Oxytocin infusion - Women and Newborn Health Service
advertisement

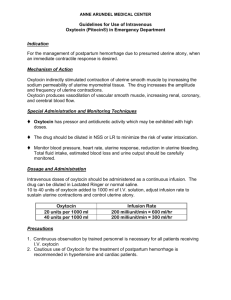
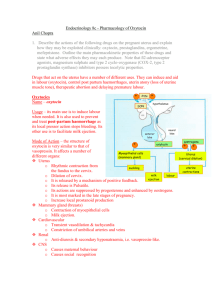
WOMEN AND NEWBORN HEALTH SERVICE King Edward Memorial Hospital CLINICAL GUIDELINES OBSTETRICS & MIDWIFERY INTRAPARTUM CARE INDUCTION OF LABOUR OXYTOCIN INFUSION Keywords: syntocinon infusion, oxytocin infusion, oxytocin induction, labour stimulation, hyperstimulation See Clinical Guidelines, Restricted Area Guidelines (O&M): Induction of Labour (Intranet only) for management prior to commencing an induction of labour. AIM To provide guidance on the use of an oxytocin infusion for labour, including contraindications, dose/dilution, infusion rates, and management of possible complications. KEY POINTS 1. 2. These infusion guidelines are as per the ACOG review October 2010. The maximum infusion rates are as per the RCOG guidelines. 1 ABSOLUTE CONTRAINDICATIONS Any condition in which spontaneous labour is inadvisable 2 or more previous caesarean sections RELATIVE CONTRAINDICATIONS Grande multiparity (> P4) – discuss with the consultant 1 previous caesarean section – discuss with the consultant Secondary arrest in active labour in a multiparous woman – discuss with consultant PRIOR TO COMMENCING OXYTOCIN Oxytocin should not be started for six hours following administration of vaginal 1 prostoglandins. For women with intact membranes an ARM should be performed prior to commencing 1 induction. 1 Establish fetal well-being immediately prior to commencement of oxytocin. Perform a 20-30 minute cardiotocograph (CTG) prior to commencing the induction. Women with a previous uterine scar and / or high parity (greater than 4) should not have oxytocin commenced without discussion with the obstetric team Consultant. Women with a previous caesarean section scar should have discussion and consent to the use of oxytocin. The rupture risk (approximately 1:100) should be explained and this discussion documented in the medical notes. 2014 All guidelines should be read in conjunction with the Disclaimer at the beginning of this section Page 1 of 4 DOSE To reduce error a standard dilution should always be used. Standard Dilution of Oxytocin 10 I.U. of oxytocin in 500mL of Hartmann’s solution. At this dilution, a 3mL/hr infusion rate equates to 1milli-unit (mU) of oxytocin per minute. INFUSION RATE The dose of oxytocin should be titrated against uterine contractions. The aim is to achieve a frequency of one contraction every two and half to three minutes, lasting 60 seconds using the minimum dose of oxytocin possible. Labour Stimulation with Oxytocin Starting Dose Incremental Increase Dosage Interval Increase the infusion Increase the infusion rate by rate at 15 minutely 4 mU per minute (12mL / hr) to a intervals maximum dose of 20 mU per minute (60mL / hr). Once the maximum dose has been running for 30 minutes the Consultant or Senior Registrar should review the woman prior to higher doses being administered. The overall maximum dose of oxytocin should not exceed 36 mU per minute (108mL/hour) 4 mU per minute (12mL / hr). Once an ideal uterine contraction pattern has been achieved, titrate the dose to maintain the pattern. In the case of grande multipara(>Para 4) or a previous caesarean section, the regime may be modified after discussion with the consultant Oxytocin Infusion Conversion Chart Time after starting Oxytocin dose Volume infused (minutes) (mU per minute) (mL per hour) 0 4 12 15 8 24 30 12 36 45 16 48 60 20 60 75 24 72 90 28 84 105 32 96 120 36 108 Doses shaded yellow are above the licensed maximum dose and require Consultant or Senior Registrar review prior to administration. DURING ADMINISTRATION Deliver the oxytocin through an infusion pump and ensure the giving set has a double or triple lumen peripheral set (V-set) attached. Note: The V-Set acts as an anti reflux valve preventing bolus administration of oxytocin. Where the oxytocin infusion is to run as a sideline to a main intravenous line, it should be connected to the main line with a V-Set. Ensure continuous electronic fetal heart rate monitoring and monitoring of uterine contractions throughout the induction using continuous electronic cardiotocography. 