EUROPEAN UROLOGY 65 (2014) 1058–1066
available at www.sciencedirect.com
journal homepage: www.europeanurology.com
Platinum Priority – Prostate Cancer
Editorial by Brian F. Chapin, Sean E. McGuire and Ana Aparicio on pp. 1067–1068 of this issue
Might Men Diagnosed with Metastatic Prostate Cancer
Benefit from Definitive Treatment of the Primary Tumor?
A SEER-Based Study
Stephen H. Culp a,*, Paul F. Schellhammer b, Michael B. Williams b
a
Department of Urology, University of Virginia, Charlottesville, VA, USA; b Department of Urology, Eastern Virginia Medical School, Norfolk, VA, USA
Article info
Abstract
Article history:
Accepted November 8, 2013
Published online ahead of
print on November 20, 2013
Background: Few data exist regarding the impact on survival of definitive treatment of
the prostate in men diagnosed with metastatic prostate cancer (mPCa).
Objective: To evaluate the survival of men diagnosed with mPCa based on definitive
treatment of the prostate.
Design, setting, and participants: Men with documented stage IV (M1a–c) PCa
at diagnosis identified using Surveillance Epidemiology and End Results (SEER)
(2004–2010) and divided based on definitive treatment of the prostate (radical prostatectomy [RP] or brachytherapy [BT]) or no surgery or radiation therapy (NSR).
Outcome measurements and statistical analysis: Kaplan-Meier methods were used to
calculate overall survival (OS). Multivariable competing risks regression analysis was
used to calculate disease-specific survival (DSS) probability and identify factors associated with cause-specific mortality (CSM).
Results and limitations: A total of 8185 patients were identified: NSR (n = 7811), RP
(n = 245), and BT (n = 129). The 5-yr OS and predicted DSS were each significantly higher
in patients undergoing RP (67.4% and 75.8%, respectively) or BT (52.6 and 61.3%,
respectively) compared with NSR patients (22.5% and 48.7%, respectively)
( p < 0.001). Undergoing RP or BT was each independently associated with decreased
CSM ( p < 0.01). Similar results were noted regardless of the American Joint Committee
on Cancer (AJCC) M stage. Factors associated with increased CSM in patients undergoing
local therapy included AJCC T4 stage, high-grade disease, prostate-specific antigen
20 ng/ml, age 70 yr, and pelvic lymphadenopathy ( p < 0.05). The major limitation
of this study was the lack of variables from SEER known to influence survival of patients
with mPCa, including treatment with systemic therapy.
Conclusions: Definitive treatment of the prostate in men diagnosed with mPCa suggests
a survival benefit in this large population-based study. These results should serve as a
foundation for future prospective trials.
Patient summary: We used a large population-based cancer database to examine
survival in men diagnosed with metastatic prostate cancer (mPCa) undergoing definitive
therapy for the prostate. Local therapy (LT) appeared to confer a survival benefit.
Therefore, we conclude that prospective trials are needed to further evaluate the role
of LT in mPCa.
# 2013 European Association of Urology. Published by Elsevier B.V. All rights reserved.
Keywords:
Metastatic prostate cancer
Radical prostatectomy
Brachytherapy
Outcomes assessment
* Corresponding author. Box 800422, Charlottesville, VA 22908, USA. Tel. +1 434 243 9325;
Fax: +1 434 982 3652.
E-mail address: shc5e@virginia.edu (S.H. Culp).
0302-2838/$ – see back matter # 2013 European Association of Urology. Published by Elsevier B.V. All rights reserved.
http://dx.doi.org/10.1016/j.eururo.2013.11.012
1059
EUROPEAN UROLOGY 65 (2014) 1058–1066
1.
prostate—either surgical removal or radiotherapy—on
survival in men diagnosed with mPCa using a large
population-based cancer database.
Introduction
Surgery or radiation therapy are standard treatment
options for men diagnosed with organ-confined prostate
cancer (PCa) and a life expectancy 10 yr [1]. For locally
advanced disease, radiation therapy with androgendeprivation therapy (ADT) is more commonly used.
However, for patients with metastatic disease at the
time of diagnosis, ADT remains the initial management
choice [2]. Despite data demonstrating improved survival
with tumor burden reduction in other malignancies [3–5],
including treatment of the primary tumor itself [6–9],
little data exist for men diagnosed with metastatic PCa
(mPCa). The purpose of this study, therefore, was to
examine the impact of definitive local therapy (LT) of the
2.
Methods
Cases were identified from the Surveillance Epidemiology and End
Results (SEER) database. SEER encompasses population-based cancer
registries covering approximately 28% of the US population and records
basic demographics, tumor site, histology, stage, grade, and treatments
performed. Because the mortality status of most all cases is known,
survival time can be accurately determined [10].
