Measurement of arterial puls []
advertisement

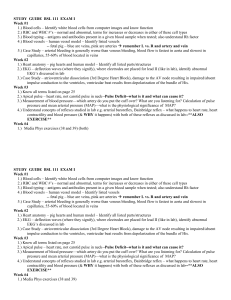
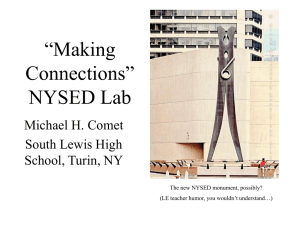
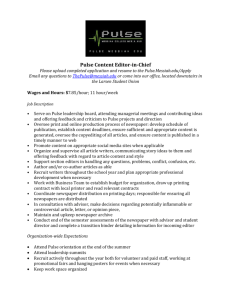
ARTERIAL PULSE Mureșan Simona, Száva Iringó, Orbán-Kis Károly I. THEORETICAL BACKGROUND The arterial pulse is the peripheral expression of the mechanical activity of the heart. It is a wave generated by and synchronous to the ventricular systole. It is transmitted down the aorta and its branches causing the rhythmic expansion of arterial walls. 1. Assessment of the arterial pulse 1.1. By palpation: it is performed by compressing any of the accessible arteries on a solid subjacent plane with three fingers: index, middle, and ring fingers (Figure 1). This method can be applied for: - carotid artery - upper limb: radial artery, ulnar artery, humeral artery, and axillary artery - lower limb: dorsalis pedis artery, posterior tibial artery, popliteal artery, and femoral artery. Pulse palpated at the level of the main branches of the aorta (carotid artery, femoral artery) is the central pulse; by exploring any of the other sites we determine the peripheral pulse. Most frequently, we use the palpation of the radial pulse. No matter which artery is explored, pulse palpation should be done bilaterally, in the same time, in order to check if the pulse waves have the same amplitude and arrive simultaneously to both sides. Thus, we can describe the symmetry and the synchronicity of the pulse wave. Several diseases can cause asymmetrical pulse; one example would be stenosis (abnormal narrowing) of one of the two subclavian arteries. Figure 1. Palpation of the peripheral pulse at the site of the radial artery: press the artery in the radial artery groove using three fingers (index, middle, and ring fingers). 1.2. By graphic recording (sphygmography) – the recording of the pulse wave, obtained with special transducers placed over an artery is called sphygmogram. The arterial pulse can be recorded on large arteries, located close to the heart, (central sphygmogram; when recorded on the carotid artery – carotidogram) or on peripheral muscular arteries (peripheral sphygmograms). The normal aspects and the significance of the central and peripheral sphygmograms are described in the ‘Mechanocardiograms’ chapter. 55 2. Pulse parameters 2.1. Pulse pressure: represents the difference between the systolic (SBP) and the diastolic (DBP) blood pressures. It is directly dependent on the cardiac output and arterial wall elasticity. Its change can be divergent, when SBP increases and DBP decreases, or convergent, when SBP decreases and DBP increases. 2.2. Pulse wave velocity: it is different and higher than the velocity of the blood flow. There is an inverse association between pulse wave velocity and arterial elasticity. Thus, pulse wave velocity increases with age and decreases with the diameter of the vessel. In people with normal arterial wall elasticity, the pulse wave spreads with a speed of: - 3 - 5 m/s in the aorta - 7 - 10 m/s in large arterial branches - 15 - 35 m/s in peripheral, small arteries. 3. Qualities of the pulse wave 3.1. Frequency (pulse rate): represents the number of arterial pulsations counted in one minute and is expressed in beats per minute (bpm). In medical practice, sometimes the pulse will be measured for 30 seconds and the result multiplied by two or counted for 15 seconds and the result multiplied by four. The most precise value is obtained by one minute continuous measurement. In case of arrhythmias, measurement for one minute is compulsory. Normal values for arterial pulse frequency: 60-90 bpm. Pathological values for arterial pulse frequency: - tachycardia: higher than 90 bpm - bradycardia: lower than 60 bpm. 3.2. Rhythm: it is dependent on the interval between two consecutive pulsations. If the intervals between two consecutive pulsations are equal, the pulse is regular (puls regularis); otherwise, the pulse is irregular (puls irregularis). Irregular pulse is usually the hallmark of arrhythmia, which can be intermittent (superimposed on a regular pulse – e.g. extrasystole) or absolute (e.g. atrial fibrillation). Other qualities of the pulse wave that were previously evaluated, but currently are less used: - pulse amplitude (puls magnus – large amplitude or puls parvus – small amplitude) - pulse velocity (puls celer – high velocity or pulse tardus – low velocity) - pulse tension - compressibility (pulse mollis – easily suppressive or pulse durus – hardly suppressive). 4. Pathological aspects of arterial pulse 4.1. Pulse deficit: represents a difference between the number of heartbeats (apical beats or heart sounds) and the number of peripheral arterial pulsations. This occurs when ventricular contractions are too weak to create enough pressure to open the aortic valve, but at the same time enough to close the mitral valve. The absence of a palpable pulse wave at the level of a peripheral artery for one or more heartbeats is often seen in arrhythmias, such as atrial fibrillation (due to the arrhythmia the duration of the diastole is 56 highly variable and often too short to fill properly the left ventricle). Pulse deficit is recorded in medical reports as the number of missing pulse waves (heart rate minus pulse rate per one minute). 