Function of reinserted abductor muscles after femoral replacement
advertisement

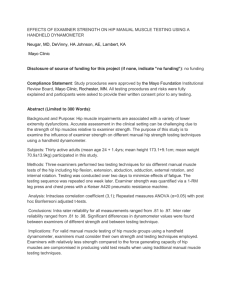
Function of reinserted abductor muscles after femoral replacement A. Giurea, T. Paternostro, G. Heinz-Peer, A. Kaider, F. Gottsauner-Wolf From the University of Vienna, Austria e compared two methods of reconstruction of the abductor mechanism in 15 patients after prosthetic replacement of the upper femur, to assess abductor strength and function. Six patients in group I had direct fixation of the gluteus medius tendon and a segment of the original bone to the prosthesis. Nine patients in group 2 had the abductor tendon fixed to the iliotibial band. We assessed clinical function, isometric muscle strength and muscle cross-sectional area for each patient. The patients in group 1 had better clinical and functional results (p = 0.059), with average peak torques for hip abduction of 92% of that in the non-operated leg in group 1, and of 57% in group 2. Group 1 had a mean muscle cross-sectional area of 69% and a mean value of strength per cross-sectional area of 134% when compared with the control side. The respective values for group 2 were 52% and 91%. Direct fixation of the abductor muscles to the prostheses gave improved function and higher isometric abductor muscle force. W J Bone Joint Surg [Br] 1998;80-B:284-7. Received 18 July 1997; Accepted 13 August 1997 Prosthetic replacement of the upper femur after tumour resection or at revision arthroplasty of the hip may be 1-3 associated with considerable loss of muscle function. The resection of malignant bone tumours often requires extensive removal of soft tissues. The reconstruction of bone defects with megaprostheses A. Giurea, MD, Consultant F. Gottsauner-Wolf, MD, Associate Professor Department of Orthopaedics T. Paternostro, MD, Consultant Department of Physical Medicine and Rehabilitation G. Heinz-Peer, MD, Consultant Department of Radiology A. Kaider, MSc, Statistician Department of Medical Computer Science University of Vienna, Währinger-Gürtel 18, A-1090 Vienna, Austria. Correspondence should be sent to Dr F. Gottsauner-Wolf. ©1998 British Editorial Society of Bone and Joint Surgery 0301-620X/98/28179 $2.00 284 is well established, but there are technical problems with 3-6 the attachment of muscles and tendons to the prosthesis. Inadequate reattachment will cause considerable loss of 5 function and loss of joint stability. Various techniques have 6,7 been devised, but the treatment of tumours produces special problems, and soft-tissue attachment with or with6,7 out the use of bone blocks is not always successful. We studied the differences between two surgical methods of refixation of the gluteus medius. In one group the gluteal muscles were fixed to the iliotibial band and in the other they were attached directly to the prosthesis. Patients and Methods We investigated 15 patients following the prosthetic replacement of the femur with reconstruction of gluteus medius, after an average of 44 months (12 to 92). There were four men and 11 women with a mean age at operation of 36 years (10 to 83). Five patients had total replacement of the femur and ten replacement of only the proximal part. The resections were for malignant bone tumours in 12 and as part of a revision hip arthroplasty in three (Table I). The KMFTR-prosthetic system (Kotz Modular Femur and Tibia Reconstruction System; Howmedica, Kiel, Germany) was used in each patient. The 32 mm head was of aluminium oxide ceramic. Either a titanium-alloy conical threaded cup (CSF, Allo Pro; Sulzer Medical, Winterthur, Switzerland) or a cemented polyethylene cup (Müller; Protek, Winterthur, Switzerland) was used. When acetabular reconstruction was not required we used a bipolar head (Howmedica, Rutherford, New Jersey). The six patients in group 1 had reattachment of the medial gluteal tendon to the prosthesis using a bone block Table I. Indications for femoral replacement in 15 patients Total Tumour 12 Ewing's sarcoma 5 Osteogenic sarcoma 4 Metastases 2 Malignant fibrous histiocytoma 1 Revision Total Proximal femoral replacement 7 3 1 2 1 Total femoral replacement 5 2 3 --- 3 3 -- 15 10 5 THE JOURNAL OF BONE AND JOINT SURGERY FUNCTION OF REINSERTED ABDUCTOR MUSCLES AFTER FEMORAL REPLACEMENT 285 Surgical techniques for reconstruction of the gluteus medius. Figure 1a – Group 1: a bone block from the greater trochanter with the insertion of gluteus medius is fixed by a polyethylene spiked plate and screws to a KMFTR prosthesis. Figure 1b – Group 2: reattachment of gluteus medius to the iliotibial band. Fig. 1a Fig. 1b 8 Table II. Functional evaluation system according to Enneking et al Score Pain Function Emotional acceptance Supports Walking Gait 5 4 3 2 1 0 None Intermediate Modest Intermediate Moderate Severe No restriction Intermediate