Cases were identified as any man 35 yr diagnosed with malignant
adenocarcinoma (International Classification of Diseases for Oncology,
third edition, code 8140) of the prostate (site code 61.9) between 2004
Table 1 – Patient characteristics
Characteristic
Median age, yr (IQR)^
Race, no. (%)
White
African American
Other
Year of diagnosis, no. (%)
2004
2005
2006
2007
2008
2009
2010
Marital status, no. (%)^
Single/widowed/divorced
Married
Unknown
PSA, ng/ml, no. (%)^
<10
10–19
20–29
30
Unknown
Tumor grade^
Low to moderate
High
Unknown
AJCC T stage, no. (%)^
T1/T2
T3/T4
Unknown
AJCC N stage, no. (%)^
N0
N1
Unknown
AJCC M stage, no. (%)^
M1a
M1b
M1c
EBRT received, no. (%)
No surgery or radiation therapy
(n = 7811)
72 (63–80)
5670 (72.6)
1570 (20.1)
571 (7.3)
Radical prostatectomy
(n = 245)
62 (58–67)
p valuea
Brachytherapy
(n = 129)
p valueb
p valuec
<0.001
0.514
68 (61–74)
<0.001
0.633
<0.001
0.756
0.004
0.007
0.086
<0.001
<0.001
<0.001
<0.001
<0.001
0.002
<0.001
<0.001
<0.001
0.002
<0.001
<0.001
<0.001
186 (75.9)
43 (17.6)
16 (6.5)
91 (70.5)
30 (23.3)
8 (6.2)
0.129
938
957
943
1129
1262
1276
1306
(95.2)
(96.2)
(93.7)
(95.5)
(94.5)
(95.4)
(97.0)
29
23
33
33
51
47
29
(3.0)
(2.3)
(3.3)
(2.8)
(3.8)
(3.5)
(2.2)
15
15
30
20
22
15
12
(1.5)
(1.5)
(3.0)
(1.7)
(1.7)
(1.1)
(0.9)
<0.001
1673 (25.2)
4375 (66.0)
584 (8.8)
26 (11.7)
184 (82.5)
13 (5.8)
632
871
558
4815
935
115
50
17
32
31
19 (16.7)
86 (75.4)
9 (7.9)
<0.001
(8.1)
(11.2)
(7.1)
(61.6)
(12.0)
(46.9)
(20.4)
(6.9)
(13.1)
(12.7)
45
19
11
44
10
(34.9)
(14.7)
(8.5)
(34.1)
(7.8)
<0.001
439 (5.6)
5673 (72.6)
1699 (21.8)
51 (20.8)
187 (76.3)
7 (2.9)
4318 (55.3)
1562 (20.0)
1931 (24.7)
130 (53.1)
113 (46.1)
2 (0.8)
3807 (48.7)
1514 (19.4)
2490 (31.9)
165 (67.4)
68 (27.8)
12 (4.9)
463
5469
1879
0
24
150
71
41
24 (18.6)
94 (72.9)
11 (8.5)
<0.001
91 (70.5)
20 (15.5)
18 (14.0)
<0.001
89 (69.9)
17 (13.2)
23 (17.8)
0.004
(5.9)
(70.0)
(24.1)
(0)
(9.8)
(61.2)
(29.0)
(16.7)
<0.001
16
75
38
54
(12.4)
(58.1)
(29.5)
(41.9)
IQR = interquartile range; PSA = prostate-specific antigen; AJCC = American Joint Committee on Cancer; M1a = nonregional lymph nodes; M1b = bone
metastasis with or without lymph nodes; M1c = distant metastasis with or without bone and/or lymph node involvement; EBRT = external-beam radiation
therapy; NSR = no surgery or radiation therapy; RP = radical prostatectomy; BT = brachytherapy.
^
At the time of diagnosis.
a
Comparing NSR with RP patients.
b
Comparing NSR with BT patients.
c
Comparing NSR with the entire local therapy cohort.
1060
EUROPEAN UROLOGY 65 (2014) 1058–1066
[(Fig._1)TD$IG]
and 2010 using all 18 SEER-based registries. Only patients with
documented stage IV (M1a–c) disease at the time of diagnosis based
on the American Joint Committee on Cancer (AJCC) Cancer Staging
Manual, sixth edition, with either radiographic or pathologic confirmation of metastatic disease through the Collaborative Staging System,
were included [11]. Per SEER coding guidelines, age, marital status,
disease grade (low–moderate [Gleason score 7] or high [Gleason 8]),
and clinical AJCC T, N, and M stages were based on data obtained at the
time of diagnosis. Furthermore, the prostate-specific antigen (PSA)
measurement for each patient corresponded to the highest PSA value
recorded prior to diagnostic prostate biopsy and treatment. For each
subject, race was defined as white, African American, or other, and cause
of death (PCa or non-PCa) was based on the SEER cause-of-death
classification.
Cases were grouped based on no surgery or radiation therapy (NSR)
or definitive LT to the prostate (either radical prostatectomy [RP]
[surgery site codes 50 or 70] or brachytherapy [BT] [radiation-specific
codes 2, 3, or 4]). Within the LT group, men were not excluded if they
received adjuvant external-beam radiation therapy (EBRT). Cases
diagnosed by autopsy or death certificate only or with unknown
radiation therapy, surgery, or metastatic site were excluded. Patients
treated with endoscopic therapy (eg, cryotherapy, transurethral
resection) (n = 1312) or EBRT only (n = 2628) were excluded, since
these treatments did not coincide with the a priori definition of definitive
LT, the latter based on the lack of EBRT organ site–specific codes within
SEER. Incidentally, on initial analyses, survival in these patient groups
was inferior to NSR patients, possibly suggesting that these treatments
were used in a more palliative setting (eg, bone pain, urinary
obstruction).
