Use PA Form# 20720
advertisement

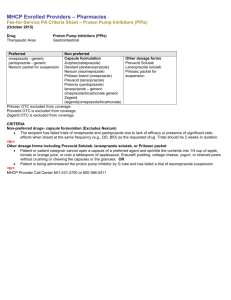
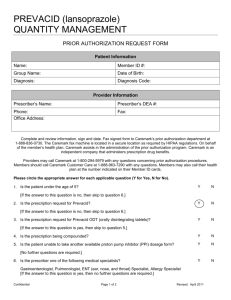
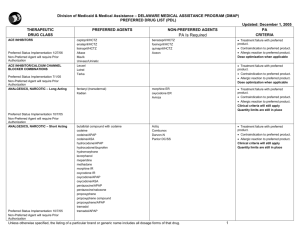
PPI.8 Form # 20720 R:7.11 State of Maine Department of Health & Human Services MaineCare/MEDEL Prior Authorization Form PROTON PUMP INHIBITORS www.mainecarepdl.org Phone: 1-888-445-0497 Member ID #: |__|__|__|__|__|__|__|__|__| Fax: 1-888-879-6938 Patient Name: ____________________________________ DOB: __________________ (NOT MEDICARE NUMBER) Patient Address:_________________________________________________________________________________________________ Provider DEA: |__|__|__|__|__|__|__|__|__| Provider NPI: __|__|__|__|__|__|__|__|__|__| Provider Name:_______________________________________________________________________ Phone:____________________ Provider Address:_____________________________________________________________________ Fax:____________________ Pharmacy Name:_____________________________Rx Address:________________________________Rx phone:_________________ Provider must fill all information above. It must be legible, correct and complete or form will be returned. (Pharmacy use only): NPI: __|__|__|__|__|__|__|__|__|__| NABP: |__|__|__|__|__|__|__| NDC: |__|__|__|__|__|__|__|__|__|__|__| Provider Prior authorization must fill all is not information required for the above. preferred It must proton bepump legible, inhibitors correct (PPI) and for complete a cumulativeor 60-days formofwill therapy be returned. per 12months. Prior authorization will be required for all non-preferred medications beginning the first day of therapy. Payment for a nonpreferred medication will be authorized only for cases in which there is documentation of previous trials and therapy failures with three preferred agents. Prior authorization is NOT required for Prevacid SoluTabs for children age 8 or younger for the first 60 days of therapy. Payment for Prevacid SoluTabs for patients 9 and older will be considered for those patients who cannot tolerate a solid oral dosage form. Preferred (PA required after 60 days) Omeprazole 20mg Pantoprazole Dexilant Non-Preferred (PA required from Day 1) Prilosec (OTC)6 Aciphex7 8 Prilosec (RX) Prevacid8 8 Omeprazole 10mg Prevacid SoluTabs8 Lansoprazole8 Nexium8 Omeprazole-Sodium Bicarbonate8 Protonix8 (8 or younger) Strength _________ Dosage Instructions ___________________ Quantity _________ Days Supply __________ Refills 1 2 3 4 5 Diagnosis: � Barrett’s esophagus � Erosive esophagitis � Hypersecretory conditions (Zollinger-Ellison syndrome, systemic mastocytosis, and multiple endocrine adenomas). � � Recurrent peptic ulcer disease after documentation of previous trials and therapy failure with at least one histamine H2-receptor antagonist at full therapeutic doses and with documentation of either failure of Helicobacter pylori treatment or a negative Helicobacter pylori test result. Symptomatic gastroesophageal reflux after documentation of previous trials and therapy failure with at least one histamine H2-receptor antagonist at full therapeutic doses. H2-receptor antagonist trial must have been in the last 12 months. Other:_____________________________________________________________________________________________ Trial Medication:_____________________________________ Trial Date From: ____________ To: ____________ Medical or contraindication reason to override trial requirements: _________________________________________________ Scope Performed? � No � Yes If yes, date of scope: ________________________________________________________ Reason for use of Non-Preferred drug requiring prior approval: ___________________________________________________ Patient is 9 years of age and cannot tolerate a solid oral dosage form? � No � Yes Attach lab results and other documentation as necessary. Pursuant to Chapter I, Section 80, The Department regards adequate clinical records as essential for the delivery of quality care, such comprehensive records are key documents for post payment review. Your authorization certifies that the above request is medically necessary, meets the MaineCare criteria for prior authorization, does not exceed the medical needs of the member and is supported in your medical records. Provider Signature: ________________________________ Date of Submission: ______________________ *MUST MATCH PROVIDER LISTED ABOVE