Effect of the pH and the Importance of the Internal Standard

Technical note
Eur J Clin Chem Clin Biochem
1995; 33:873-875
© 1995 Walter de Gruyter & Co.
Berlin · New York
TECHNICAL NOTE
Effect of the pH and the Importance of the Internal Standard on the
Measurement of the Urinary Catecholamines by
High-Performance Liquid Chromatography
By Adriana Rivero-Marcotegui, Ana Grijalba-Uche, Mercedes Palacios-Sarrasqueta and Sergio Garcia-Merlo
Departamento de Bioquimica Clinica, Hospital de Navarra, Pamplona, Navarra, Spain
(Received May 5/July 7, 1995)
873
Summary: Clinical manifestations of phaeochromocytoma are not always sufficient for its early diagnosis. It is therefore necessary to confirm hypersecretion of catecholamines. Current methods for the measurement of catecholamines are based on their oxidative properties, and the majority of the laboratories often use HPLC methods for catecholamine testing. However, the extraction procedures used for the biogenic amines differ. We use a method of ion-exchange chromatography which is performed at pH6.5. In order to avoid the spontaneous oxidation of the catecholamines, the urine sample has to be collected on HC1, which gives a pH of approximately 2. Occasionally, the acidified urine «ample has a pH less than 1 requiring the addition of NaOH to reach a pH of 6.5, necessary for the adsorption of catecholamines on cation exchanger resins, liiis phenomenon produces a decrease in the peak areas but the use of an internal standard allows the final results to be corrected.
interpretable chromatogram with well-resolved and undistorted peaks.
Materials and Methods
Chromatographie conditions
The HPLC System consisted of an Autosampler 465, a Pump 420
(Kontron Instruments, USA), a Coulochem II detector, an Analytical Cell, a Guard Cell (ESA, Beldford, USA), controlled by a Data
System 450 (Kontron Instruments, USA). The column was a
LiChrospher 100 RP-18 packed with 5 μπι particles (Merck, Darmstadt, Germany). Catecholamines were detected after their oxidation and reduction at + 300 mV and —250 mV, respectively, following separation at a flow rate of 1.5 ml/min of mobile phase solution (CAT-A-PHASE, ESA, Belford, USA).
Introduction
The measurement of catecholamines in urine is useful for assessment of neural function and diagnosis of phaeochromocytoma and neuroblastoma (1, 2). Although the incidence of phaeochromocytoma remains low (<1%), it constitutes a rare but curable cause of hypertension (3).
Early diagnosis is essential because the tumoral release of catechoL· amines can be lethal for patients suffering from this disease.
Phaeochromocytoma can not be confirmed solely by clinical manifestations, so catecholamine hypersecretion must be demonstrated.
Recently, we have seen important advances in the understanding of catecholamine metabolism, in part due to a progressive change toward more sensitive and specific laboratory methods that ensure adequate removal of interfering compounds with elution profiles similar to those of the catecholamines. Currently, the quantification of urinary catecholamines by HPLC appears to be the method of choice (4). Electrochemical detection with ion-pairing adaptation of reversed-phase chromatography is the most common methodology (5). Detection is performed after a one step sample preparation on a cation-exchanger resin (6).
We have shown the great importance of the internal standard as well as of the pH of the urine and the resin, in obtaining an easily
Procedures
Specimen collection and analysis of samples
Urine specimens (24 h) were collected in a container with 25 ml of 6 mol/1 HC1 as preservative, and stored at -20 °C until assayed.
The catecholamines are extracted by using a weak-cation exchanger (Biorex 70) (BioRad, Richmond, USA), which provides a great selectivity (7). The resin had been previously adjusted to pH
6.5 with glacial acetic acid (Merck, Darmstadt, Germany) according to Shandu (8). After the resin pH stabilized, it was washed 4-5 times with de-ionized water.
Free catecholamines are extracted by the following method: Pipet
5 ml aliquot of an acidified 24 h urine specimen into a test tube.
Add 1 ml Na
2
EDTA · H
2
O (29.8 mmol/1) (Merck, Darmstadt, Germany) and 100 μΐ of internal standard (3,4-dihydroxybenzylamine,
17.9 μτηοΐ/ΐ) (ESA, Beldford, USA) and 7ml of distilled water.
Adjust the pH to 6.5 with 1 mol/1 NaOH and again add water to
20 ml. Apply 2 ml of the sample mixture to the weak-cation exchange resin column (100 mg of Bio-Rex 70, adjusted at pH 6.5
previously) for 10 min, allow to drain completely and discard the eluate. Elute the catecholamines from the column into a clean tube by adding 2 ml of boric acid (0.64 molA) (Merck, Darmstadt, Germany) and inject 50 μΐ into the Chromatograph. It is important that
Eur J Clin Chem Clin Biochem 1995; 33 (No 11)
874 Technical note the resin column be washed with 2 mj of water after each step of the technique.
To prepare a standard sample, add 100 μΐ of the catecholamine standard (noradrenaline: 14.77 μπιοΐ/l, adrenaline: 13.64 μιηοΐ/ΐ, dopamine: 16.32 μηιοΐ/ΐ) (ESA, Beldford, USA) to 7ml of water and 1 ml of Na
2
EDTA · H
2
0 (29.8 mmol/1). Treat this in the same way as the urine samples and use it as a calibration mixture.