Outcomes of interest included overall survival (OS) and diseasespecific survival (DSS), as well as factors independently associated with
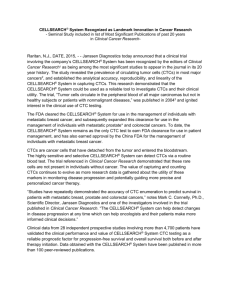
Fig. 1 – (A) Overall survival and (B) cumulative incidence of prostate
cancer (PCa)-specific mortality in patients with metastatic PCa at
diagnosis based on treatment received. For cumulative incidence of
cancer-specific mortality, analyses are adjusted for age at diagnosis;
race; initial prostate-specific antigen; tumor grade; American Joint
Committee on Cancer T, N, and M stages; year of diagnosis; and registry,
and account for the competing risk of non-PCa death. NSR = no surgery
or radiation therapy; RP = radical prostatectomy; BT = brachytherapy.
cause-specific mortality (CSM). Kaplan-Meier methods were used to
determine OS. Even with mPCa, patients can live many years after
diagnosis and may die from non-PCa causes. To account for this situation,
competing risks regression analysis, according to the model of Fine and
Gray [12], was used to calculate the cumulative incidence of PCa-specific
death and DSS probabilities using death from non-PCa as the competing
variable. Stepwise multivariable competing risks regression analysis was
used to identify factors independently associated with CSM using
backward elimination of variables based on the Wald test and a p value
0.20. Variables differing among patient groups were determined using
Pearson chi-square analysis. STATA v.12 (Stata Corp, College Station, TX,
USA) was used for all analyses, with a p value 0.05 considered
significant.
3.
Results
A total of 8185 eligible cases were identified, with a median
follow-up of 16 mo (interquartile range [IQR]: 7–31): NSR
(n = 7811), RP (n = 245), and BT (n = 129). Patient characteristics are listed in Table 1. A total of 3115 patients
(38.1%) died of PCa: 3048 NSR patients (40.7%), 33 RP
patients (13.5%), and 34 BT patients (26.4%). The 5-yr OS
was significantly higher in patients undergoing either RP
(67.4%; 95% confidence interval [CI], 58.7–74.7) or BT
(52.6%; 95% CI, 39.8–63.9) compared with NSR patients
(22.5%; 95% CI, 21.1–23.9) ( p < 0.001) (Fig. 1). In addition,
undergoing RP or BT was each independently associated
with decreased CSM, with predicted 5-yr DSS probabilities
of 75.8% and 61.3%, respectively, compared with 48.7% for
NSR patients (Fig. 1 and Table 2). In patients dying of nonPCa causes (1284 patients [15.7%]), no significant differences in survival were noted among groups. Although OS
was higher in RP patients compared with BT patients, there
was no significant difference in CSM between the two
groups (Fig. 1).
To account for patients who might benefit least from
LT—either because of progressive disease, significant
comorbidity, or a history of other primary malignancies
that might bias outcomes—analyses were repeated, but this
time excluding patients dying 12 mo from diagnosis
(n = 1813) or with multiple malignant primaries (n = 618).
At a median follow-up of 27 mo (IQR: 18–42), 5-yr OS
continued to be higher in patients undergoing RP (76.5%;
95% CI, 67.0–83.7) or BT (58.2%; 95% CI, 44.5–69.7)
compared with NSR patients (30.6%; 95% CI, 28.9–32.4)
( p < 0.001). Additionally, undergoing RP (subhazard ratio
[SHR]: 0.37; 95% CI, 0.26–0.54; p < 0.001) or BT (SHR: 0.57;
95% CI, 0.37–0.87; p = 0.01) was still each independently
associated with decreased CSM compared with NSR
patients, with 5-yr DSS probabilities of 75.1%, 64.5%, and
46.9%, respectively.
Factors independently associated with increased CSM in
LT patients included age 70 yr, cT4 disease, PSA 20 ng/ml,
high-grade disease, and pelvic lymphadenopathy (Table 3).
