Text Only Version
advertisement

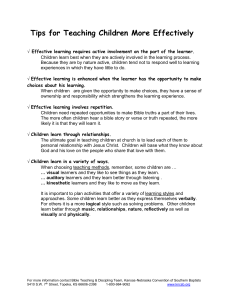
Slide 19- The most widely understood learning style is the Sensory Modality Preferences Theory. Research indicate that 35% of people are mainly visual learners, 25% mainly auditory and 40% are kinesthetic, in other words, prefer to manipulate or be involved in their learning environment as opposed to viewing or hearing. There are several free sensory modality preference tests available on the internet. Three are featured on this slide. You should chose one and take a test to determine your personal learning style preference. This is a highly interesting personal exploration that you are asked to do on your Training of Trainers journey. Take some time to do just that. What is your learning style? Share that information with one another and encourage fellow students to do likewise. Slide 20 – Visual learners learn through seeing. Their primary perceptual preference is visual. They can often recall what they have read or observed. They like to look at illustrations or diagrams or watch something, rather than listening only. They may be learners who make lists. Moreover, they tend to be more pro-active when their environments are neat. A cluttered environment would hinder their learning or cause anxiety. Slide 21- Auditory learners prefer to listen. They can memorize what they hear and tend to be very attentive when information is presented in this way. They search for meaning and interpretation in lectures or speeches and are tuned into tone of voice, pitch, speech and other auditory signals. They need to be told what to do rather than have them read directions. Slide 22- Kinesthetic or tactile learners need to write things down. This sometimes is confused with visual, or may partner with visual. They like to incorporate their fine motor skills. They like to take notes as they listen and keep their hands busy. Such learners like to use their bodies in the learning process. They need to DO, not just passively listen or watch in order to transfer information into understanding. Slide 23- The Multiple Intelligences Learning Style is more complex- taking the visual, auditory and tactile (physical) three sensory processes into more a diversified breakdown Slide 24 - The Multiple Intelligences learning theory breaks down learning styles into seven distinct preferences: visual/spatial; auditory/musical; linguistic; kinesthetic; mathematical; interpersonal and intrapersonal. Individuals can have combinations of these styles. Slide 25 - David Kolb describes “experiential learning theory” into four distinct stages- Concrete experiences; reflective observation; abstract conceptualization and active experimentation. He then elaborates his theory that postulates four types of learners, in other words, learning styles, based on experiential learning. Those are: Diverger/Experiencers- who prefer concrete experiences and reflective observation; Assimilators (Thinkers) – who prefer abstract conceptualization and reflective observation; Converger/Doers- who prefer abstract conceptualization and Active experimentation; and Accommodator/Integrators- who prefer concrete experiences and active experimentation. Slide 26 - Benner is noted for research on Novice to Expert theories of learning. Experts notice features and meaningful patterns of information that are not noticed by novices. They have acquired a great deal of content knowledge that is organized in ways that reflect a deep understanding of their subject matter. Their knowledge cannot be reduced to sets of isolated facts or propositions, but instead reflects contexts of applicability. That is, the knowledge is ‘conditionalized’ on a set of circumstances. They can flexibly retrieve important aspects of their knowledge with little attentional effort. Although they know their disciplines thoroughly, this does not guarantee that they can teach others. This is an important point and why we are here with this TOT course. The most important thing to look at is how many people in the field of clinical research vary in their “expertise” as clinical researchers. They may be very experienced in clinical medicine or nursing, but novices in clinical research. This is a case where someone travels from being an expert backwards to being a novice. It is important to remember what it is like to be a novice, new at something- and to summon flexibility and mentoring postures to help bring novices through experiences so that they can evolve as experts in their own right. Expert clinical researchers may be good at “teaching” a consent form, but not so good at teaching peers the processes of clinical research. This conflict also can occur when an expert clinician is then put into supervisory roles without training in management and business. Considerable research is being done on the theory of expert verses novice, in nursing and other healthcare settings. Slide 27- While the theories of learning and learning style preferences abound, there are ten basic characteristics of learning to consider. o First, we learn to do by doing. o Second, we learn to do what we do and not something else. o Third- without readiness, learning is inefficient and may be harmful. o Forth – without motivation, there can be no learning at all. o Fifth – for effective learning, responses must be immediately reinforced. o Sixth- Meaningful content is better learned and longer retained than less meaningful content. o Seventh – For the greatest amount of transfer learning, responses should be learned in the way they are going to be used. o Eighth- One’s response will vary according to how one perceives the situation; o Ninth – An individuals responses will vary according to the learning atmosphere; and o Finally, number ten- one does the only thing one can do given the physical inheritance, background and present acting forces. What do you think about those ten characteristics of learning? Do you agree with those? Can you think of how you have experienced each of these points- as a learner? As a clinician? As a