Effect ofthepH of the urine
To check the importance of the pH of the samples we analysed the catecholamines of a urine sample at pH 2. Then, we adjusted the pH to 0.5 with HC1, and measured the catecholamines as well.
We also prepared a solution of NaCl (6.8 mol/1) which was added to a urine sample to give a final concentration of 310, 620, and
1240 mmol/1 with the objective of veryfying the effect this compound has on the area peaks.
chromatograms are apparent. The aliquot at pH 0.5 yielded smaller peaks than the aliquot at pH2 (fig. I). Table 1 shows the results of the catecholamines in the two aiiquots. This phenomenon always occurs when the pH of the acidified urine is below 1. In order to confirm that this effect was due to the formation of NaCl, we analysed a sample with an original pH of 2 after adding various volumes of NaCl (fig. 2). We subsequently extracted the catecholamines as previously described. Figure 2 shows that the addition of
310 mmol/1 of NaCl produces a significan't decrease in catecholamine peak height and area. No detectable differences were observed after the addition of 310 mmol/1 NaCl as compared to 620 mmol/1
NaCl. The addition of NaCl consistently led to the disappearance of adrenaline.
Otherwise, an increase of resin pH produces a peak splitting (fig.
3) in noradrenaline, adrenaline and dihydroxybenzylamine but not in the dopamine peak.
Effect of the pH of the resin
In order to study the resin pH effect on the extraction of catecholamines, we adjusted an aliquot of resin at three different pH values
(4, 6.5 and 10) with glacial acetic acid or NaOH (1 mol/1)
(Pancreac, Barcelona, Spain).
Results
We extracted the catecholamines of two aliquots of a urine sample, one at pH 2 and the other at pH O.5. The differences between both
Discussion
Urinary catecholamines represent a quantitatively small but diagnostically important component of excretion products. As with plasma, the unconjugated fraction is less affected by diet (9). The diagnostic sensitivity is equivalent for total and free catecholamines (4). Therefore we chose to quantify free catecholamines which do not require a hydrolysis step, resulting in a shorter procedure.
For the determination of urinary catecholamines, urine must be collected under HC1 to avoid spontaneous oxidation (10). The majority of urine samples received in our laboratory have a pH between 1.5 and 2.5, but are occasionally near pH O.5. For this reason, a larger volume of NaOH is required to reach pH 6.5. In these
540.08
Dopamine
.§ 3Β0.ΒΘ-
I <D
>
2ΘΒ.ΒΒ-
Noradrenaline
• ll Adrenaline/,
Θ.48 LS8
Fig. 1 Chromatograms obtained from two aliquots of a urine sample at pH 2 (—) and 0.5 (—) under conditions (sensitivity: 100 nA) stated in the text.
β.40 2,09 i,80 6.8θ 8.88 IB.
t [min]
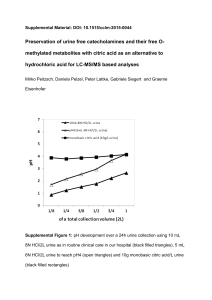
Fig. 2 Effect of the addition of NaCl (·: original urine; x: urine with NaCl to obtain a final concentration of 310 mmol/1 NaCl; D: urine with NaCl to obtain a final concentration of .620 mmol/1
NaCl; A: urine with NaCl to obtain a final concentration of 1240 mmol/1 NaCl).
Tab. 1 Results of the catecholamines (nmol/24 h) extracted from two urine sample aliquots at different pH values, with and without inclusion of the internal standard in the calculation of the results.
Urine pH 2, with internal standard
Urine pH 0.5, with internal standard
Noradrenaline
Adrenaline
Dopamine
216.34
20.19
2448.00
242.35
20.19
2565.50
Urine. pH 0.5, without internal standard
108.17
8.73
1142.40
Eur J Clin Chem Clin Bioehem 1995; 33 (No 11)
Technical note 875
8. -
Fig. 3 Effect of resin pH on the peaks. The BioRex 70 was adjusted to pH 10 instead of 6.5 with 1 mol/1 NaOH. The extraction of the catecholamines was performed as described in Material and
Methods. No differences were observed when the resin was adjusted to pH 4 and pH 6.5.
cases, we obtain a poor quality chromatogram (fig. 1) and this frequently involves the repetition of the analysis and associated testing delays.