Five-year OS (77.3%; 95% CI, 67.4–84.5) and DSS probability
(89.9%) were highest in patients with one or fewer factors
(n = 181 [48.4%]). Although patients with two factors
(n = 116 [31.0%]) exhibited lower 5-yr OS (53.1%; 95% CI,
38.9–65.4) and lower DSS probability (68.7%), survival was
still better than for NSR patients. However, patients with
three or more factors (n = 77 [20.6%]) demonstrated a 5-yr
EUROPEAN UROLOGY 65 (2014) 1058–1066
[(Fig._2)TD$IG]
1061
Table 2 – Stepwise multivariable competing risks regression
analysis of patients with metastatic prostate cancer at diagnosis*
Characteristic
Adjusted
SHR
Type of treatment
No surgery or radiation
therapy
Radical prostatectomy
Brachytherapy
High-grade disease^
T4 disease^
(vs <T4 disease)
PSA 20 ng/ml^
(vs PSA <20 ng/ml)
AJCC N stage^
N0
N1
AJCC M stage^
M1a
M1b
M1c
Year of diagnosis
95% confidence
interval
p value
0.38
0.68
1.70
1.25
0.27–0.53
0.49–0.93
1.42–2.04
1.12–1.40
<0.001
0.018
<0.001
<0.001
1.29
1.20–1.40
<0.001
Ref
1.21
1.09–1.33
<0.001
Ref
1.86
2.35
0.93
1.55–2.24
1.94–2.85
0.91–0.95
<0.001
<0.001
<0.001
Ref
SHR = subhazard ratio; PSA = prostate-specific antigen; AJCC = American
Joint Committee on Cancer; Ref = reference; M1a = nonregional lymph
nodes; M1b = bone metastasis with or without lymph nodes; M1c =
distant metastasis with or without bone and lymph node involvement.
*
Surveillance Epidemiology and End Results, 2004–2010.
^
At the time of diagnosis.
Table 3 – Stepwise multivariable competing risks regression
analysis of patients with metastatic prostate cancer at diagnosis
undergoing definitive local therapy of the prostate*
Characteristic
Age, yr^
<70
70
AJCC T stage^
T1–T3
T4
Grade of disease^
Low
High
PSA, ng/ml^
<20
20
AJCC N stage^
N0
N1
AJCC M stage^
M1a
M1b
M1c
Adjusted
SHR
95% confidence
interval
Fig. 2 – Survival of patients with metastatic prostate cancer (PCa) at
diagnosis undergoing local therapy (LT) based on the number of factors
independently associated with an increase in PCa-specific mortality: T4
or high-grade disease, age I70 yr, PSA I20 ng/ml, and pelvic
lymphadenopathy. (A) Kaplan-Meier analysis demonstrating overall
survival; (B) cumulative incidence of PCa-specific mortality, accounting
for the competing risk of non-PCa and adjusted for race, American Joint
Committee on Cancer M stage, year of diagnosis, and registry. Patients
undergoing no surgery or radiation therapy (NSR) are listed as a
reference.
p value
Ref
2.31
1.44–3.72
0.001
Ref
2.09
1.05–4.18
0.037
Ref
3.79
1.30–11.07
0.015
Ref
2.24
1.37–3.66
0.001
Ref
3.13
1.60–6.12
0.001
Ref
3.32
3.66
1.23–9.01
1.23–10.84
0.018
0.019
SHR = subhazard ratio; Ref = reference; AJCC = American Joint Committee
on Cancer; PSA = prostate-specific antigen.
Surveillance Epidemiology and End Results, 2004–2010.
^
At the time of diagnosis.
*
OS survival (38.2%; 95% CI, 24.4–51.9) and a DSS probability
(50.1%) similar to NSR patients (Fig. 2).
Subset analyses were performed to determine if survival
differed among groups based on age (<70 vs 70 yr) or
PSA (<20 vs 20 ng/ml), since previous studies have
demonstrated poorer survival in metastatic disease in
older patients (75 yr) [13,14] and in patients with PSA
20 ng/ml [15]. Although both OS and DSS probabilities
were significantly higher in patients <70 yr, only OS was
significantly better in patients 70 yr undergoing LT
compared with NSR patients (Fig. 3 and Table 4). OS and
DSS probability were significantly higher in RP or BT
patients with PSA <20 ng/ml. However, although both RP
and BT demonstrated a significantly higher OS in patients
with PSA 20 ng/ml, only RP patients demonstrated
significantly decreased CSM compared with NSR patients
(Fig. 4 and Table 4).
To determine if the extent of metastatic disease affected
survival among groups, subset analyses were performed
based on AJCC M stage (M1a–c) (Fig. 5 and Table 4).
Compared with NSR patients, men undergoing RP exhibited
decreased CSM regardless of M stage and a higher OS in M1b
and M1c disease. In BT patients, OS was higher regardless of
M stage, and CSM was decreased in men with M1c disease.
There were no significant differences in survival among
groups based on individual AJCC M stage in patients dying of
non-PCa causes.
4.
Discussion
PCa is the most commonly diagnosed cancer and the second
leading cause of death from cancer in American men.
