Post-operative guidelines for patients
having total hip replacement
patient information BOOKLET
The Galway Clinic Department of Physiotherapy
Reproduced from the Arthritis Research Campaign information booklet www.arc.org.uk
Make your next appointment online @ www.galwayclinic.com
table of contents
1. Structure of Hip 1
2. Information on Total Hip Replacement (THR) 3. Physiotherapy 4. Exercise Programme for THR 5. Protocol Post Operatively 6. Cardinal Rules for THR 14 - 18
7. Activities on Discharge 17 - 20
8. Stairs Technique 21
9. Summary 22
2-4
5
6-7
8 - 13
10. Glossary 23
11. Notes 25
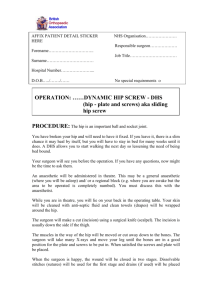
the healthy hip
The hip joint is one of the body’s largest weight bearing joints. It is a ball
and socket joint. The hip joint is formed where the head of the thigh bone
(femur) joins the pelvis.
Adapted from KRAMES communications
Cartilage is a layer of smooth soft tissue. It covers the head of the femur
and lines the socket that the thigh bone fits into. Healthy cartilage absorbs
stress and allows the ball to glide easily in the socket.
1
total hip replacement
This is a new artificial hip joint. There are two major types of artificial hip
joint: cemented and uncemented prosthesis.
Both types are widely used. The type of prosthesis used for your surgery
is usually decided upon by your surgeon based on your age, your lifestyle
and the surgeon’s preference. The head of the thigh bone is removed and a
new ceramic or metal head is fitted and fixed into the bone with or without
cement. A cemented prosthesis is held in place by a type of epoxy or bone
cement that attaches the metal to the bone. An uncemented prosthesis has
a fine mesh of holes on the surface area that touches the bone. The mesh
allows the bone to grow into the mesh and “become part of” the bone. The
socket in the pelvis itself is then fitted with an artificial plastic cover to form
a new joint.
Adapted from KRAMES communications
2
What Can I Expect From Hip Surgery?
Pain should no longer be a problem - that is the major benefit of surgery.
You will usually notice the benefit almost immediately after the operation,
although you will of course have pain from the surgery to start with. You
should also be less disabled and have greater mobility and a better quality
of life. It is important to remember that an artificial hip is not as good as a
natural hip. It does have some limitations, which are summarised later in
this booklet (see ‘physiotherapy’ and ‘After the first few weeks’).
What happens the day of the operATIon?
You will probably be given a tablet or an injection to sedate you
(a ‘pre-med’). In the operating theatre you will begiven an anaesthetic by
the anaesthetist. This may be a spinal or epidural injection (which makes
you lose feeling from the waist down). In certain circumstances or when
recommended by the anaesthetist, this may be a general anaesthetic (in
which case you will be asleep). Many patients nowadays have the spinal or
epidural, and are sedated if necessary during the course of the operation.
Once inside the operating theatre you will be placed either on your back
or on your side, depending on the way the surgeon does the operation.
3
What happens after leaving theoperating theatre?
When you leave the operating theatre you will usually have an intravenous
drip in your arm (to give you any fluid and drugs you may need) and one
to two suction drains in your hip (to remove fluid as the body heals).
You will be taken to a recovery room and kept there until you are fully
awake and the doctors feel that your general condition is stable.
Then you will be taken back to the ward with a wedged pillow strapped
between your legs to keep them apart.
You will be given painkillers to help relieve pain.
4
Physiotherapy
The physiotherapist will help to get you moving freely and advise you on
exercises to strengthen your muscles.
Don’t forget to pack the appropriate clothing to wear for your exercise
therapy. e.g. comfortable loose clothes and non-slip footwear
(e.g. trainers, rubber heeled shoes). Slip-on Shoes with no heel support
are NOT APPROPRIATE for gait re-training!!
Physiotherapy sessions will take place in the Galway Clinic Physiotherapy
Department daily at 11am - 12pm or 3pm - 4pm
Your physiotherapist will tell you when you are ready for these and which
session you are to attend.
5
Range of moTion exercises
Active hip and knee flexion:
• Lying on your back with legs straight, toes pointed toward the ceiling
arms by your side.
• Keep the heel in contact with the bed
• Bend your hip and knee
• Return to starting position
• Progress to 20 repetitions, 3 times a day
Active Abduction:
• Place a smooth surface (card table, plywood sheet, etc.)
under your legs.
