Mechanical Ventilation Sedation Critical Care Orders
advertisement

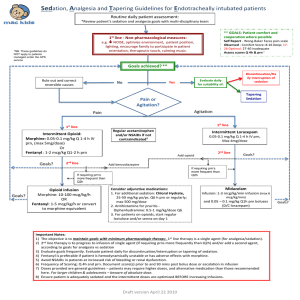
PLACE LABEL HERE MECHANICAL VENTILATION SEDATION CRITICAL CARE ORDERS The following orders will be implemented. Orders with a “” are choices and are NOT implemented unless checked. Initial all handwritten order modifications and the bottom of each page when indicated (multipage). 1. Assess and document Richmond Agitation Sedation Scale (RASS) q 2 hr. Maintain goal of: __________ Richmond Agitation Sedation Scale (RASS) Score Description Definition +4 Combative Overtly combative, violent, immediate danger to staff +3 Very Agitated Pulls or removes tube(s) or catheter(s); aggressive +2 Agitated Frequent non-purposeful movements, fights ventilator +1 Restless Anxious, but movements are not aggressive, vigorous 0 Alert and Calm Alert, able to follow simple commands -1 Drowsy Not fully alert, but has sustained awakening – eye opening/eye contact to voice (>10 seconds) -2 Light Sedation Briefly awakens with eye contact to voice (<10 seconds) -3 Moderate Sedation Movement to eye opening or voice (but no eye contact) -4 Deep Sedation No response to voice, but movement or eye opening to physical stimulation -5 Unarousable No response to voice or physical stimulation 2. Assess and document pain q 2 hrs 3. Spontaneous awakening trial (SAT) Sedation Vacation q 24 hrs between 0700 - 1200 Hold all sedative and narcotic infusions. The goal of the sedation vacation is to achieve a RASS of -1 to 0 Coordinate SAT with respiratory therapy and physician Check with the physician prior to performing SAT for patients with sedative infusions for active seizures, ethanol withdraw (CIWA Score ≥ 10), excessive agitation, or requires FIO2 ≥ 50% or PEEP > 8cm H2O to maintain SpO2 ≥ 88% If re-sedation indicated (RASS of +2 or greater) and vacation over 4 hrs, change to intermittent sedation as needed to maintain target score If sedation vacation < 4 hrs, resume continuous infusion at ½ of original rate after a bolus dose o Exclude patients with High frequency ocilation ventilator (HFOV), Neuromuscular Blocking Agents, Intracranial Pressure (ICP) monitoring or elevation, Uncontrolled arrhythmias, or Active myocardial ischemia within the last 24 hrs Order writer’s initials _______ Copy to pharmacy *3-15395* FORM 3-15395 REV. 12/2014 Page 1 of 2 MECHANICAL VENTILATION SEDATION CRITICAL CARE ORDERS PLACE LABEL HERE The following orders will be implemented. Orders with a “” are choices and are NOT implemented unless checked. Initial all handwritten order modifications and the bottom of each page when indicated (multipage). 4. Do not perform wake-up assessment Perform wake-up assessment using guidelines below: Diprivan (propofol): Perform wake-up assessment at scheduled times: 0400, 0800, 1200, 1600, 2000, 2400. Allow RASS score to elevate to ≥ -1. When performing a wake-up assessment on Diprivan (propofol), decrease rate 5–10 mcg/kg/min every 5 – 10 min until RASS equal to -1 or 0 All other Anxiolytics or Analgesics: Perform sedation vacation as stated above Neuro Patients: MEDICATIONS: 5. Consider a combination of an analgesic and an anxiolytic for synergistic effect. May use combination of intermittent and continuous if needed. INTERMITTENT IV SEDATION/ANALGESIA: If RASS is greater than ordered level and SBP > 90, give: Analgesic (check one): Fentanyl 25 - 100 mcg IV push q 2 hr prn Morphine 1 - 4 mg IV push q 2 hr prn Anxiolytic (check one): Versed (midazolam) 2 - 5 mg IV push q 1 hr prn Ativan (lorazepam) 0.5 - 2 mg IV push q 1 hr prn If able to maintain goal RASS with boluses more than 2 hrs apart, continue to administer intermittent sedation If patient requires boluses more frequently than q 2 hrs, notify physician to consider continuous sedation CONTINUOUS INFUSION MAINTENANCE: Analgesic (check one): Fentanyl: Continuous infusion: 0.05 - 5 mcg/kg/hr IV, initiate at lowest end of range after prn bolus Morphine: Anxiolytic (check one): Versed (midazolam): Ativan (lorazepam): Diprivan (propofol): If titration upward needed, increase by 25 mcg/hr PRN bolus: Fentanyl 25 mcg every 1 hr prn Continuous infusion: 1 - 10 mg/hr IV, initiate at lowest end of range after prn bolus If titration upward needed, increase by 1 mg/hr PRN bolus: Morphine 2 - 4 mg q 1 hr prn Continuous infusion: 0.5 - 10 mg/hr IV, initiate at lowest end of range after prn bolus If titration upward needed, increase by 1 mg/hr PRN bolus: Versed (midazolam) 0.5 - 2 mg IV push q 1 hr prn Continuous infusion: 0.5 - 10 mg/hr IV, initiate at lowest end of range after prn bolus If titration upward needed, increase by 1 mg/hr PRN bolus: Ativan (lorazepam) 0.5 - 2 mg IV push q 1 hr prn Continuous infusion: start at 5 mcg/kg/min May increase in increments of 5 - 10 mcg/kg/min q 10 min prn Lab: Triglyceride level every 3 days if on Diprivan (propofol) Precedex (dexmedetomidine) Continuous infusion: 0.2 - 1 mcg/kg/hr x 48 hours 6. Reversal agent for: Fentanyl or Morphine: Versed (midazolam) or Ativan (lorazepam): 7. 8. Narcan (naloxone) 0.4 mg IV in 10 ml NS, 0.5 ml q 1 min until change in alertness or max of 10 mg Romazicon (flumazenil) 0.5 mg IV q 5 min up to 3 mg total dose Isopto Tears (hypromellose) 2 drops in each eye q 6 hrs prn dry eyes, if not already ordered. Peridex (chlorhexidine) oral rinse 15 ml po BID, if not already ordered. Copy to pharmacy FORM 3-15395 REV. 12/2014 Page 2 of 2 MECHANICAL VENTILATION SEDATION CRITICAL CARE ORDERS _________________ ______________ Date Time PLACE LABEL HERE ____________________________________ Physician Signature _________________ PID Number Copy to pharmacy FORM 3-15395 REV. 12/2014 Page 2 of 2