Historically, approximately 25% of men presented with
1062
EUROPEAN UROLOGY 65 (2014) 1058–1066
Table 4 – Subset analyses of survival of patients with metastatic prostate cancer at diagnosis based on age, prostate-specific antigen, or
American Joint Committee on Cancer M stage and treatment received*
Age, yr
<70
NSR
RP
BT
70
NSR
RP
BT
PSA, ng/ml
<20
NSR
RP
BT
20
NSR
RP
BT
AJCC M stage*
M1a
NSR
RP
BT
M1b
NSR
RP
BT
M1c
NSR
RP
BT
No. (%)
Adjusted
SHR
95% CI
p value
5-yr
OS, %
95% CI
DSS, yra
p value
1
3
5
3324 (42.6)
202 (82.4)
74 (57.4)
Ref
0.26
0.55
0.17–0.39
0.34–0.88
<0.001
0.014
28.9
71.2
57.4
26.6–31.3
61.6–78.9
22.6–66.6
<0.001
<0.001
86.1
96.7
92.2
57.7
86.9
73.9
45.8
82.0
65.2
5047 (57.6)
46 (17.3)
63 (43.5)
Ref
0.65
0.67
0.37–1.12
0.43–1.03
0.120
0.070
18.1
50.3
48.5
16.5–19.8
30.1–67.5
30.0–64.7
<0.001
<0.001
80.1
86.7
86.2
58.6
70.8
69.9
49.5
63.5
62.5
No. (%)
Adjusted
SHR^
5-yr
OS, %
95% CI
p value
95% CI
p value
DSS, yrb
1
3
5
1503 (21.9)
165 (77.1)
64 (53.8)
Ref
0.26
0.36
0.15–0.45
0.18–0.72
<0.001
0.004
33.7
77.1
71.2
30.4–37.1
66.1–85.0
46.8–85.9
<0.001
<0.001
87.3
96.5
95.3
66.6
89.9
86.5
57.9
86.7
82.3
5373 (78.1)
49 (22.9)
55 (46.2)
Ref
0.58
0.91
0.34–0.97
0.63–1.33
0.039
0.633
19.8
55.7
37.3
18.2–21.5
37.1–70.9
21.4–53.2
<0.001
0.027
81.4
88.8
82.9
55.6
71.3
58.5
44.8
63.0
48.1
No. (%)
Adjusted
SHR^
5-yr
OS, %
95% CI
p value
95% CI
p value
DSS, yrc
1
3
5
463 (5.9)
24 (9.8)
16 (12.4)
Ref
0.24
0.56
0.06–0.95
0.20–1.58
0.043
0.272
35.1
64.3
54.7
28.0–42.3
38.7–81.4
8.6–86.2
0.064
0.014
93.4
98.4
96.3
73.3
92.9
84.1
61.4
89.1
76.2
5469 (70.0)
150 (61.2)
75 (58.1)
Ref
0.35
0.74
0.22–0.55
0.42–1.05
<0.001
0.078
22.9
70.1
55.0
21.2–24.6
58.1–79.2
31.1–64.5
<0.001
<0.001
84.1
94.1
89.2
59.6
83.4
71.0
48.4
77.6
61.9
1879 (24.1)
71 (29.0)
38 (29.5)
Ref
0.33
0.56
0.19–0.57
0.34–0.94
<0.001
0.027
18.6
60.7
53.4
16.1–21.2
42.7–74.6
34.4–69.2
<0.001
<0.001
75.6
91.1
85.4
50.4
80.0
68.3
43.0
75.6
62.1
SHR = subhazard ratio; M1a = nonregional lymph nodes; M1b = bone metastasis with or without lymph nodes; M1c = distant metastasis with or without bone
and lymph node involvement; OS = overall survival; CI = confidence interval; DSS = disease-specific survival; NSR = no surgery or radiation therapy; RP = radical
prostatectomy; BT = brachytherapy; PSA = prostate-specific antigen; AJCC = American Joint Committee on Cancer; Ref = reference.
*
Based on multivariable competing risks regression analysis using death from non–prostate cancer as the competing variable.
a
Adjusted for race; registry; year of diagnosis; PSA; and AJCC T, N, and M stages.
b
Adjusted for age; race; registry; year of diagnosis; and AJCC T, N, and M stages.
c
Adjusted for age, race, registry, year of diagnosis, PSA, and AJCC T and N stages.
either metastatic or lymph node–positive disease. However,
because of PSA screening and associated stage migration,
<5% of men currently present with synchronous metastatic
disease [16]. Although RP and radiation therapy (BT,
conformal radiation therapy, and intensity-modulated
radiation therapy [IMRT]) are routinely used for the
treatment of organ-confined or locally advanced disease,
ADT remains the standard initial management for patients
diagnosed with metastatic disease. Despite the ability of
ADT to prolong survival and curtail disease-related symptoms, resistance to hormone therapy ultimately develops.
The introduction of newer, more novel agents, including
sipuleucel-T [17], abiraterone [18], cabazitaxel [19], and
enzalutamide [20], has shown improvement in survival.
However, 5-yr survival for men with metastatic disease is
only 28%, in stark contrast to nearly 100% for men diagnosed
without mPCa [21].
Decreasing tumor burden, through cytoreductive surgery, radiation, or both, improves survival in a number of
malignancies. In particular, studies demonstrate that
maximal cytoreduction improves survival in patients with
breast cancer [5], colon cancer [3], and ovarian cancer [4], in
addition to increasing tumor response to systemic chemotherapy. Furthermore, treatment of the primary tumor itself
has been associated with improved survival in patients
diagnosed with glioblastoma [8], colon cancer [9], and renal
cell carcinoma [6,7].