trainer? As a manager? As a parent? Slide 28- A more simplified way to look at learning is to consider these four main components: 1. Motivation- the thing that moves the learner to action 2. Reinforcement- the positive and negative influences to the learning experience 3. Retention- things that influence retention of information or performance 4. Transference- which refers to the ability to use the learned information in a new setting Slide 29- Motivation – a term that comes from the Latin word- Movere- means to set in motion; a psychological force- something that moves someone to some kind of action. Readiness to learn is an important element of motivation and effects the transfer of new information to application. Theories in patient education often refer to motivation or readiness to learn as an important step in the learning process. This is described as the time when a learner demonstrates an interest in learning the type or degree of information necessary to maintain optimal health. It can also apply to staff members- - and the demonstrated interest in learning new skill-sets to maximize work performance or ethical behaviors in a clinical research setting. Slide 30- PEEK readiness to learn has been described as the physical, emotional, experiential and knowledge properties that influence learning. For instance, physical properties might be ability, task complexity, environmental effects, health status and gender. Emotional properties likewise would be anxiety, support systems, motivation and frame of mind. Examples of Experiential readiness factors could range from cultural background, past experiences with learning, locus of control and orientation. Finally, knowledge factors range from present knowledge base to general cognitive ability and effects of limitations of learning styles. Slide 31 - Most learners that are encountered at the clinical research site are adult learners. Those learners would be the staff members within the clinic, and adult clients, or parents and caregivers of pediatric clients. Adult learners have unique characteristics that influence how trainers and learners interact and exchange learning. Six primary characteristics of adult learners have been listed on this slide. Firstly, adults are at various stages of autonomy and they like to exercise autonomy in learning situations. Their concepts of self directly affect their behavior and desire to learn. They are their own persons- with vast life experiences and/or achievements. Adults also have a broad base of experiences to draw on and share with others. Sharing experiences is important and should be valued. They also seek to learn what they have identified as important rather than what others deem as important. In other words, adults must value the subject matter being taught. Slide 32 – Adults also want the learning to be immediately applicable to their work or life environment. They are problem-centered, rather than subject centered. Again this characteristic is related to the quest for applicable knowledge, rather than knowledge for knowledge-sake. They want to know (and be assured that) what they are learning is relevant to their needs, or at least to the needs of others. Slide 33 - Given those six characteristics, there are several principles of adult learning that should be discussed and applied to training endeavors at the clinical research site. These are practical tips for structuring the learning. Those principles are centered on how adults learn best. Practically speaking, adults learn best when: 1. Learning is related to an immediate need, problem or deficit. 2. Learning is voluntary and self-initiated 3. Learning is person-centered and problem centered 4. Learning is self-controlled and self-directed 5. The teacher role is that of a facilitator rather than “teacher” 6. Information and assignments are pertinent Slide 34- Adults also learn best when: 7. New material draws on past experiences 8. Threat to self is reduced to a minimum in the educational situation 9. They are able to participate actively in the learning process 10. Learning is done in a group 11. Nature of learning activity changes frequently 12. Reinforcement is given by application and prompt feedback. Given your most recent learning experiences, recall how those principles have been true for you as a learner, or how you have observed the learning environment to be maximized when those principles have been attended to. Slide 35 – This is a moment in which you should STOP and think. I would like for you to consider several points. 1. Given the characteristics and principles stated in the prior four slides- how would a teacher (or rather facilitator) modify teaching to maximize learning in adults? 2. Think of practical applications for adult learners in the clinical research site. 3. As a fellow adult learner, what “modifications” have you experienced that works best for you? This might be pulling together adult learner and learning style issues! Take your time to journal (Reflective Journal) about these three points. Also, note that there is a discussion assignment that relates to these points. Slide 36- Now it is time to begin to engage in the course and form a course community. Go to Assignment 1- found in the Discussion Section of VISTA. Download and complete the attached Word Document (illustrated below). Take a learning style inventory (select one from available options). Complete and attach to your discussion comments in the available sections. Please reply to at least one fellow student posting. This will help us formulate our course community. We want to know the following information about you: 1.Who are you? 2.Where do you work? 3.What kinds of research are your involved in? 4.What is your role at your research site? 5.What is YOUR main learning style? (You will find out by taking a learning style inventory) 6.What is one important characteristic of adult learners (your opinion) 7.What works best for you as an adult learner? Please post your response to these questions in Assignment 1 Discussion Board.