2014 All guidelines should be read in conjunction with the Disclaimer at the beginning of this section Page 2 of 4 Place an intrauterine pressure catheter in women whose contractions cannot be adequately assessed by external monitoring or manual palpation. Monitor fluid balance. Ensure constant midwifery support. The woman should have one-on-one midwifery care while 1 have oxytocin infusion. POTENTIAL COMPLICATIONS OF OXYTOCIN INFUSION Complications that may potentially occur with oxytocin use include: Uterine Hyperstimulation 4 4 Hyponatraemia . hypotension 4 nausea and vomiting (infrequent) 5 Rarely – arrhythmias, anaphylactoid reaction 5 UTERINE HYPERSTIMULATION Uterine hyperstimulation from the use of oxytocin or prostaglandins induction of labour occurs in 1-5% 3 of women. Oxytocin has a short half life from 1-5 minutes and is easy to titrate should 6 hyperstimulation occur. Uterine hyperstimulation is defined as: 5 or more contractions in 10 minutes 3, 4 3 contractions lasting more than 90 seconds to 2 minutes. 4 contractions of normal duration occurring within 1 minute of each other. 4 Management of Hyperstimulation with FHR Decelerations or Abnormalities 3, 4 1. CEASE THE OXYTOCIN INFUSION 3 2. Reposition the woman onto her left side. 3. Notify the midwifery Co-ordinator and the Medical Obstetric Team. 4. Consider tocolysis with Terbutaline 0.25mg subcutaneously if cessation of the oxytocic 3 infusion fails to resolve hyperstimulation. A response from Terbutaline should occur within 510 minutes. Note: Terbutaline is contra-indicated in women with cardiac disease. 5. Prepare the woman for immediate vaginal delivery or possible Caesarean delivery if the FHR 3 does not return to normal. 6. If the uterine hyperstimulation resolves, re-start the oxytocin infusion at half the rate of the last 3 dose infused, and increase the rate as required. Management of Uterine Hyperstimulation without Fetal Compromise 4 Decrease the oxytocin infusion rate. If in doubt, cease the oxytocin, reassess the clinical situation and discuss the management with the Medical Obstetric Team. HYPONATRAEMIA Oxytocin is similar in structure to vasopressin and in high doses may cause water retention. With the 4 use of isotonic solutions it is rare. It can occur with prolonged infusions and if hyponatraemia is not recognised can lead to seizures, coma and death. Pulmonary oedema may also occur without 4 hyponatraemia. To reduce the risk of hyponatraemia: 4 Monitor and record fluid intake and output at least 2 hourly during oxytocin infusion. Apply caution with use and careful monitoring of fluid balance for women with cardiac conditions. 7 HYPOTENSION If oxytocin is given as a bolus dose it can cause significant hypotension. Use of infusion pumps prevents this risk. If a rapid injection is given it can cause transient hypotension, flushing and reflex 5 tachycardia. 2014 All guidelines should be read in conjunction with the Disclaimer at the beginning of this section Page 3 of 4 REFERENCES (STANDARDS) 1. 2. Novartis Syntocinon ® Product Information. 2009 McGeown P. Induction of Labour and Post-term Pregnancy. In: Henderson C, MacDonald S, editors. Mayes' Midwifery. 13th ed. London: Bailliere Tindall; 2004. p. 862-75. 3. Thorogood C, Donaldson C. Disturbances in the rhythm of labour. In: Pairman S, Pincombe J, Thorogood C, Tracy S, editors. Midwifery Preparation for Practice. Sydney: Churchill Livingstone; 2006. p. 679-716. Smith JG, Merrill DC. Oxytocin for Induction of Labor. Clinical Obstetrics and Gynecology. 2006;49(3):594-608. 4. 5. 6. 7. 8. Royal Australian College of General Practitioners, Australian Society of Clinical and Experimental Pharmacologists and Toxicologists, Pharmaceutical Society of Australia. Australian Medicines Handbook. Adelaide; 2008. Harman JH, Kim A. Current trends in Cervical Ripening and Labor Induction. American Family Physician. 1999;60(2):477-83. Shiers C. Prolonged Pregnancy and Disorders of Uterine Action. In: Fraser DF, Cooper MA, editors. Myles Textbook for Midwives. 14th ed. London: Churchill Livingstone; 2003. Wei et al.High Dose vs Low Dose Oxytocin for labor augmentation.American Journal of O&G. 2010. National Standards – 4 Medication Safety Legislation – Poison’s Act 1965 Related Policies - Nil Other related documents –KEMH Clinical Guidelines: Obstetrics & Midwifery: Intrapartum Care; Restricted Area Guidelines: Induction of Labour RESPONSIBILITY Policy Sponsor Medical Director OGCCU Initial Endorsement July 2008 Last Reviewed September 2014 Last Amended February 2015 Review date September 2017 Do not keep printed versions of guidelines as currency of information cannot be guaranteed. Access the current version from the WNHS website. 2014 All guidelines should be read in conjunction with the Disclaimer at the beginning of this section Page 4 of 4