Although prospective data do not exist regarding a
survival benefit for patients with mPCa undergoing
treatment of the primary tumor, there are retrospective
EUROPEAN UROLOGY 65 (2014) 1058–1066
[(Fig._3)TD$IG]
1063
Fig. 3 – Overall survival (left column) and cumulative incidence of prostate cancer (PCa)-specific mortality (right column) in patients with metastatic PCa
at diagnosis based on age ([A] <70 yr and [B] I70 yr) and treatment received. For cumulative incidence of cancer-specific mortality, analyses are adjusted
for race; prostate-specific antigen; tumor grade; American Joint Committee on Cancer T, N, and M stages; year of diagnosis; and registry, and account for
the competing risk of non–PCa death. NSR = no surgery or radiation therapy; RP = radical prostatectomy; BT = brachytherapy.
[(Fig._4)TD$IG]
Fig. 4 – Overall survival (left column) and cumulative incidence of prostate cancer (PCa)-specific mortality (right column) in patients with metastatic PCa
at diagnosis based on prostate-specific antigen level ([A] <20 ng/ml and [B] I20 ng/ml) and treatment received. For cumulative incidence of cancerspecific mortality, analyses are adjusted for race; age; tumor grade; American Joint Committee on Cancer T, N, and M stages; year of diagnosis; and
registry and account for the competing risk of non-PCa death. NSR = no surgery or radiation therapy; RP = radical prostatectomy; BT = brachytherapy (BT).
1064
[(Fig._5)TD$IG]
EUROPEAN UROLOGY 65 (2014) 1058–1066
Fig. 5 – Overall survival (left column) and cumulative incidence of prostate cancer (PCa)–specific mortality (right column) in patients with metastatic PCa
at diagnosis based on American Joint Committee on Cancer M stage [M1a, M1b, or M1c] and treatment received. For cumulative incidence of cancerspecific mortality, analyses are adjusted for age, race, prostate-specific antigen, tumor grade, AJCC T and N stages, year of diagnosis, and registry, and
account for the competing risk of non-PCa death. NSR = no surgery or radiation therapy; RP = radical prostatectomy; BT = brachytherapy.
studies that do indicate improved outcome with prostate
tumor cytoreduction [22–24]. In particular, investigators at
the Mayo Clinic evaluated 79 matched pairs of patients with
pTxN+ PCa undergoing either RP with pelvic lymph node
dissection (PLND) plus orchiectomy within 3 mo of surgery
or PLND with orchiectomy only [23]. They found that
patients undergoing RP with orchiectomy demonstrated
both a higher OS (66% vs 28%; p < 0.001) and a higher DSS
(79% vs 39%; p < 0.001) compared with patients undergoing
orchiectomy alone [23]. In a population-based study using
the Munich Cancer Registry, Engel et al. examined the OS
and relative survival of patients with node-positive disease
undergoing RP (n = 688) in comparison with patients in
whom RP was aborted (n = 250) [24]. Recognizing that there
was a higher number of positive lymph nodes in the aborted
RP group, 10-yr OS (64% vs 28%) and relative survival
(86% vs 40%) were still higher in the RP group. In addition,
on multivariable analysis, not undergoing RP was an
independent predictor of decreased survival (hazard ratio:
2.04; 95% CI, 1.59–2.63; p < 0.0001) [24]. Finally, studies
have shown an increased response to ADT and newer agents
(eg, sipuleucel-T) in patients with metastatic disease who
had undergone prior RP [25–27].
To our knowledge, this is the first population-based
analysis to suggest a possible survival benefit of primary
treatment of the prostate in men diagnosed with mPCa. Our
results demonstrate that patients undergoing definitive
treatment of the prostate (either through RP or BT with or
without adjuvant pelvic radiotherapy) had a higher 5-yr OS
and DSS probability compared with patients not undergoing
LT. It is important to note that in men who died of non-PCa
causes, no survival differences were noted based on
treatment compared with no treatment.
We noted that features independently associated with
increased CSM in patients undergoing LT included age 70
yr, high-grade and high-stage (T4) disease, PSA 20 ng/ml,
and pelvic lymphadenopathy. Consistent with previous
reports demonstrating poorer survival in patients with
metastatic disease who were older or had a higher PSA,
subset analyses in our study demonstrated that patients
EUROPEAN UROLOGY 65 (2014) 1058–1066
70 yr and patients with PSA 20 ng/ml were less likely to
benefit from LT [13–15]. In terms of AJCC T and N stages,
although resection of bulky tumor or lymph nodes is
certainly achievable, the potential for leaving disease
behind is greater, which might negate any beneficial effects
of primary tumor cytoreduction. Because of the small
sample size of patients undergoing LT in the current study,
questions regarding benefit with respect to modality
(surgery vs radiation therapy) based on the previously
described factors would be best answered in a prospective
trial.
Mechanisms underlying a survival benefit of cytoreductive treatment remain unknown. Possible explanations in
mPCa include removing tumor-promoting factors and
immunosuppressive cytokines; decreasing the total tumor
burden and thus allowing for an improved response to ADT
and/or chemotherapy; eliminating the primary source of
the dissemination of metastatic cells; and/or eliminating
the primary site, which data have indicated can also be a site
of metastasis through the ‘‘self-seeding’’ hypothesis [28].
Studies have shown that increased circulating tumor cells
are associated with tumor progression and reduced survival
[29]. Removal of the prostate may therefore reduce the
number of circulating tumor cells.
