Lung tox 1 - Learnblock
advertisement

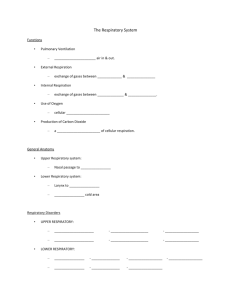
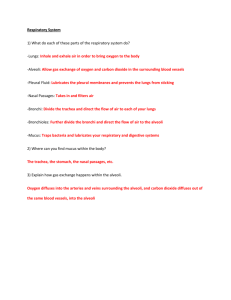
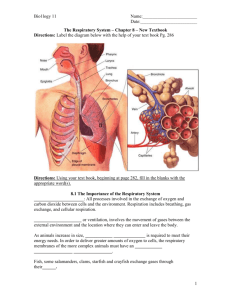
4/15/10 Respiratory Toxicology 1 J Paul Seale MB BS PhD FRACP Professor of Clinical Pharmacology COMMONWEALTH OF AUSTRALIA Copyright Regulation WARNING This material has been reproduced and communicated to you by or on behalf of the University of Sydney pursuant to Part VB of the Copyright Act 1968 (the Act). The material in this communication may be subject to copyright under the Act. Any further reproduction or communication of this material by you may be the subject of copyright protection under the Act. Do not remove this notice Outline of 2 lectures • • • • The respiratory system as a target organ The anatomy & structure / function Host defence : mucus & muco-ciliary clearance Vulnerable cell types – & their pathological responses • Damage to lung cells – Chemical – immunological • Disease states Respiratory system as target organ • in contact with external environment Respiratory system & inhaled toxins : 2 categories of effects • Local effects – Nasal – Upper airways : larynx/trachea – Lower airways & alveoli – all the way from nostrils to alveoli • samples a large volume of air – >10,000 L per day • has defense system • Distant effects – toxin absorbed into the body – toxic effects on “distant organs” (e.g. CO) – but can be over ridden Anatomy : Respiratory Tract Respiratory system & injury • Injury to the lungs can occur via Naso-pharynx Nasal cavity – inhaled toxins – toxins in the blood (e.g. paraquat) pharynx Larynx “voice box” Airways Trachea “windpipe” Alveoli “gas exchanging units” 1 4/15/10 CT scan of nasal cavity Nasal cavity Middle turbinate (MT) Inferior turbinate Uvula (U) - soft palate Nasal breathing Mouth breathing tongue • Showing maxillary sinuses F. Netter Textbook of Human Anatomy from "Respiratory Specialists Slide Set" Thryoid cartilage Cricoid cartilage Nasal function ~27 generations of asymmetrically branching airways Generation 1 • Air-conditioner of inhaled air – heats air – humidifies air Trachea Longitudinal mucosal folds • Filter – captures large particles • Captures water soluble gases • Nasal epithelium has cytochrome P450s bronchi Right upper lobe Left upper lobe – 1A1, 2B1, 4B1 in several species Right lower lobe Left lower lobe Bronchi Bronchioles Acinus education.vetmed.vt.edu/.../labs/Lab25/lab25.htm Dr Thomas Caceci, VM8054: Veterinary Histology. Dept. of Biomedical Sciences & Pathobiology, Virginia-Maryland Regional College of Veterinary Medicine, Blacksburg, VA 2 4/15/10 Bronchioles and alveoli Alveolar spaces Trachea Bronchi Bronchioles (<1mm diameter, no cartilage in walls) alveoli (terminal sacs) Alveolar septum SPACE Photograph courtesy of Prof M Saetta Moore, K.L. & Dalley, A.F.. 2003, Clinically Oriented Anatomy, Instructor’s resource DVD ROM 5th Edn, Lippincott Williams and Wilkins, Philadelphia. O2 Interstitial cell Epithelial Cell: Type 1 CO2 Alveoli cells • Type 1 cells: line the airspaces • Type II cells : located in corner of alveoli – Produce surfactant – Transform into Type 1 cells if necessary ENDOTHELIUM Endothelial cell • E.g. if Type 1 cells are damaged nucleus Type II cell Mucus • Where does it come from ? – Goblet cells – Mucous glands Lamella body • What does it do ? – host defense mitochondria 3 4/15/10 Respiratory mucosa Mucociliary system cilia Goblet cell ? Direction of flow Mucus Cilia Ciliated Cell Ciliated Cell periciliary fluid layer Goblet Cell basement membrane Submucosal glands submucosa Direction of flow Direction of mucociliary flow : nasal