Recreational restriction Intermediate Partial disability Total disability Enthusiastic Intermediate Satisfied Intermediate Accepts Dislikes None Intermediate Brace Intermediate Cane or crutch Canes or crutches Unlimited Intermediate Limited Intermediate Indoors only Unable unaided Normal Intermediate Minor cosmetic Intermediate Major cosmetic Major handicap Fig. 2b Fig. 2a which included the natural insertion; four patients had fixation by a spiked polyethylene plate and two screws, which is provided routinely with the prosthesis (Fig. 1a). The nine patients in group 2 had gluteus medius sutured to the iliotibial band with no direct fixation to the endoprosthesis (Fig. 1b). All patients were examined clinically and radiologically, 8 using the evaluation system of Enneking et al (Table II). The isometric muscle strength of hip abduction and of foot dorsiflexion were measured in both legs of 13 patients by computerised dynamometry using a Cybex 6000 testing 9-12 machine (Lubex Inc, Ronkonkoma, New York). Two VOL. 80-B, NO. 2, MARCH 1998 CT scans of a 20-year-old woman with endoprosthetic replacement of the left proximal femur showing (a) a scout view with the levels indicated and (b) the cross-sectional area of gluteus medius and gluteus maximus on the control side (1 and 2) and on the operated side (4 and 3). patients, one aged 80 years (group 1) and the other aged 91 years (group 2), were unable to perform the dynamometric tests. The tests were repeated three times on each leg and the highest peak torque was recorded as the isometric muscle strength. The foot dorsiflexion was tested to assess any overall weakness within the operated leg caused by postoperative immobilisation. In 11 patients, the cross-sectional area of the gluteus medius was measured on each side from CT scans (Tomoscan SR 7000; Philips, Eindhoven, The Netherlands) (Fig. 2). From three to five scans were taken in steps of 10 mm starting at the proximal end of the endoprosthesis, the 286 A. GIUREA, T. PATERNOSTRO, G. HEINZ-PEER, Table III. Clinical results showing the percentages of patients with excellent and good results on the system 8 of Enneking et al Group 1 (n = 6) 2 (n = 9) Pain Function Emotional acceptance Supports Walking Gait 83 67 83 67 83 67 89 56 89 56 78 33 Total rating 71 59 A. KAIDER, F. GOTTSAUNER-WOLF compared with the control side (Fig. 4). The strength of hip abduction per unit of cross-sectional area in group 1 was 134% (58 to 272) of that on the control side, and in group 2 91% (33 to 182) (p = 0.21; Fig. 4). Discussion Clinical evaluation showed an average Enneking rating of 71% (20 to 97) in group 1 and of 59% (37 to 77) in group 2 (p = 0.059) (Table III). All the implants were radiologically stable with no signs of loosening. The isometric muscle strength of hip abduction in group 1 (five patients) showed a mean peak torque of 92% (30 to 185) compared with the non-operated leg. The corresponding value in group 2 (eight patients) was 57% (20 to 99) (Fig. 3), but the difference did not reach statistical significance (p = 0.18). The mean peak force was 65.6 Nm (24 to 142) in group 1 and 39.2 Nm (14 to 72) in group 2. The mean peak torque of foot dorsiflexion was 98% (51 to 158) in group 1 and 88% (55 to 171) in group 2, again compared with the non-operated leg (p = 0.38; Fig. 3). The mean cross-sectional area of the gluteus medius on the operated side was 69% (42 to 89) in group 1 (five patients) and 52% (0 to 88) in group 2 (six patients) when Direct fixation of the gluteus medius to the prosthesis gave improved overall clinical outcomes, particularly of gait. The refixation of muscles to the prosthesis appeared to improve the quality of life and reduce the need for external aids. Isometric measurement of muscle force has been reported to correlate well with the function of the replaced hip as 1 assessed by gait analysis. We found that isometric muscle strength was greater in group 1 after direct muscle fixation to the prosthesis, and also found that gluteus medius had a larger mean cross-sectional area in this group. This may have been due to greater activity in the reinserted muscle, although loss of the muscle which had been resected could have influenced the result. There was, however, also a higher muscle strength per unit of cross-sectional area in group 1. Other factors which affect muscle function include 13,14 and the positioning of the the use of physiotherapy 2,9,15 prosthesis which we did not assess. Muscles which were not fixed to the prosthesis, but to the tensor fascia, showed reduced strength per unit of crosssectional area compared with muscles attached to the prosthesis. The power of abduction is greater when there is 7,12,16 direct transfer of load to the femoral prosthesis. The fixation is better and the risk of dislocation, very real after 5 tumour