Finally, the most significant findings from this study
were that survival of patients undergoing LT was still
improved regardless of the extent of metastases and that
death from non-PCa causes did not differ among groups
on the whole or based on AJCC M stage. Although the
baseline expectation would be that the greatest benefit
would be seen only in patients with M1a disease, not only
was improved survival noted in patients with either M1b
or M1c disease, but also the difference was most
pronounced in patients with M1c disease. If true, this
finding would be critical for patient enrollment in
prospective clinical trials.
SEER is the only comprehensive population-based
database in the United States that includes disease stage
and grade at the time of diagnosis, initial treatments
performed, and accurate data regarding patient survival. As
such, SEER represents an ideal approach to studying the
survival of patients diagnosed with mPCa in the United
States, especially in recent time periods. We chose to
include only patients diagnosed between 2004 and 2010, as
this time period represented the most up-to-date and
comprehensive collection of validated data regarding PCa
based on the Collaborative Staging System (eg, sites of
metastasis, PSA, surgery-specific coding) and correlated
with the most recent standard of care for patients with
metastatic disease (eg, docetaxel-based chemotherapy and
ADT). In fact, we noted that a more recent year of diagnosis
was associated with decreased CSM in the entire cohort,
likely representing the positive impact of improved agents.
Nonetheless, variables unavailable from SEER undoubtedly
limited our analysis and precluded controlling for any
selection bias that might exist. These variables include
patient performance status, comorbidity, site-specific EBRT
codes, timing and dosage of chemotherapy and/or ADT, and
the use of ADT relative to surgery or BT. The lack of ADT
1065
information is especially important given the influence of
ADT on PCa progression and survival. Finally, SEER lacks
information regarding the extent of bony metastasis, an
entity that undoubtedly influences patient survival.
5.
Conclusions
Despite the inherent limitations of this SEER-based study,
our results suggest that LT for the primary tumor confers a
survival advantage in patients with mPCa at diagnosis.
Because of the lack of site-specific EBRT codes, it was not
possible to examine the effects of IMRT or other forms of
prostate-directed EBRT on patient survival. However, we
would hypothesize that dedicated treatment of the primary
tumor by EBRT would confer similar survival benefits, since
level 1 evidence has shown that ADT plus radiation therapy
compared with ADT alone confers a survival advantage
among patients with high-risk disease and an increased risk
of micrometastases [30]. Although our results are based on
data collected prospectively, our analyses are still retrospective, which limits our ability to fully conclude that
localized treatment of the primary tumor should be part of
the multidisciplinary management of patients with mPCa.
As such, we do not advocate LT based on these data alone
but instead in the context of organized prospective clinical
trials designed not only to demonstrate a survival benefit
with LT of the primary tumor but also to identify patients
most likely to benefit.
Author contributions: Stephen H. Culp had full access to all the data in
the study and takes responsibility for the integrity of the data and the
accuracy of the data analysis.
Study concept and design: Culp, Schellhammer, Williams.
Acquisition of data: Culp.
Analysis and interpretation of data: Culp, Schellhammer, Williams.
Drafting of the manuscript: Culp, Schellhammer, Williams.
Critical revision of the manuscript for important intellectual content: Culp,
Schellhammer, Williams.
Statistical analysis: Culp.
Obtaining funding: None.
Administrative, technical, or material support: Culp, Schellhammer,
Williams.
Supervision: Culp, Schellhammer, Williams.
Other (specify): None.
Financial disclosures: Stephen H. Culp certifies that all conflicts of
interest, including specific financial interests and relationships and
affiliations relevant to the subject matter or materials discussed in the
manuscript (eg, employment/affiliation, grants or funding, consultancies, honoraria, stock ownership or options, expert testimony, royalties,
or patents filed, received, or pending), are the following: None.
Funding/Support and role of the sponsor: None.
References
[1] Scardino P. Update: NCCN prostate cancer clinical practice guidelines. JNCCN 2005;3(Suppl 1):S29–33.
[2] Loblaw DA, Virgo KS, Nam R, et al. Initial hormonal management of
androgen-sensitive metastatic, recurrent, or progressive prostate
cancer: 2006 update of an American Society of Clinical Oncology
practice guideline. J Clin Oncol 2007;25:1596–605.
1066
EUROPEAN UROLOGY 65 (2014) 1058–1066
[3] Glehen O, Mohamed F, Gilly FN. Peritoneal carcinomatosis from
[17] Small EJ, Schellhammer PF, Higano CS, et al. Placebo-controlled
digestive tract cancer: new management by cytoreductive surgery
phase III trial of immunologic therapy with sipuleucel-T (APC8015)
and intraperitoneal chemohyperthermia. Lancet Oncol 2004;5:
in patients with metastatic, asymptomatic hormone refractory
219–28.
prostate cancer. J Clin Oncol 2006;24:3089–94.
[4] Bristow RE, Tomacruz RS, Armstrong DK, Trimble EL, Montz FJ.
[18] de Bono JS, Logothetis CJ, Molina A, et al. Abiraterone and increased
Survival effect of maximal cytoreductive surgery for advanced
survival in metastatic prostate cancer. N Engl J Med 2011;364:
ovarian carcinoma during the platinum era: a meta-analysis. J Clin
Oncol 2002;20:1248–59.