• Begin with your legs together
• Spread legs apart as far as you can
• Hold legs apart for 5 seconds
• Return to the starting position
• Progress to 20 repetitions, 3 times a day
6
Strengthening Exercises
Quadriceps Setting:
• Tighten the muscles on the front of your thigh
• Push the back of your knee downward into the bed
• The result should be straightening of your leg
• Hold for 5 seconds, relax 5 seconds
• Progress to 20 repetitions, 3 times a day
Gluteal Setting:
• Lie on your back with your legs straight and in contact with the bed
• Tighten buttocks in a pinching manner
• Hold the isometric contraction for 5 seconds, relax 5 seconds
• Progress to 20 repetitions, 3 times a day
7
Day of OperaTIon
•
•
•
•
•
Adhere to Do’s and Don’ts (See Cardinal Rules)
Leave operating theatre with a triangular pillow between legs to
prevent crossing them
One to two drains from operation site are in place to clear excess fluid
Pain control
If awake do ankle exercises for five minutes hourly
• Deep breathing exercises hourly
Adapted from KRAMES communications
8
Day 1
•
•
•
•
Drain stays in place 24-48 hours
Up and mobilise with a walking frame under supervision of a
physiotherapist and assistant
May sit out.
Commence gentle hip and knee exercises to build up buttock and
thigh muscles (see exercises, strengthening and range of motion)
9
day 2
•
•
•
•
Drain out
Get out of bed with the assistance of one person
Increase distance covered with walking frame to a quarter of the
corridor
Attend Physiotherapy Classes to carry out exercise programme
(Please dress appropriately!)
10
Day 3
•
•
•
•
Get out of bed independently
Progress to using elbow crutches under the supervision of the
Physiotherapist
Increase the distance covered daily to half the corridor
Continue exercise programme in physiotherapy department
11
day 4
• Independent use of crutches
• Can walk the length of the corridor independently
• Continue to attend Physiotherapy classes
• Stairs with the Physiotherapist (see stairs technique)
Adapted from KRAMES communications
12
Day 5
• Independent on the stairs
• May shower once dressing has been changed
• Prepare for home
FOR THE NEXT SIX WEEKS:
•
•
•
•
Adhere to Do’s and Don’ts until your surgeon states otherwise
Walk as much as possible with crutches during this period
Continue with your exercises
Wear elastic stockings (TEDS) during this time
To sit safely, always
keep your back upright
and your knees level
with or below your hips.
Adapted from KRAMES communications
13
cardinal rules
• For the first six weeks post surgery or until your surgeon says otherwise
you must obey these three guidelines:
Rule 1
Do not let your hip bend more than 90° i.e. a right angle.
Therefore Do Not:
• Bend to pick anything up off the floor
• Sit on low chairs/toilets
Do:
• Take care when sitting and standing
DON’T bend all the way
over from the waist.
Instead, use a device
such as a long-handled
grasper, to reach down.
Adapted from KRAMES communications
14
cardinal rules
Rule 2
Do not allow your legs to cross the mid line of your body.
• Do sleep only on your back
• Do not cross you legs
DON’t let your knee
cross the midline of
your body.
INSTEAD sit with both
feet on the floor, with your
kneew 6 inches apart.
Adapted from KRAMES communications
15
cardinal rules
Rule 3
Do not twist your legs to the extremes of rotation.
• Do not swivel while walking
• Do take care when letting your leg roll outwards/inwards while in
bed/sitting
DON’T plant your foot
and rotate your new
hip inward.
INSTEAD, turn both your
feet and your body.
Adapted from KRAMES communications
16
When can I leave hospital?
Most people are able to climb stairs and are ready to leave hospital on
day 5. When you leave the hospital you will be given an appointment to
visit your surgeon in his rooms, as an out-patient. This is usually around
6 weeks after the operation and is a routine check-up which will make
sure you are progressing satisfactorily. You may also be offered outpatient
physiotherapy if this will help to improve your recovery.
Once you are home your GP will take out any stitches (sutures) somewhere
between 9-14 days. On discharge you will be given a pack for the GP and
advised when to make your appointment. If you have any problems with
your wound healing then you should tell the professional staff at the
hospital straight away.
It is important to adhere to your prescription as advised by your doctor.
You will be sent home on prescribed medications to control pain. Plan to
take your pain medication 30 minutes before exercises.
If pain control continues to be a problem, call your doctor.
17
What happens in the first few weeks AFTer the operaTIon?
