Introductory Pharmacology
Abbreviations Fall 2002
Ann MacLeod, RN, BScN, MPH
Objectives
Identify components of a medication order
Interpret the meaning of a medication order
Identify the meanings of standard abbreviations used in medication
administration
Reading Medication Labels
*examine a variety of labels in your "Gray" text and describe what would be in
the container of these labels
*dose
*strength
*route
*total volume
*directions
Understanding an order
Colace 30 mg. PO QID
Name Dose Route Frequency
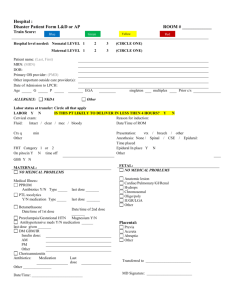
The Order
Pt. NAME: full name to avoid errors, pt.id #
DATE OF ORDER: may tell you when to stop drug
NAME OF DRUG: generic / trade name
DOSE: exact strength
ROUTE: how to give
TIME/ FREQUENCY : BID, od
SIGNATURE: MD, or midwife who wrote order
TYPES OF ORDERS
Stat- drug given immediately only that time, not again with that order
PRN- nurse gives when pt. needs a particular drug
Self terminating - time limited order (until temp ) some drugs can only be
given for a certain # of days (ie. 72hrs. or 7 days)
Medical directives
3 () checks for meds
check when taking out
patient
patient
when pouring
when putting away
6 Rights of Med Admin
drug
amount
time
route
documentation
Administration Process The 6 rights
drug
amount or dose
route
time
documentation
E.THE SIX RIGHTS
RIGHT PATIENT- always arm band or photo on MAR sheet, ask their name
RIGHT DRUG-check MAR sheet or kardex, do 3 checks
RIGHT DOSE (amount)- based on wt., tolerance, condition. never guess, you
may have to calculate
RIGHT ROUTE- can't change this, may be given a choice, if pt. can't tolerate
contact MD
6 RIGHTS Cont’d
RIGHT TIME - a part of the order see abbreviations for clarification
RIGHT DOCUMENTATION- chart where we should
PREPARING THE MEDS
Meds are prepared in med room or at the pt. bedside with the cart, meds
should be locked when not using , some kept in fridge
STEP 1- check MAR or med ticket with MD Rx or kardex
STEP 2- ensure order is complete & you understand it
STEP 3- prepare med (3 checks)
PREPARING THE MEDS cont’d
STEP 4- identify pt. & prepare to give (some pts. want more teaching info than
others)
STEP 5- record : name, route, admin time, dose, signature, status
always compare armband with MAR sheet or med card (don’t assume you
have the right pt.)
if no arm band check photo id, ask another nurse to verify or ask pt. to state
their name
STEP 6- assess for adverse effects, check within hr. & record if req’d
Identifying the pt.
Right Patient
Abbreviations : Doses
mL
Meq
L
cc
cm
kg
ii
tab
cap
kvo keep vein open
ss
tsp.(t)
u
mcg ( microgram)
mg ( milligram)
g ( gram )
tbsp. (T)
gr.
Gtt drop
mEq milliequivalents
Abbreviations: Routes PO - orally vs SL sublingual
Parenteral
IV - intravenous
SC - subcutaneous
IM - intramuscular
Instillation - drops gtt - NG (Nasogastric tube)
OD - right eye OS - left eye OU - both eyes
Insertion - supp or pr (per rectum) or vag (vaginal)
Topical - percutaneous ung or oint ( ointment) - transdermal patch
Inhalation
NPO nothing by mouth
Abbreviations - Time
Od
once per day
bid
twice per day
tid
three times per day
qid
4 times per day
q
every
qod
every other day
q1h
every 1 hour
q 4h
every 4 hours
Stat
now
prn
as needed
ac
before meals
pc
after meals
hs
at bedtime
DOCUMENTATION
the medication record is a legal document –nurse name & status signed for
each med given : drug, dosage, route,time, signature
the record keeps team informed
chart as soon as you give
prn's, stats may be charted in 2 places
response to med must be charted somewhere
Examples
Zidovudine 200 mg po q4h
Synthroid 200 mcg po qd
Regular Humulin insulin 5 U sc ac and hs
Mylanta 1 oz po q4h prn
Gentamycin 45 mg IVPB q 12h
Prednisone 10 mg po qod
 0
0