4.2. Pulsus alternans: represents the situation when the pulse is regular, but every other pulsation has different amplitude. It is generally associated with severe disturbance of cardiac contractility (e.g. left ventricular failure). II. EXPERIMENTAL OBJECTIVES AND PROCEDURES 1. Experimental objectives to find the pulse over different arteries (carotid artery, brachial artery, radial artery, ulnar artery, posterior tibial artery, dorsalis pedis artery) to measure the pulse rate of all students at the level of the radial artery to measure the pulse rate in at least two subjects under different circumstances (standing, sitting, supine) to evaluate if the pulse is regular/irregular to become familiar with the principle of plethysmography and its usefulness in qualitatively assessing peripheral changes in blood volume to observe and record changes in peripheral blood volume and pressure pulse under a variety of experimental and physiological conditions to determine the approximate speed of the pulse wave traveling between the heart and the finger to illustrate the electrical activity associated with normal cardiac activity and how it relates to the flow of blood throughout the body. 2. Materials for manual pulse rate measurement: watch or stopwatch (analog or digital) for recording plethysmography: BIOPAC recording system (BIOPAC data acquisition unit connected to a computer) transducers for recording ECG (SS2L) and pulse (SS4L) measuring tape, ice water in plastic bucket 3. Experimental methods 3.1. Manual measurement of pulse rate A.1. Students should form pairs. Find the pulse at the carotid artery, brachial artery, radial artery, ulnar artery, posterior tibial artery, and dorsalis pedis artery. Check both right and left side simultaneously. Switch places so that everybody palpates the pulse. Do not take the carotid pulse bilaterally at the same time! Avoid taking the carotid pulse for more than 15 seconds! Avoid massaging the carotid region when taking the pulse! A.2. Measure the pulse rate of all students in the class. All measurements should be done in sitting position, at the level of the right radial artery, for one minute. Complete the tasks in the corresponding section of the Worksheet. 57 A.3. Measure the pulse rate in two different subjects in standing, sitting, and supine positions. All measurements should be done at the level of the right radial artery, for one minute. Complete the tasks in the corresponding section of the Worksheet. 3.2. Recording of ECG and pulse During this recording the BIOPAC system will be used to record simultaneously the ECG (Lead II) and pulse plethysmography. The recording system will be set up by lab assistants. In order to record, the transducers must be connected according to Figure 2. Figure 2. The electrode cable for Lead II must be connected to Channel I; electrodes will be placed on both lower limbs and right upper limb: red to left leg (positive), white to right arm (negative) and black to right leg (ground). The pulse transducer will be connected to Channel II of the system with the sensor on the tip of the right index finger (snug but not too tight – it must not obstruct the flow of blood). After connecting the transducers follow the lead of the lab assistant who will guide you through the necessary steps of the recording. For a proper recording subject must be seated in a relaxed fashion, always facing away from the monitor. B.1. Record with the subject seated and relaxed, arms supported, breathing normally, facing away from the monitor. Suspend the recording after approximately 15 seconds. The recording should look like Figure 3. Figure 3. Two-channel recording: top trace ECG, bottom trace pulse plethysmography. 58 B.2. The subject remains seated and relaxed, facing away from the monitor. Put the subject’s left (non-recording) hand into a plastic bucket filled with cold water (around 20°C). Recording should start immediately as the subject stopped moving. Suspend the recording after approximately 30 seconds. B.3. The subject remains seated, relaxed, facing away from the monitor. If cold water was used, wait for the subject’s hand to return to normal temperature before continuing. The subject raises his/her right hand above the head, arm extended, pulse transducer attached. Recording should start immediately as the subject stopped moving. Suspend the recording after approximately 60 seconds. Review your data. Complete the tasks in the corresponding section of the Worksheet. 59 TEST YOUR KNOWLEDGE 1. The pulse pressure: a. represents the difference between the systolic and diastolic blood pressures b. is directly dependent on the arterial wall elastic properties c. is directly dependent on the venous return d. represents the number of arterial pulsations counted in one minute e. if SBP increases and DBP decreases, the pulse pressure is convergent 2. The pulse deficit: a. represents a numeric difference between the number of heartbeats and the number of peripheral arterial pulsations b. depends on myocardial contractility c. can be associated with right ventricular failure d. can occur even if the pulse rhythm is regular e. represents the numeric difference between the systolic and diastolic blood pressure 3. If the heart rate is 110 bpm and the peripheral arterial pulse 100 bpm, calculate the pulse deficit. _____________________________________________________________________________ _____________________________________________________________________________ _____________________________________________________________________________ _____________________________________________________________________________ 4. If the heart rate is 120 bpm and the calculated pulse deficit is 15 bpm, the pulse frequency measured at the radial artery is: _____________________________________________________________________________ _____________________________________________________________________________ 60