Document
advertisement

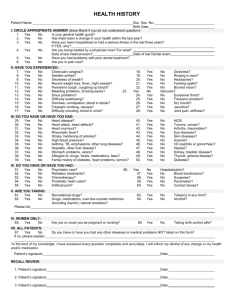
ISSRA AGE VERIFICATION & HEIGHT PREDICTION PROFORMA Annexure 1 To be filled (PRINT) in by the Subject/Parent/Sports federation and to be verified by the ISSRA Rep Computer Code: Date: PERSONAL DETAILS (To be filled in by the Subjects/Parents) TOURNAMENT DETAILS(in case of players) Name of Full Name Tournament Date of Birth Venue Age at last Dates birthday Country Age Group Home Address Phone No. E-mail SECTION 1 ( Chronological age) - To be filled in by the Subject/Parents/Sports Federation PLEASE ATTACH CERTIFIED COPIES OF THE FOLLOWING DOCUMENTS Document No. Date of Issue Date of Expiry Issuing Authority Birth Certificate Passport School Certificate (verifying age group) National Identity Card Place of Birth Name of the Hospital Father’s Name Father’s Date of Birth Photograph of subject (Paste here) Mother’s Name Mother’s Date of Birth Parents’ Date of Marriage Brothers/Sisters Date of Birth (in chronological order) Step brothers/sisters not to be included Age as on tournament cut off date I have been explained that the age verification protocol shall may involve Physical including external genitalia examination ,dental examination and radiographic examination and findings shall be accepted by me. Signature of the Player Date : SECTION 2 - PHYSIOLOGICAL AGE: To be filled in by ISSRA Doctor or Team Physician Physical Characteristics Height cms: Weight kgs: BMI Physical Appearance: Ecto/Meso/Endo Family history Height of the Father Cms: Height of the Mother Cms: Height of Brothers with age 1.Age height 2 Age height 1.Age height 2 Age height Height of Sisters with age Cms Any Medical problem in family SECTION 3- Dental Age : To be filled in by ISSRA Doctor or ISSRA Dental Surgeon Space behind 3rd molar (>15 years) Signature: 3.Age 3.Age height Cms height Signature: SECTION 4- Bone Age: To be filled in by ISSRA CONSULTANT Doctor Bone Age RUS Method TW3 Method Special Investigation (if any) MRI/CT Scan/X-rays Signature: REMARKS : We hereby accept the ISSRA Age verification Protocol and give our consent for the player to undergo the X-ray of the wrist and hand (AP view) and any other x-ray as advised The details of the above protocol has been explained to the SUBJECT AND PARENTS/GUARDIAN CONCLUSION Bone Age and Height predicted as determined by ISSRA Consultant Signature – Player/Guardian/Parent _________________________________________ Date _______________________________ Signature – Subject _________________________________________ Date _______________________________ Signature – Chairman, ISSRA Age Verification Board _________________________________________ Date _______________________________ Signature – Radiological Consultant --------------------------------------------------------Signature - Dental Surgeon _________________________________________ Signature Designated Team Physician by National federation----------------------------------- (NOT VALID FOR MEDICO LEGAL PURPOSE) Date _______________________________