Most people are relieved that the pain from the arthritis has gone. You may
find that you cannot bend your leg upwards as far as you would like - it is
important not to test your new joint to see how far it will go. You need to take
great care during the first 8-12 weeks after the operation, to avoid dislocating
the hip.
AFTer the first few weeks
You can expect to drive again after 6 weeks, and you could return to work at
about this stage, but only if you have a job which does not mean too much
moving around. Getting in and out of a car can be difficult - you may need to
sit sideways on the seat first and then swing your legs around.
You must take regular exercise. After all, that is one of the reasons for having
the operation. Walking, swimming and riding a bicycle are fine (but avoid
breaststroke when swimming). You can also play golf or bowls or walk the
dog. You should avoid running on hard surfaces and activities such as playing
squash or competitive tennis, as all of these involve sudden impact which
can overload your new hip (‘impact loading’). You should use your new hip
- exercise is good for your mind and your body. If you are not sure about a
specific activity, ask your surgeon, rheumatologist or physiotherapist. You
should continue to avoid any extreme position of the hip indefinitely. Normal
sexual activity can be started again at 6-8 weeks, although the warning about
avoiding extreme positions of the hip applies.
18
What are the long-term effects of hip replacement?
Your new hip should allow you virtually normal pain-free activity for a
great many years. There are many different types of replacement joint
nowadays.
While some do better than others, many other factors affect the outcome.
Over 80% of cemented hips should last for 20 years or more. The so-called
‘hybrid’ hips, in which only one part is cemented, have given good results
in active middle- aged patients.
19
Can there be any complicaTIons?
Hip replacement is major surgery. Risks vary according to your general
health and you should discuss the risks and benefits with your surgeon.
After hip replacement some people suffer from clots which form in the
deep veins of the leg. There are various ways to reduce this, including
special stockings, pumps to exercise the feet, and different drugs.
Contact your doctor or physiotherapist if you experience:
1. Any oozing or redness of the wound, fever or chills.
2. Any difficulty in breathing or heaviness in the chest.
20
Stairs Technique
Going Up-Stairs
• Maintain crutches/walking stick on the step below
• Lead with the un-operated leg up onto the step above
• Take your weight onto the un-operated leg by pushing on crutches
walking stick and banister
• Follow with the crutch/walking stick onto the same step
Going Downstairs
• Put crutch/walking stick down onto the step below
• Follow with the operated leg
• Take weight onto the operated leg using the crutches and banister
for support
• Follow with the un-operated leg onto the same step
21
summary
Cardinal Rules
• Do not let your hips bend more than 90 °/ a right angle
• Do not allow your legs to cross the midline of your body
• Do not twist your legs to the extremes of rotation
Exercises
• Active hip and knee flexion
• Active abduction
• Quadriceps setting
• Gluteal setting
• Straight leg raising (after six week post op)
Straight Leg Raising: (Not to be attempted until 5-6 weeks post
operation)
• Bend uninvolved leg by raising the knee and keeping the foot flat
on the bed
• Keeping your involved leg straight
• Lift involved leg about 6 to 10 inches from the bed
• Lower the leg slowly to the bed
• Progress to 20 repetitions, 3 times a day.
22
glossary
Acetabulum - the socket of the hip bone (pelvis), into which the head of
the femur fits.
Anaesthetic - a drug which removes sensation.
Ceramic-on-ceramic - a replacement hip joint in which both parts, or
both surfaces, are ceramic.
Ceramic-on-plastic - a replacement hip joint in which one part or surface
is ceramic (usually the ball or head) and one part or surface is plastic
(usually the socket).
Dislocate - to come out of position. In a hip joint this means that the ball
part of the joint comes out of the socket
Epidural - this term is often used to describe an injection given around
the area of the spinal nerves to anaesthetise the lower half of the body.
The full name is epidural blockade.
Femur - the thigh bone.
Prosthesis (plural ‘prostheses’ ) - an artificial body part.
An artificial hip joint is one example.
23
adapted from:
•
The American Academy of Orthopaedic Surgeons, July 2007.
• Data bases courtesy of the Irish Society of Chartered Physiotherapists
(ISCP) and the UK Chartered Society of Physiotherapy (CSP).
• Arthritis Research Campaign - www.arthritisireland.ie
(For further information contact www.arc.org.uk)
24
NOTES
25
The Galway Clinic, Orthopaedic & Sports Physiotherapy
Doughiska Co. Galway, Ireland
Phone: +353 (0)91 785 450/457
Fax: +353 (0)91 785 453
E-mail: physio@galwayclinic.com
Make your next appointment online @
www.galwayclinic.com
 0
0