cavity • Nose : backwards • Trachea & lower airways : Upwards • To nasopharynx VISUALISATION swallowed Mucociliary clearance : lung Clearance is “upwards” Dye in oropharynx at peak intensity 4 4/15/10 Mucus • From goblet cells & mucous glands • Traps pollutants & debris (physical properties) • Other properties – Anti-oxidant – Acid neutralising – Free radical scavanging Measuring muco-ciliary clearance • Patient inhales radiolabelled particles • counter continuously records emission • Segment into “areas of interest” peripheral central Measuring muco-ciliary clearance Damage from inhaled noxious agents # ## Intervention Colonization with bacteria, virus and besides impairment of the mucociliary-clearance Inflammation (Neutrophils) Cardinal symptoms: cough, sputum and (micro-) infections. Respiratory Clearance • Nasal – Anterior : wiping / blowing – Posterior ; muco-ciliary • Tracheobronchial : mucociliary – trapped in mucus – phagocytosed by macrophages ----> mucus • Pulmonary- peripheral – phagocytosed by alveolar macrophages ---> lymph drainage • via lymph nodes – Dissolve from surface of particles & enters • lymphatics OR • blood Vulnerable cells & damage • Particle size determines site of deposition – Large particles in upper airways – Small particles reach small airways / alveoli (distal lung) – Gases can cause damage along the entire tract • And may be absorbed (affecting distant organs) • Site of deposition will determine which cells are at risk of damage 5 4/15/10 Mechanisms for deposition • Interception – particle trajectory brings it contact with airway epithelium (Large airways) PARTICLE DEPOSITION • Sedimentation – as flow diminishes gravity leads to sedimentation(small airways) trachea Very abrupt bronchi bronchioli 1-5 μm less abrupt + Effective deposition Leach CL, et al. [REF T/C] Vulnerable cells : damage by chemicals – mediated by oxygen free radicals generated by : • ozone • nitrogen dioxide • tobacco smoke – also from lung defense cells • neutrophils, monocytes, macrophages 0 -labelled particles : lung deposition Large particles Small particles • Oxidative burden ++ Periphery /Alveoli 1 μm diffusion 99Tc ++++ +++ mild – No flow (alveoli) (HFA propellant, radiolabelled) interception/ impaction sedimentation • Diffusion Deposition of inhaled Airflow Directional change • Impaction – at sites of airway bifurcation (large airways) Particle size Naso-pharynx 5-30 μm Ineffective deposition Lung defense cells • Convert molecular oxygen to : – Reactive oxygen species (ROS) • ROS are part of host defense O2 ----> ROS Kill microbes (host defence) “appropriate” If “excessive” ----> lung damage 6 4/15/10 Immune System Basics Vulnerable cells : immunological damage Response phases Cell Number • Immune response is part of host response – Humoral (antibodies) – Cell mediated (T lymphocytes) • Normal cells can be affected – “collateral damage” Reprinted from: Abbas & Lichtman, “Phases of adaptive immune response” Cellular and Molecular Immunology, 2005 L Toxicity of inhaled gases : site of injury depends on water solubility Highly soluble (e.g. SO2) -captured in nasal fluid - not very toxic Relatively water insoluble (e.g Ozone, NO2 ) -penetrate deep into lung - small airway/alveolar damage 38 Lung toxicology 1 : summary • Respiratory tract in contact with external environment ; vulnerable – also at risk from some blood born substances • Well developed host defense Very water insoluble (e.g.CO ) - reach alveoli – But this can be depleted or overwhelmed • Damage can occur via : binds to haemoglobin – Particles, gases, or mis-directed immune response blood Tissue hypoxia 7