1995–2005.
[19] de Bono JS, Oudard S, Ozguroglu M, et al. Prednisone plus cabazi-
[5] Polychemotherapy for early breast cancer: an overview of the
taxel or mitoxantrone for metastatic castration-resistant prostate
randomised trials. Early Breast Cancer Trialists’ Collaborative
cancer progressing after docetaxel treatment: a randomised open-
Group. Lancet 1998;352:930–42.
label trial. Lancet 2010;376:1147–54.
[6] Flanigan RC, Salmon SE, Blumenstein BA, et al. Nephrectomy fol-
[20] Scher HI, Fizazi K, Saad F, et al. Increased survival with enzaluta-
lowed by interferon alfa-2b compared with interferon alfa-2b alone
mide in prostate cancer after chemotherapy. N Engl J Med 2012;
for metastatic renal-cell cancer. N Engl J Med 2001;345:1655–9.
[7] Mickisch GH, Garin A, van Poppel H, de Prijck L, Sylvester R. Radical
nephrectomy plus interferon-alfa-based immunotherapy compared with interferon alfa alone in metastatic renal-cell carcinoma:
a randomised trial. Lancet 2001;358:966–70.
[8] Nitta T, Sato K. Prognostic implications of the extent of surgical
resection in patients with intracranial malignant gliomas. Cancer
1995;75:2727–31.
367:1187–97.
[21] American Cancer Society. Cancer facts and figures 2013. Atlanta,
GA: American Cancer Society; 2013.
[22] Steuber T, Budaus L, Walz J, et al. Radical prostatectomy improves
progression-free and cancer-specific survival in men with lymph
node positive prostate cancer in the prostate-specific antigen era: a
confirmatory study. BJU Int 2011;107:1755–61.
[23] Ghavamian R, Bergstralh EJ, Blute ML, Slezak J, Zincke H. Radical
[9] Temple LK, Hsieh L, Wong WD, Saltz L, Schrag D. Use of surgery
retropubic prostatectomy plus orchiectomy versus orchiectomy
among elderly patients with stage IV colorectal cancer. J Clin Oncol
alone for pTxN+ prostate cancer: a matched comparison. J Urol
2004;22:3475–84.
1999;161:1223–7, discussion 1227–8.
[10] Harlan LC, Hankey BF. The surveillance, epidemiology, and end-
[24] Engel J, Bastian PJ, Baur H, et al. Survival benefit of radical prosta-
results program database as a resource for conducting descriptive
tectomy in lymph node-positive patients with prostate cancer. Eur
epidemiologic and clinical studies. J Clin Oncol 2003;21:2232–3.
Urol 2010;57:754–61.
[11] Greene FL, Page DL, Fleming ID, et al. AJCC cancer staging handbook:
[25] Swanson GP, Riggs M, Earle J. Failure after primary radiation or
TNM classification of malignant tumors. ed. 6. New York, NY: Springer-
surgery for prostate cancer: differences in response to androgen
Verlag; 2002.
[12] Fine JP, Gray RJ. A proportional hazards model for the subdistribution of a competing risk. J Am Stat Assoc 1999;94:496–509.
[13] Humphreys MR, Fernandes KA, Sridhar SS. Impact of age at diagnosis on outcomes in men with castrate-resistant prostate cancer
(CRPC). J Cancer 2013;4:304–14.
[14] Scosyrev E, Messing EM, Mohile S, Golijanin D, Wu G. Prostate
cancer in the elderly: frequency of advanced disease at presentation and disease-specific mortality. Cancer 2012;118:3062–70.
ablation. J Urol 2004;172:525–8.
[26] Thompson IM, Tangen C, Basler J, Crawford ED. Impact of previous
local treatment of prostate cancer on subsequent metastatic disease. J Urol 2002;168:1008–12.
[27] Kantoff PW, Higano CS, Shore ND, et al. Sipuleucel-T immunotherapy for castration-resistant prostate cancer. N Engl J Med 2010;363:
411–22.
[28] Comen E, Norton L, Massague J. Clinical implications of cancer selfseeding. Nat Rev Clin Oncol 2011;8:369–77.
[15] Bertaglia V, Tucci M, Fiori C, et al. Effects of serum testosterone
[29] Resel Folkersma L, San Jose Manso L, Galante Romo I, Moreno Sierra
levels after 6 months of androgen deprivation therapy on the
J, Olivier Gomez C. Prognostic significance of circulating tumor cell
outcome of patients with prostate cancer. Clin Genitourin Cancer
count in patients with metastatic hormone-sensitive prostate can-
2013;11:325–30.
cer. Urology 2012;80:1328–32.
[16] Ryan CJ, Elkin EP, Small EJ, Duchane J, Carroll P. Reduced incidence
[30] Warde P, Mason M, Ding K, et al. Combined androgen deprivation
of bony metastasis at initial prostate cancer diagnosis: data from
therapy and radiation therapy for locally advanced prostate cancer:
PCaSURE. Urol Oncol 2006;24:396–402.
a randomised, phase 3 trial. Lancet 2011;378:2104–11.