, for those that continued for 2 months, glucose decreased 54%, pulse pressure decreased 34% and the conditions of the diabetic foot improved as measured by a 37% decrease in total score using the (S)AD system. In those subjects with significant hypertension, systolic BP decreased 22% and diastolic BP decreased 12.6%. The study was open label and placebo controlled. Subjects were told to refrain from taking long acting insulin the night before any tests were to be performed. Methods and Materials 29 subjects diagnosed with Diabetes Mellitus Type 1 were tested before, during and after administration of 365 mg Magnesium Di-Potassium EDTA suppositories with blood chemistries and assessed via the (S)AD System by Rosamund M. McFarlane (The Diabetic Foot Journal, Vol. 2, No. 4, 123-131, 1999). The (S)AD Classification has three grades, scoring affected area, depth, sepsis, arteriography, and denervation. Also performed was the 6 stage Simple Staging System by Ali Foster (The Diabetic Foot Journal, Vol. 3, No. 2, 56-62, 2000). 6 subjects were also assessed pre and post with Doppler. The subjects were divided into three Groups. Group one consisted of 12 subjects who were instructed to take the suppositories as follows: one per day for 14 days, one every other day for approximately 53 days. Group, consisting of 11 subjects two were to take the suppositories as follows: one per day for 14 days, 1 every other day for approximately 21 days, then placebo suppositories for approximately 30 days. Group three, consisting of six subjects only received placebo suppositories throughout the entire study. Two of the 12 subjects from Group one did not complete the study, two of the 11 subjects in Group two did not complete the study and four of the six subjects in Group three (the placebo Group) did not complete the study. Those in Group two were given placebo suppositories during the 31 st through the 60 th days. Days are given as ~35 and ~67 in the charts since some subjects were tested a few days before or after the target dates. 35 and 67 represent the average number of days that passed between the initial baseline testing, and the two follow up tests/assessments. Actual testing days for both dates of subjects in both Groups one and two are days number (29,32,32,34,36,36,36,39,54) and (59,63,63,64,67,67,70,70,82) respectively. Data on the placebo-only subjects is not given, as the majority of them did not complete the study. This is understandable since they did not show any improvement, and without any improvement, who would want the inconvenience of going to a medical office, taking blood tests and taking suppositories. Data on the results of Group two following the first month, after which point they too were on placebos, is also not given. As expected, many of the gains experienced by Group two are lost when they began placebo. Discussion Glucose measurements at the onset of the study (Day 0) of Groups one, and Groups one and two combined showed average glucose readings of 348 and 361mg/DL respectively. After the first month the average glucose reading of Groups one and two combined decreased to 231 a 36% decrease. By the end of the second month, the average glucose reading of Group one subjects decreased again to 159 from their initial 348, a 189-point drop. This represents a 54% decrease in blood glucose for Group one. The background represents Group one and two (G 1+2), and the foreground represents only Group one (G1) The average pulse pressure (systolic minus diastolic) of Group one (G1) and Groups one and two combined (G 1+2) at the start of the study were 87 and 74 respectively. At the end of the first month, the average pulse pressure for G1 and G 1+2 respectively dropped to 62 and 61. This represents a 28% decrease for G1 and a 17.5% decrease for G 1+2. By the end of the second month, the average pulse pressure for G1 had dropped to 57, a 34% decrease from the beginning of the study. From a cardiological perspective, this represents (for males) a drop in the biological age of their hearts from 75+ to 55 years of age. 1 The drop in pulse pressure is especially significant in the light of the fact that a pulse pressure of 65 or more triples the risk of heart attack. 2 The background represents Group one (G1) and the foreground represents Groups one and two (G 1+2) The average systolic and diastolic blood pressures those subjects in Group one with significant hypertension (as defined as systolic readings greater than 150) was 198/101. By the end of the second month, the average systolic and diastolic blood pressures for this group dropped to 140/83, a 29% drop of the systolic and an 18% drop of the diastolic. Blood pressure control can reduce cardiovascular disease (heart disease and stroke) by approximately 33% to 50% and can reduce microvascular disease (eye, kidney, and nerve disease) by approximately 33%. In general, for every 10 millimeters of mercury (mm Hg) reduction in systolic blood pressure, the risk for any complication related to diabetes is reduced by 12% 3 , thus the 58 point drop in systolic pressure would represent a 70% decrease in any diabetic complications. The background represents systolic and the foreground represents diastolic The condition of the feet was measured both by the (S)AD classification system as shown in the table below, as well as in a few circumstances, by Doppler. “Score” (which will show up in the chart on the following page represents the summation of all these grade values across the symptom columns for any one date and can vary from 0 to 15. Area Depth Sepsis Arteriopathy Denervation 10 – 30 mm sq Pinprick Pedal pulses sensation/VPT Skin intact No infection palpable normal Skin and Diminution of both Reduced or ab subcutaneous Superficial: slough pulses or absence of pinprick sensa tissues or exudate one VPT raised Neuropathy Tendon, joint, Absence of both dominant: pal capsule periosteum Cellulitis pedal pulses pedal pulses >30 mm sq Bone and/or joint spaces Skin intact <10 mm sq Osteomyelitis Gangrene Charcot foot The background represents the initial day 0 values for Groups one. The foreground represents the values for day ~67 of Group one. Information on Groups one and two combined for the first ~35 days is not included as it makes the chart too complicated and adds no unexpected information. After ~67 days, remarkable improvements were seen in all categories. The global (S)AD score decreased 37% from 6.3 to 4. Among the 9 subjects who after the first ~37 days received only placebo, 1 continued to improve, 6 maintained their gains and only two regressed in their total score. Only six Doppler measurements could be made, but among them, amplitude increases in the non-computerized Doppler's that did not go off the top of the scale on the measurement paper after EDTA showed increases of 175%, 200% and 260%. 66% of the subjects in Group one had the ‘Area' score drop by a full point indicating that the affected area decreased from 10-30mm 2 to <10mm 2 . 77% of subjects in Group one had their ‘Denervation' scores decreased by at least one full point with 22% of Group one's subjects having the ‘Denervation' score decrease by two full points. Conclusion Magnesium Di-Potassium EDTA in suppository form: • Has significant effect in lowering high glucose readings. • Has significant effect in lowering high blood pressure and high pulse pressures. • Significantly decreases the biological age of the diabetic heart. • Decreases the area, depth, septic condition, arteriopathy and denervation of the diabetic foot. • Increases blood flow to the diabetic foot. • Represents a novel and important approach to the diabetic condition. 1 Biological Aging Measurement Clinical Applications, Ward Dean M.D. page 300, 1998. 2 Pulse Pressure: A predictor of Long-Term Cardiovascular Mortality in a French Male Population. Institut Natinal de la Sante et de la Recherce Medicale. Athanase Bentos MD, PhD. 3. Center for Disease control Diabetes website http://www.cdc.gov/diabetes/pubs/general.htm