Health, Wellness and Lifestyle Questionnaire
advertisement

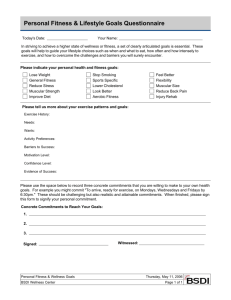
Health, Wellness and Lifestyle Questionnaire Name:______________________________ Phone#_____________________________ 8. __________________________________________ 9. Date of Birth: ____________ What types of things make you feel stressed? How do you deal with your stress? Sex: M / F __________________________________________ Person to contact in case of emergency: Name: ___________________________ Phone#___________________________ The following information is required and together with the Functional Movement Screen will assess your physical fitness level to establish an customized exercise program. Your health questionnaire and test results are confidential and will not be released to anyone other than yourself. 1. In the past year, how often have you been engaged in physical activity? ___ (4- 5 times/ week) ___ (2- 3 times/ week) ___ (1- 2 times/ week) ___ (None) 2. What type of physical activity do you consider fun? _______________________________________ 3. What are your personal barriers to exercise? __________________________________________ 4. What physical activity have you been successful with in the past? __________________________________________ 5. What is your present occupation? __________________________________________ 6. 7. Does your occupation require much activity ( i.e. walking, carrying things etc.) Yes___ No___ What are your leisure activities? __________________________________________ 10. How many meals and/or snacks do you have per day? __________________________________________ 11. Do you feel that you eat healthy most of the time? Yes___ No___ 12. Specifically describe what you would like to accomplish through your fitness program during the next: 1 month __________________________________ 4 months __________________________________ 1 year __________________________________ 13. Do you have any negative feelings toward, or have you had any bad experiences with physical activity programs? Yes___ No___ If yes, explain. ___________________________________________ 14. Do you start an exercise program but then find yourself unable to stick with them? Yes___ No___ 15. How much are you willing to devote to an exercise program? ______min/day ______ days/week 16. Are you currently involved in regular exercise? Yes___ No___ Health, Wellness and Lifestyle Questionnaire 17. Can you exercise during the work day? Yes___ No___ 18. Would an exercise program interfere with your job? Yes___ No___ 19. Would it benefit your job? Yes___ No___ 20. What type of exercises interest you? ___ Walking ___ Jogging ___ Swimming ___ Cycling ___ Strength training ___ Rowing ___ Tennis ___ Golf ___ Stretching ___ Other 21. What do you want exercise to do for you? ____________________________________ 22. Use the following scale to rate each goal separately: Very Important 1 2 3 4 5 6 7 a. Improve cardiovascular fitness b. Body-fat weight loss c. Reshape/tone my body d. Sport specific e. Ability to cope with stress f. Improve flexibility g. Increase strength h. Increase energy level i. Feel better j. Improve posture k. Enjoyment l. Other Not important 8 9 10 ___ ___ ___ ___ ___ ___ ___ ___ ___ ___ ___ ___ 23. How much would you like to change your current weight? (+) _____ lbs. (-) _____ lbs. 24. Anything else you would like your trainer to know? ______________________________________