Full Text - Laboratory Medicine
advertisement

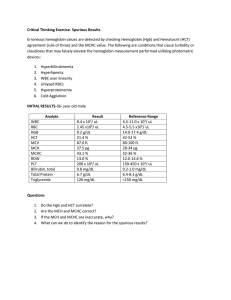
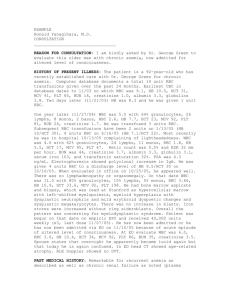
Ask the Experts Inconsistent Relationship Between Hemoglobin and Hematocrit An inconsistent relationship between hemoglobin (HGB) and hematocrit (HCT) is a common clue to the presence of analytic artifact in an individual patient's CBC count results. Technologists should always be alert for violations of the "rules of three and nine": Relationship RBC x 9 = HCT RBC x 3 = HGB HGB x 3 = HCT Patient's Values Expected Observed 33.5 29.4 9.6 7.7 23.1 29.4 The laboratory seems to have considered several common reasons for hemoglobin/hematocrit inconsistency, only some of which could be possible in the situation described in Ms Kling's letter. Lipemia or jaundice spuriously elevates the hemoglobin level and produces an HCT/HGB ratio of less than 3:1 rather than the high ratio of 3.8:1 observed by Kling. Cryoglobulins and leukocyte fragments could have falsely elevated the red cell count, but these causes were excluded. One primary measurement was rechecked by an alternate method. The spun hematocrit was 24%, suggesting that the original hemoglobin value was also correct (24/3 = 8). If this is so, the original red count or MCV must have been falsely increased (Coulter HCT = MCV x RBC). Most of the common causes for elevated MCV were excluded, as Kling indicated. Autoagglutinins would be seen on the smear, and in any case, the HCT/HGB ratio would be low, not high. Hyperglycemic osmotic matrix effects that produce swelling of the red cells in diluent is a possibility, but the "correct" MCV 8 6 8 LABORATORY MEDICINE • VOL. 18, NO. 12, DECEMBER 1987 in this situation, from the data described, would be expected to be about 65 fL. Van Voolen and co-workers indicated a 5-fL MCV increase occurs for every 1,000-mg/ dL increase in glucose at 37 °C, suggesting that the patient's glucose level would have been about 3,000 mg/dL. I suspect the laboratory would have noted this if it had occurred. Occasionally, the red count can be elevated by small particulates such as microdots or air bubbles in the aspiration lines. If such particles are small enough, they will be gated in as red cell sized by the analyzer. Debris seems to be a special problem in CBCs from dialysis units. The following is a CBC count from a dialysis patient with a pattern similar to that reported by Kling: WBC RBC HGB HCT MCV MCH MCHC RDW 3.6 x 109/L 4.11 x 1012/L 6.1 g/dL— 28.2 %—HCT/HGB ratio 3.6:1 68.6 fL 14.8 pg 21.5 g/dL 20.5 units Verification showed that the hemoglobin level was correct, and the spun HCT was 19.9%. There were no grossly observable clots in the EDTA tube. Tiny bubbles can be introduced into the sample lines by briefly withdrawing the sample aspirator tip from the blood during aspiration and then reinserting it. Experimental counts 1 and 2 are replicates; count 3 was produced from the same tube by withdrawing and reinserting the blood. WBC RBC HGB HCT MCV MCH MCHC 1 6.8 4.83 14.1 42.7 88.4 29.3 33.1 2 6.9 4.85 14.0 42.7 88 28.9 32.9 3 0.6 1.63 1.5 14.2 87.3 9.0 10.4 The WBC count and hemoglobin level fell to a tenth of their original values; the red count decreased only by twothirds. The instrument, a Coulter S + II, was apparently counting small bubbles as red cells, producing the absurd values for MCH and MCHC. I suspect that the results reported by Kling were due to bubbles or microdots, but this cannot be proven after the fact. In such a situation, results violating the expected relationships between interdependent parameters should not be released before rechecking at least one and preferably two of the primary measurements—RBC, HCT, and HGB—by an alternate method. Releasing data after rechecking on the original analyzer is not sufficient, as Ms Kling found out. Richard A. Savage, MD Ashtabula County Medical Center Ashtabula, Ohio Downloaded from http://labmed.oxfordjournals.org/ by guest on March 4, 2016 Our institution is currently using the Coulter S550 for CBC counts. Recently a technologist sent out the following values: 15.4 WBC 3 Bands + 3 Hypochromic 3.72 RBC 87 Polys +2 Anisocytosis 7.7 HGB 10 Lymphs +2 Poikilocytosis 29.4 HCT +2 Polychromatophilia 79 MCV +1 Macrocytes + Target Cells Platelet Count 295,000 The technologist repeated her work and accepted the results as correct in view of the very high red count. The physician was very critical of her work because the H&H did not match. The technologist then did a 'spun hematocrit' with 24% as the reported result. Interference by lipemia, an elevated white count, and cryoglobulins were ruled out. Which hematocrit is correct? Gail Kling, MT(ASCP)BB Peekskill Community Hospital Peekskill, NY