resection, is probably also reduced. We recommend that the remaining greater trochanter with the insertion of the gluteal tendon is fixed directly to a femoral prosthesis. This is feasible in most revision arthroplasties; tumour prostheses can usually be adapted to allow such fixation of muscle and tendon. When malignant tumours are resected, the bony insertions of the abductor muscles are usually removed with the tumour to achieve safe surgical margins. Despite this, we recommend the refixation of remaining soft tissue directly Fig. 3 Fig. 4 Box plots (±SD) for isometric muscle strength (Nm) of hip abduction and foot dorsiflexion in both groups, as percentages of the normal side. Box plots (±SD) for the cross-sectional area of gluteus medius and strength per cross-sectional area in both groups, as percentages of the normal side. circumferences of the gluteal muscles were digitised and 2 the area was calculated in mm . The data from the operated side were compared with those from the non-operated side, and the muscle strength of hip abduction was normalised to the cross-sectional area of the gluteus medius. For statistical analysis we used exact Wilcoxon rank-sum tests to compare differences between the two groups. A p value <0.05 was considered significant. Results THE JOURNAL OF BONE AND JOINT SURGERY FUNCTION OF REINSERTED ABDUCTOR MUSCLES AFTER FEMORAL REPLACEMENT to the prosthesis, provided that an appropriate means of fixation is available. This should provide stable initial attachment and have a porous coating to allow secondary biological ingrowth of bone. It has been shown experimentally that appropriate techniques can achieve a biological 7 link between muscle, tendon, and prosthesis, but that this provided only about one-third of the pull-out strength 7 recorded for bone-block fixation. No benefits in any form have been received or will be received from a commercial party related directly or indirectly to the subject of this article. References 1. Berman AT, Bosacco SJ, Israelite C. Evaluation of total knee arthroplasty using isokinetic testing. Clin Orthop 1991;271:106-13. 2. Delp SL, Wixson RL, Komattu AV, Kocmond JH. How superior placement of the joint center in hip arthroplasty affects the abductor muscles. Clin Orthop 1996;328:137-46. 3. Chao EY, Sim FH. Modular prosthetic system for segmental bone and joint replacement after tumor resection. Orthopedics 1985;8:641-51. 4. Kotz R, Ritschl P, Trachtenbrodt J. A modular femur tibia reconstruction system. Orthopaedics 1986;9:1639-52. 5. Sim FH, Chao EYS. Hip salvage by proximal femoral replacement. J Bone Joint Surg [Am] 1981;63-A:1228-39. 6. Gottsauner-Wolf F, Egger EL, Markel MD, Schultz FM, Chao EYS. Fixation of canine tendons to metal. Acta Orthop Scand 1994;65:179-84. 7. Gottsauner-Wolf F, Egger EL, Schultz FM, Sim FH, Chao EY. Tendons attached to prostheses by tendon-bone block fixation: an experimental study in dogs. J Orthop Res 1994;12:814-21. VOL. 80-B, NO. 2, MARCH 1998 287 8. Enneking WF, Dunham W, Gebhardt MC, Malawar M, Pritchard DJ. A system for the functional evaluation of reconstructive procedures after surgical treatment of tumours of the musculoskeletal system. Clin Orthop 1993;286:241-6. 9. McGrory BJ, Morrey BF, Cahalan TD, An KN, Cabanela ME. Effect of femoral offset on range of motion and abductor muscle strength after total hip arthroplasty. J Bone Joint Surg [Br] 1995; 77-B:865-9. 10. Petschnig R, Baron R, Kotz R, Ritschl P, Engel A. Muscle function after endoprosthetic replacement of the proximal tibia: different techniques for extensor reconstruction in 17 tumor patients. Acta Orthop Scand 1995;66:266-70. 11. Tsuboyama T, Windhager R, Dock W, et al. Knee function after operation for malignancy of the distal femur: quadriceps muscle mass and knee extension strength in 21 patients with hinged endoprostheses. Acta Orthop Scand 1993;64:673-7. 12. Minns RJ, Crawford RJ, Porter ML, Hardinge K. Muscle strength following total hip arthroplasty: a comparison of trochanteric osteotomy and the direct lateral approach. J Arthroplasty 1993;8:625-7. 13. Johnsson RA, Carlsson A, Kisch K, et al. Function following mega total hip arthroplasty compared with conventional total hip arthroplasty and healthy matched controls. Clin Orth Rel Res 1985; 192:159-67. 14. Horstmann T, Martini F, Mayer F, Sell S, Knak J, Zacher J. Strength of muscles surrounding the hip joint and gait in patients following implantation of a cementless hip endoprosthesis. Z Orthop Ihre Grenzgeb 1995;133:562-7. 15. Huang CH, Cheng CK, Lee YT, Lee KS. Muscle strength after successful total knee replacement: a 6- to 13-year follow-up. Clin Orthop 1996;328:147-54. 16. Horwitz BR, Rockowitz NL, Goll SR, et al. A prospective randomized comparison of two surgical approaches to total hip arthroplasty. Clin Orthop 1993;291:154-63.