On the other hand, the addition of large volumes of NaCl produces smaller peaks (fig. 2). By adding a greater volume of NaCl, the peak height and area become smaller. This is probably a result of increased ionic strength in the sample. Decrease of catecholamines peaks could be due to stronger retention on the weak cation exchanger or could more likely result from the urine sample. On the other hand, in a bonded reversed-phase column, an increase in ionic strength of the sample would increase its polarity, decreasing retention time but not peak areas.
We considered the possibility that this fact could hide a possible phaeochromocytoma, yielding false negative results. We chromatographed a urine sample (pH 1.96) from a patient diagnosed as having phaeochromocytoma, and also after adding HC1
(6 mol/1) to the urine sample until a pH of 0.6 was obtained. A chromatogram with smaller peaks was obtained (data not shown), but the results were equivalent when normalised using the internal standard, as stable 1 shows for another urine sample. If we had not included the internal standard, the results would have been about 50% of the real results (tab. 1). The acknowledgement of this phenomenon should avoid an unnecessary repetition of the analysis. Diagnostically, however, this problem is not serious, because it does not produce false negative results provided that the internal standard is taken into account. According to this finding, it is important to take care with the collection of urine samples as preanalytical steps are of great importance to obtain an optimum result.
On the other hand, we have studied the influence of the pH of the resin on the extraction of the catecholamines. The retention of the catecholamines on a weak cation-exchanger is performed at pH 6.5
(11) being careful not to exceed this pH. The pH of our resin, was adjusted to p H 6.5, tended to increase spontaneously. We think that this phenomenon was produced by contact with NH^ in the environment. The pH increase of the resin produced a peak splitting (fig. 3). Thereafter, we removed an aliquot of resin and kept the pool perfectly closed. From time to time, the pH of the resin was measured. Degel (12) studied the effect of the pH of the sample injected into the chromatogram and obtained a single and undistorted peak from each catecholamine at pH from 3.6 to 6.5, but a distorted peak at pH 7.5 and 8.5. We obtained a similar result.
At pH > 6.5 the resin is less negatively charged and its interaction with the catecholamines could be weaker or could form different complexes giving distortions of the catecholamine peaks. According to Degel (12) catecholamines may be present in two or more forms and during the Chromatographie separation and changes in equilibrium are observed between the complexed and free catecholamines.
To summarize, these findings clearly indicate the importance of pH in the determination of urinary catecholamines.
References
1. Bravo EL, Gifford RW. Pheochromocytoma diagnosis, localization and management. N England J Med 1984; 311:1298-
303.
2. Maas JW. Biogenic amines and depression. Arch Gen Psychiatry 1975; 32:1357-61.
3. Samaan NA, Rickey RC, Shutts PE. Diagnosis localization and management of pheochromocytoma, pitfalls and follow up in 41 patients. Cancer 1988; 62:2451-60.
4. Peyrin L, Momex R. Le diagnostic biologique du pheochromocytome. U impact de revolution technologique. Ann Biol Clin
1992; 50:835-65.
5. Lee BL, Chia SK, Orig CN- Measurement of urinary free catecholamines using high performance liquid chromatography with electrochemical detection. J Chromatogr 1984;
494:303-9.
6. Chan YP, Siu S. Simultaneous quantitation of catecholamines and o-methylated metabolites in urine by isocratic ion-pairing high-performance liquid chromatography with araperometric detection. J Chromatogr 1988; 459:251-60.
7. Bauersfeld W, Diener U, Ratge D, Knoll E, Wisser H. Untersuchungen zur Spezifität der Vortrennung der Catecholamine mit
Borsäuregel und einem schwachen Ionenaustauscher. Fresenius Z Anal Chem 1982; 311:436-7.
8. Shandhu RS, Freed RM. Catecholamines and associated metabolites in human urine. In: Cooper GR, Annino JS, Faulkner
WR, MacDonald RP, Mather A, editors. Standard methods of
Clinical Chemistry. London: Academic Press Inc.,
1972:231-46.
9. Moleman P. Effect of diet on urinary excretion of unconjugated catecholamines and some of their metabolites in healthy control subjects and depressed patients. Clin Chim Acta 1990;
189:19-24.
10. Giles HG, Meggirini S. Stability of catecholamines in urine.
Clin Chem 1983; 29:595.
11. Parker NC, Levtzow CB, Wright PW, Woodard LL, Chapman
JF. Uniform chromatography conditions for quantifying urinary catecholamines, metanephrines, vanillylmandelic acid, 5hydroxyindolacetic acid by liquid chromatography with electrochemical detection. Clin Chem 1986; 32:1473-6.
12. Degel F, Zuman P, Jandik P, Gilch G. Effect of pretreating samples with boric acid before liquid-chromatographic determination of urinary catecholamines. Clin Chem 1987;
33:108-12.
A. Rivero-Marcotegui
Departamento of Bioquimica Clinica
Hospital de Navarra c/Irunlarrea 3
E-31008 Pamplona (Navarra)
Spain
Eur J Clin Chem Clin Biochem 1995; 33 (No 11)