finger joint stiffness - Orthopaedic Research Society
advertisement

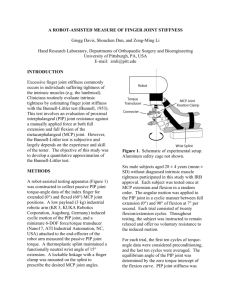
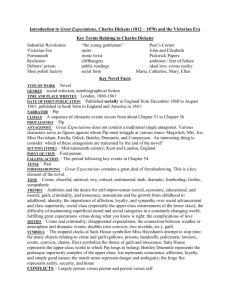
FINGER JOINT STIFFNESS Zong-Ming Li, Gregg Davis, Shouchen Dun Hand Research Laboratory, Department of Orthopaedic Surgery University of Pittsburgh, PA, USA. zmli@pitt.edu INTRODUCTION Finger joint stiffness, a manifestation of many joint diseases, severely compromises hand function. One of the causes of finger joint stiffness is the tightness of the intrinsic muscles. Clinicians routinely evaluate finger joint stiffness to determine intrinsic tightness by performing the Bunnell-Littler test [1]. This test involves an evaluation of proximal interphalangeal (PIP) joint resistance against a manually applied force at both full extension and full flexion of the metacarphalangeal (MCP) joint. However, the Bunnell-Littler test is subjective and largely depends on the experience and skill of the tester. The objective of this study was to quantitatively study finger joint stiffness with the MCP joint at different position. METHODS A testing apparatus (Figure 1) was constructed to collect passive PIP joint torque-angle data of the index finger with the MCP joint at extended (0°) or flexed (60°) positions. A low payload (3 kg) industrial robotic arm (KR 3, KUKA Robotics Corporation, Augsburg, Germany) was used to induce cyclic motion about the PIP joint and a miniature 6DOF force/torque transducer (Nano17, ATI Industrial Automation, NC, USA) was attached to the end-effecter of the robot arm to measure the passive PIP joint torque. A thermoplastic splint maintained a functionally neutral wrist angle of 15° extension. A lockable linkage with a finger clamp was mounted on the splint to prescribe the desired MCP joint angle (0° or 60°). Ten young male subjects without diagnosed intrinsic muscle tightness participated in this study. Each subject was tested at MCP extension and flexion in a random order. The angular motion was applied to the PIP joint in a cyclic manner between full extension (0°) and 90° of flexion at 7° per second. Each trial consisted of twenty flexion/extension cycles. Throughout testing, the subject was instructed to remain relaxed and offer no voluntary resistance to the induced motion. For each trial, the first ten cycles of torque-angle data were considered as preconditioning, and the last ten cycles were averaged. The equilibrium angle of the PIP joint was determined by the zero torque intercept of the flexion curve. PIP joint stiffness was calculated as the slope of the induced flexion curve in a 20° window starting from the equilibrium angle. Paired t-tests were performed for the statistical analyses with a significance level of α = 0.05. decrease in equilibrium angle, (b) an decrease in flexion torque at a given PIP joint position, and (c) an increase in extension torque at a given PIP joint position. For the induced flexion, the average equilibrium angle changed significantly from 47.6° ± 15.0° with the MCP joint extended at 0° to 21.9° ± 11.4° with the MCP joint flexed at 60° (p < 0.001). This may be due to passive tightening of the PIP joint extensors as the MCP joint assumes a flexed position. The PIP joint showed a significant increase in stiffness from 0.44 ± 0.24 N-mm/degree with the MCP joint flexed at 60° to 0.69 ± 0.22 N-mm/degree with the MCP joint extended at 0° (p < 0.01). This increase is most likely due to a passive tightening of the intrinsic muscles as the MCP assumes an extended position, because passive tightening of the intrinsic muscles provides an additional PIP extension torque due to their attachment to the extensor hood via the lateral bands. Joint stiffness is commonly evaluated based on a subjective feeling of joint resistance against applied force, or the observation of a limitation of range of motion. We have successfully developed a quantitative measure of PIP joint stiffness. PIP joint stiffness is dependant on the MCP joint angle, supporting the regulation role of the intrinsic muscles on PIP joint stiffness, and the use of Bunnell-Littler test for the evaluation of intrinsic muscle tightness. In future studies, we will compare PIP joint stiffness between asymptomatic hands and hands with intrinsic muscle tightness. We expect to find a much higher elevation in PIP joint stiffness when the MCP joint changes from flexion to extension for hands with intrinsic tightness. Other applications include the examination of the effectiveness of surgical procedures of intrinsic muscle release to reduce finger joint stiffness. Figure 2: Representative ten cycles of torque-angle data of the PIP joint at 60° MCP joint position. Figure 1. Schematic of experimental setup to measure passive stiffness of the PIP joint. RESULTS AND DISCUSSION A reproducible torque-angle relationship was demonstrated across multiple cycles (Figure 2). The induced flexion and extension torqueangle curves showed distinct hysteresis. As the MCP joint changed from an extended position to a flexion position (see Figure 3), the torque-angle curves shifted to the left (Figure 3), leading to (a) an Figure 3. Representative PIP joint torque-angle data of the induced flexion portion with MCP joint at 0° and 60º. REFERENCES [1] Bunnell, 1953. J Bone Joint Surg Am 35: 88-101 ACKNOWLEDGEMENTS The Pittsburgh Foundation 51st Annual Meeting of the Orthopaedic Research Society Paper No: 0120